Page 9 of 17
OG11.1 | Multiple Pregnancy — SDL Guide
Learning Objectives
- Describe the aetiology and classification of multiple pregnancy by zygosity and chorionicity
- Explain how chorionicity is determined by first-trimester ultrasound and why it is the key prognostic determinant
- Enumerate the maternal and fetal complications specific to multiple pregnancy
- Describe the Quintero staging system for twin-to-twin transfusion syndrome (TTTS) and its management
- Outline the principles of antenatal surveillance and delivery planning, stratified by chorionicity
INSTRUCTIONS
Multiple pregnancy is associated with significantly higher rates of maternal and fetal complications compared to singleton pregnancies, and its incidence is rising worldwide due to assisted reproductive technology. Understanding the pathophysiology of chorionicity-dependent complications — particularly twin-to-twin transfusion syndrome — and the evidence-based surveillance schedules is essential for any obstetrician managing these high-risk pregnancies.
References
- DC Dutta's Textbook of Obstetrics, 9th edition, Ch 17 — Multiple Pregnancy (textbook)
- Williams Obstetrics, 26th edition, Ch 45 — Multifetal Pregnancy (textbook)
- NICE Guideline NG137: Twin and triplet pregnancy (2019) (guideline)
- Senat MV et al. Endoscopic laser surgery versus serial amnioreduction for severe twin-to-twin transfusion syndrome. NEJM 2004;351:136–44. (trial)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Mrs Priya, 28 years old, has been trying to conceive for three years and underwent IVF with two embryos transferred. At her first antenatal visit at 10 weeks, the USS report reads: 'Twin pregnancy; two chorionic sacs visible; lambda sign at the inter-twin membrane.' Her obstetrician tells her this is excellent news — 'the safest type of twins' — and explains why. At her 20-week scan, a second patient, Mrs Lakshmi, also carrying twins, has an inter-twin membrane with a T-sign, no lambda. The obstetrician's tone changes: a much closer surveillance schedule is booked. Why does the same diagnosis — twin pregnancy — carry such different implications for these two women?
WHY THIS MATTERS
Multiple pregnancy incidence has more than doubled in high-income countries over the past three decades, driven primarily by assisted reproductive technology. In India, the incidence of twins is approximately 1 in 80–90 pregnancies (naturally higher in African populations due to DZ twinning rates). Multiple pregnancies account for a disproportionate share of perinatal morbidity and mortality: twins carry 5–6 times the perinatal mortality risk of singletons, primarily due to prematurity, growth restriction, and the unique complications of monochorionic placentation. As a final-year student, you will encounter multiple pregnancies in antenatal clinics, labour ward, and theatre — recognising chorionicity at booking and acting on its implications is a non-negotiable clinical skill.
RECALL
Recall from your embryology module that fertilisation normally produces a single zygote that implants in the uterine endometrium. In multiple pregnancy, either more than one egg is fertilised (dizygotic, the common twin type) or a single fertilised egg splits (monozygotic). The chorionic villi form the placental structure and are derived from trophoblast (extra-embryonic); the amnion is the inner membrane enclosing the amniotic fluid and the fetus. Both of these membrane types are relevant to understanding twin placentation. Also recall that the human placenta is normally a single organ; in monochorionic twins, the two fetuses share one placenta — a situation that creates vascular communications between the two circulations, with potentially serious consequences.
Introduction and Epidemiology of Multiple Pregnancy
Multiple pregnancy refers to the simultaneous development of more than one fetus in the uterus. The vast majority are twin pregnancies (approximately 1 in 80 natural conceptions in India); triplet and higher-order multiples are rarer but carry even greater risks. The incidence of multiple pregnancies is rising globally. The primary driver of this increase is the widespread use of assisted reproductive technology (ART) — both ovulation induction (which promotes multifollicular development and dizygotic twinning) and in vitro fertilisation with multiple embryo transfer. Clomiphene citrate, used extensively in India for ovulation induction, carries a 6–8% twin rate. IVF with double embryo transfer historically resulted in 25–30% twin pregnancies; modern single-embryo-transfer policies are reducing this but multiple pregnancies from ART remain common.
From the initial clinical presentation, multiple pregnancy may be suspected when:
- The uterine size is large for dates — the uterus measures significantly larger than expected for gestational age on abdominal palpation.
- There are hyperemesis symptoms disproportionate to gestational age (higher hCG in multiple pregnancy).
- The patient reports family history of twins, or has undergone ART.
