Page 7 of 38
OG12.3 | Diabetes in Pregnancy — SDL Guide
Learning Objectives
- Define gestational diabetes mellitus (GDM) and classify diabetes complicating pregnancy
- Describe the pathophysiology of insulin resistance in pregnancy and the mechanism of GDM development
- Apply the DIPSI and IADPSG/WHO-2013 screening protocols correctly, citing the exact thresholds for each
- Identify the adverse effects of diabetes on the mother, foetus, and neonate
- Outline the evidence-based management of diabetes in pregnancy including glycaemic targets, pharmacological therapy, intrapartum care, and postpartum reclassification
INSTRUCTIONS
Diabetes complicates 10–15% of pregnancies in India, and the country carries among the highest burdens of gestational diabetes in the world. Getting the diagnosis right — and naming the correct screening protocol with its exact threshold — is as clinically important as the management itself, because misdiagnosis leads to either under-treatment (maternal and foetal harm) or over-diagnosis (unnecessary anxiety and intervention). This module takes you through the full clinical arc from presentation to postpartum, with a focused section on the DIPSI and IADPSG protocols that are the most commonly tested clinical knowledge points.
References
- DC Dutta's Textbook of Obstetrics, 9th edition, Chapter 14 (textbook)
- Williams Obstetrics, 26th edition, Chapter 57 (textbook)
- FOGSI Good Clinical Practice Recommendations: Gestational Diabetes Mellitus, 2018 (guideline)
- WHO Diagnostic Criteria and Classification of Hyperglycaemia First Detected in Pregnancy, 2013 (guideline)
- Seshiah V et al. DIPSI criteria for GDM diagnosis — Gestational Diabetes India Study, 2004 (research)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Priya, 31 years old, presents for her first antenatal visit at 14 weeks. She is para 1 with a previous large baby (3.9 kg) delivered by emergency caesarean section for shoulder dystocia. Her BMI is 28 kg/m², her mother has Type 2 diabetes, and her fasting blood glucose today is 94 mg/dL. The midwife asks whether she needs a glucose tolerance test. The consultant's answer depends on precise knowledge: which screening protocol to use (DIPSI or IADPSG?), at what gestational age, and how to interpret the result. The stakes are high — undiagnosed gestational diabetes in a woman with this risk profile is a direct route to foetal macrosomia, shoulder dystocia, and neonatal intensive care unit admission.
WHY THIS MATTERS
India has one of the highest burdens of gestational diabetes mellitus (GDM) in the world, with a prevalence estimated at 10–15% of all pregnancies — higher in urban, high-BMI, and older reproductive-age populations. Diabetes in pregnancy is a major driver of foetal macrosomia, shoulder dystocia, neonatal hypoglycaemia, and stillbirth. For the mother, it increases the risk of pre-eclampsia, operative delivery, type 2 diabetes postpartum, and cardiovascular disease later in life. The foetal consequences of hyperglycaemia extend into childhood: offspring of diabetic mothers have a significantly higher risk of developing obesity and type 2 diabetes themselves. For you as a future clinician, understanding and correctly applying the DIPSI and IADPSG screening protocols — with their distinct requirements, thresholds, and clinical contexts — is a high-stakes competency that you will use at every antenatal clinic.
RECALL
Before exploring diabetes in pregnancy, recall from your physiology and biochemistry courses: the pancreatic beta cell senses rising blood glucose via GLUT-2 transporters, closes K-ATP channels, and triggers calcium-mediated insulin secretion; insulin facilitates glucose uptake in muscle and adipose tissue (GLUT-4) and suppresses hepatic gluconeogenesis; counter-regulatory hormones (glucagon, cortisol, growth hormone) oppose insulin. Normal fasting plasma glucose in a non-pregnant adult is 70–99 mg/dL; 2-hour post-load is below 140 mg/dL on a standard OGTT. Pregnancy is a physiologically insulin-resistant state from the second trimester — this is the metabolic backdrop that creates the vulnerability for GDM.
Clinical Presentation and Classification
Diabetes in pregnancy encompasses two clinically and pathophysiologically distinct entities that require separate consideration, though their management principles overlap significantly.