- On abdominal palpation, multiple fetal parts are felt and more than one fetal pole is identified.
- Two fetal heart rates are heard simultaneously at different sites.
However, clinical diagnosis is unreliable — ultrasonography is the definitive method for diagnosing multiple pregnancy and must be performed routinely at the first-trimester scan (11–14 weeks). At this scan, the number of embryos, the number of chorionic sacs, the inter-twin membrane appearance, and fetal viability are assessed. This early USS is the critical window for determining chorionicity — the most important prognostic factor in multiple pregnancy.
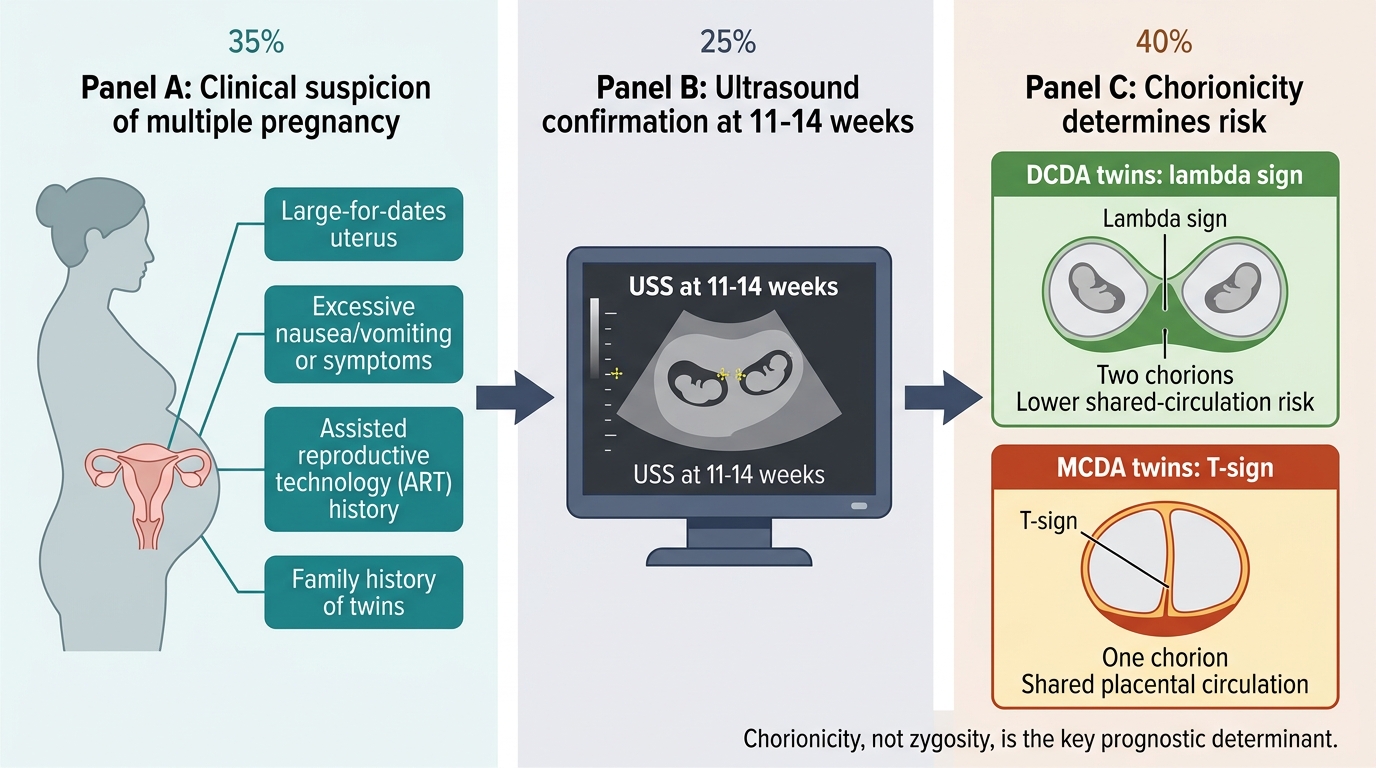
Clinical Suspicion and Ultrasound Chorionicity in Multiple Pregnancy
Aetiology, Zygosity, and Chorionicity
Understanding the origin of multiple pregnancy — whether from one or two fertilised eggs — and the precise timing of embryonic splitting in monozygotic twins are the two conceptual keys that unlock the entire clinical risk stratification of twin pregnancy. Once these are understood, every complication, every surveillance schedule, and every delivery planning decision follows logically from first principles. Chorionicity (the number of chorions, which determines the number of placentas) is the single most important prognostic determinant in twin pregnancy, because it governs whether the two fetal circulations share a common placental vasculature — a shared circulation that creates the unique and potentially lethal complications of monochorionic placentation. Zygosity (identical vs fraternal), while clinically intuitive, does not determine risk; two monozygotic (identical) twins who split early and are DCDA have a safer pregnancy than two different-sex (clearly dizygotic) monochorionic twins — an apparent paradox that reflects the primacy of placental anatomy over genetic identity.
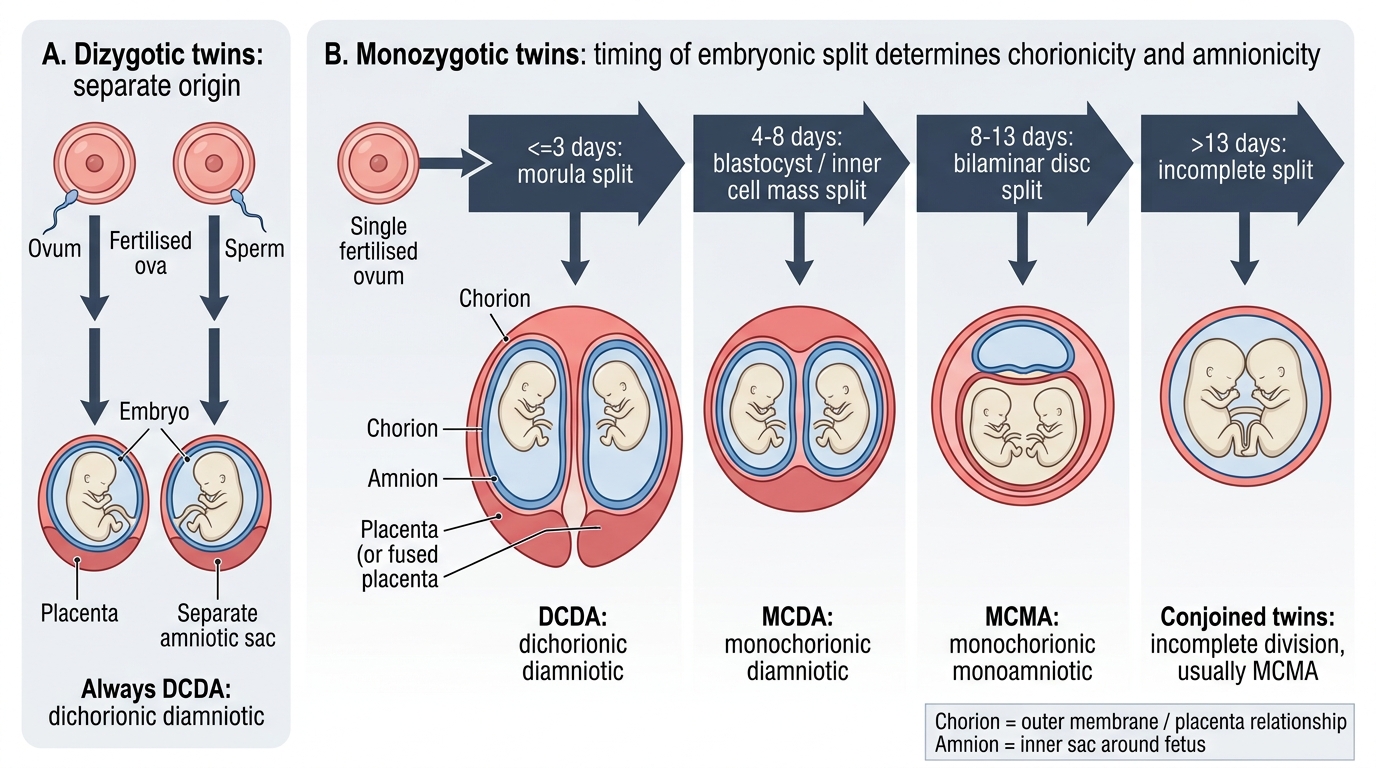
Dizygotic (DZ) twinning — the most common form (~70% of all twins):
- Cause: Two separate ova fertilised by two separate sperms in the same menstrual cycle. Simultaneous release of two oocytes (superfetation/superfecundation).