Gestational diabetes mellitus (GDM) is defined as glucose intolerance of any degree with onset or first recognition during pregnancy. It does not include women with overt diabetes diagnosed before pregnancy. GDM typically has no symptoms — it is detected entirely through systematic screening, which is why a structured antenatal screening protocol is non-negotiable. Occasionally, women present with polyuria, polydipsia, or a history of recurrent candidiasis, but these are non-specific and unreliable as screening criteria. The lack of clinical symptoms makes protocol-driven screening the only reliable detection strategy.
Pre-gestational diabetes mellitus (PGDM) refers to women with Type 1 or Type 2 DM diagnosed before the current pregnancy. These women often have established disease with end-organ complications (retinopathy, nephropathy, neuropathy, cardiovascular disease) that influence both pregnancy management and perinatal risk. They require preconception care including optimisation of HbA1c to below 6.5% before conception, folic acid 5 mg/day from preconception, and retinal and renal assessment before pregnancy begins.
Epidemiology and risk factors: The prevalence of GDM in India ranges from 10–15% in most population studies, with urban rates up to 18–22%. Risk factors include:
• Advanced maternal age (≥25 years in Indian context; ≥35 years in European populations)
• Body mass index ≥25 kg/m² (overweight/obesity)
• Family history of diabetes in a first-degree relative
• Previous GDM
• Previous macrosomic infant (birth weight >4 kg)
• Previous unexplained stillbirth
• Polycystic ovary syndrome (PCOS) — insulin resistance is intrinsic to PCOS
• South Asian ethnicity (independently associated with higher GDM risk at lower BMI)
Although the above risk factors identify a high-risk group, FOGSI and many Indian guidelines recommend universal screening of all pregnant women, because a significant proportion of GDM cases occur in women without classical risk factors. This is especially important in India, where dietary patterns and genetic predisposition make the risk more widely distributed than in Western populations.
Provided image
Pathophysiology of Diabetes in Pregnancy
Pregnancy is inherently a state of progressive insulin resistance, a metabolic adaptation that serves the critical purpose of ensuring a continuous glucose supply to the growing foetus. To understand how GDM arises, it is necessary to trace this physiological process and identify precisely where it crosses from normal adaptation into pathology.
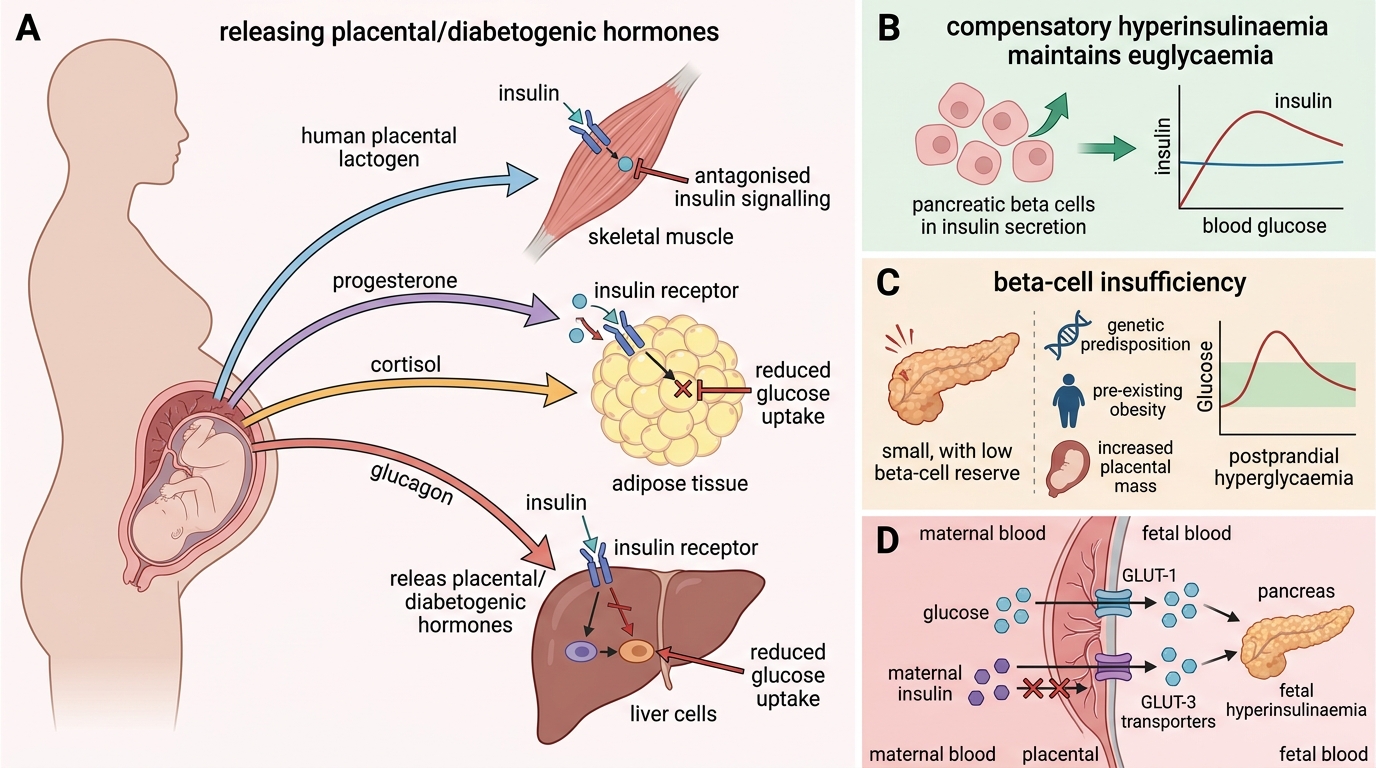