- Always dichorionic-diamniotic (DCDA): Each embryo implants independently with its own chorion and amnion. There are two separate placentas (or one fused placenta) and two amniotic sacs.
- Risk factors: Increasing maternal age (higher FSH → multifollicular development), family history (maternal side), high parity, African ethnicity, and ovulation-induction drugs.
- Genetics: DZ twins share ~50% of genes — like ordinary siblings.
Monozygotic (MZ) twinning (~30% of all twins):
- Cause: Spontaneous splitting of a single fertilised ovum into two genetically identical embryos. Rate is relatively constant across populations (~3–4 per 1,000 births); slightly increased by IVF (zona manipulation).
- Chorionicity depends entirely on the timing of the split:
- Split ≤3 days (before trophoblast differentiates): Dichorionic-Diamniotic (DCDA) — each twin has its own placenta and amnion. The safest MZ type.
- Split 4–8 days (after chorion forms, before amnion): Monochorionic-Diamniotic (MCDA) — shared placenta, separate amniotic sacs. ~75% of MZ twins. High risk due to shared placental vasculature.
- Split 8–13 days (after amnion forms): Monochorionic-Monoamniotic (MCMA) — shared placenta AND amniotic sac. 1–2% of MZ twins. Highest risk — cord entanglement is universal; fetal mortality up to 50% without intensive surveillance.
- Split >13 days (after disc formation): Conjoined twins — incomplete separation with fused body parts. Extremely rare (1 in 50,000–100,000 deliveries).
- Genetics: MZ twins are genetically identical.
The clinical and prognostic importance of this classification is profound: while a DCDA twin pregnancy (whether MZ or DZ) carries approximately twice the risk of a singleton, a MCDA pregnancy carries 3–4 times the risk due to twin-to-twin transfusion syndrome (TTTS), selective intrauterine growth restriction (sIUGR), and twin anaemia-polycythaemia sequence (TAPS). MCMA pregnancy carries the highest risk of all.
Timing of Twin Splitting and Chorionicity
SELF-CHECK
At a 10-week ultrasound scan, a twin pregnancy shows a triangular wedge of placental tissue projecting into the base of the inter-twin membrane, creating a 'lambda' or 'twin peak' sign. What chorionicity does this indicate, and what is its clinical significance?
A. Monochorionic-diamniotic (MCDA) — higher risk; T-sign confirms shared placenta
B. Dichorionic-diamniotic (DCDA) — lower risk; each twin has its own placenta, no shared vascular anastomoses
C. Monochorionic-monoamniotic (MCMA) — highest risk; absent inter-twin membrane confirms this
D. Dizygotic twinning — always associated with a lambda sign but carries variable risk
Reveal Answer
Answer: B. Dichorionic-diamniotic (DCDA) — lower risk; each twin has its own placenta, no shared vascular anastomoses
The lambda (twin peak) sign — a triangular projection of placental tissue into the base of the inter-twin membrane — indicates dichorionic-diamniotic (DCDA) twinning. In DCDA pregnancies each twin has its own chorion and separate placenta (or two lobes of a fused placenta), with no shared vascular anastomoses. This carries significantly lower risk of TTTS and other monochorionic-specific complications. The T-sign (membrane meets placenta perpendicularly without a wedge of placental tissue) indicates monochorionic twinning.
Diagnosis and Investigations in Multiple Pregnancy
Once multiple pregnancy is suspected on clinical grounds, ultrasonography is the cornerstone of both diagnosis and risk stratification. The timing of the first USS is critical: first-trimester USS (ideally 11–14 weeks) is the optimal window for determining chorionicity with high accuracy (>95%). After 14 weeks, the inter-twin membrane thickens and chorionicity determination becomes progressively less reliable — a diagnostic failure that has significant management implications.
Ultrasound determination of chorionicity — the two signs:
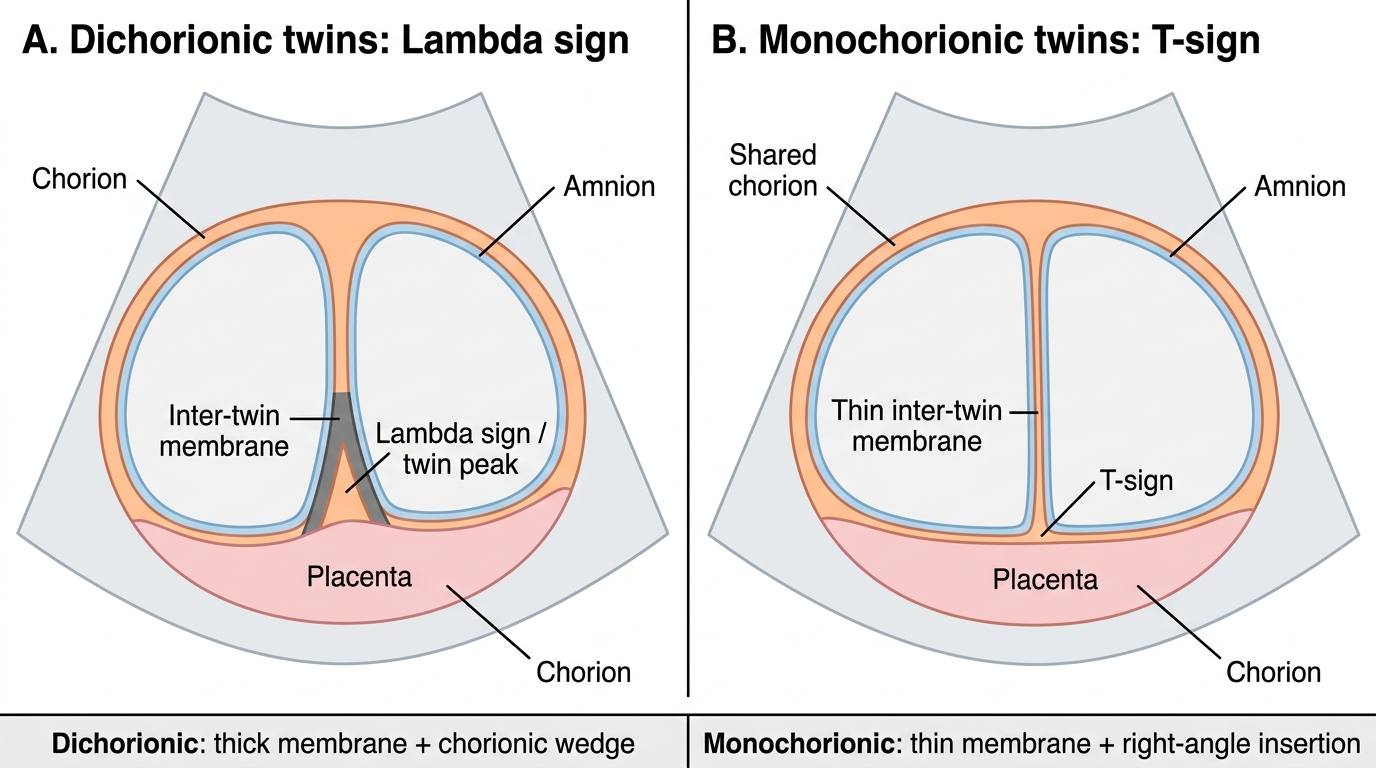
Lambda (twin peak) sign — DCDA:
A triangular wedge of placental tissue projects into the base of the inter-twin membrane, creating a 'peak' visible at the placental surface. This occurs because chorionic villi from both placentas grow into the inter-twin membrane in a DCDA pregnancy. The sign is well-defined in the first trimester and indicates dichorionic placentation.
T-sign — MCDA:
In monochorionic twins, only amniotic tissue forms the inter-twin membrane (no chorionic component), so the membrane meets the placental surface perpendicularly without a placental wedge — forming a 'T' shape at the base. This sign indicates monochorionic placentation and mandates intensive surveillance for TTTS.
MCMA: No inter-twin membrane is identifiable — the two fetuses share a single amniotic sac. Free-floating umbilical cords with no membrane between the twins on USS. Colour Doppler may identify cord entanglement.
Booking investigations for multiple pregnancy:
- All routine antenatal tests (blood group, Rh, haemoglobin, HIV, VDRL, hepatitis B, rubella immunity, urine C&S) — same as singleton.
- GDM screening early (DIPSI or IADPSG): higher risk of gestational diabetes in multiple pregnancy; screen at booking AND 24–28 weeks.
- Detailed fetal anomaly scan at 18–20 weeks: congenital anomalies are more common in MZ twins.
- First-trimester screening (combined test: nuchal translucency + serum PAPP-A/free βhCG): applicable to twin pregnancies; interpretation differs from singletons (serum levels adjusted). Cell-free DNA testing (NIPT) is available.
First Trimester Ultrasound Signs of Chorionicity