During the first trimester, the metabolic milieu is actually more insulin-sensitive than the non-pregnant state, driven by rising oestrogen and progesterone levels. This early phase promotes anabolic fat storage in the mother, building energy reserves for the later nutritional demands of foetal growth. As the placenta enlarges from the second trimester onward, it secretes increasing quantities of diabetogenic hormones — most importantly human placental lactogen (hPL), but also progesterone, prolactin, placental growth hormone (PGH), and cortisol from the maternal adrenal glands (stimulated by rising CRH). Collectively, these hormones impair insulin receptor signalling at peripheral tissues (muscle and adipose), increase hepatic gluconeogenesis, and accelerate lipolysis.
Pregnancy-Induced Insulin Resistance and GDM
In a metabolically healthy woman, the pancreatic beta cells sense this increasing resistance and mount a compensatory hyperinsulinaemic response — insulin secretion rises two- to threefold by the third trimester, maintaining euglycaemia. GDM develops when beta-cell reserve is insufficient to compensate for the degree of insulin resistance imposed by the pregnancy. The key factors determining beta-cell insufficiency include:
• Genetic predisposition to type 2 diabetes (reduced beta-cell mass or secretory capacity)
• Pre-existing obesity with chronic insulin resistance, reducing the available reserve before pregnancy begins
• Increasing placental mass (with twin pregnancies or macrosomia in a current pregnancy) generating proportionally higher levels of diabetogenic hormones
The pathophysiological consequences cascade through multiple systems. Maternal postprandial hyperglycaemia drives increased glucose transfer across the placenta to the foetus via facilitated diffusion (GLUT-1 and GLUT-3 transporters); glucose crosses the placenta but maternal insulin does NOT. The foetal pancreas responds with foetal hyperinsulinaemia, which is the central mechanism for most neonatal complications:
• Insulin is a potent foetal growth factor → macrosomia (foetal body weight >4 kg or >90th centile)
• Insulin suppresses foetal lung surfactant synthesis → respiratory distress syndrome (RDS) in the neonate, even at term
• Hyperinsulinaemia at delivery, in the absence of continuing maternal glucose supply, causes neonatal hypoglycaemia within 1–2 hours of birth
• Foetal erythropoiesis is stimulated by relative hypoxia in an overgrown placenta → polycythaemia
In pre-gestational diabetes, particularly Type 1 DM, the risk of congenital anomalies is significantly elevated (two- to fivefold above baseline), especially cardiac defects (ventricular septal defect, transposition of great arteries) and neural tube defects (failure to close during organogenesis at 3–8 weeks — before most women know they are pregnant). The teratogenic mechanism is hyperglycaemia-induced free radical generation disrupting organogenesis. This is the reason preconception HbA1c optimisation is so critical in known diabetic women: the period of greatest teratogenic risk has passed before GDM would even be screened for.
Screening and Diagnosis — DIPSI and IADPSG Protocols
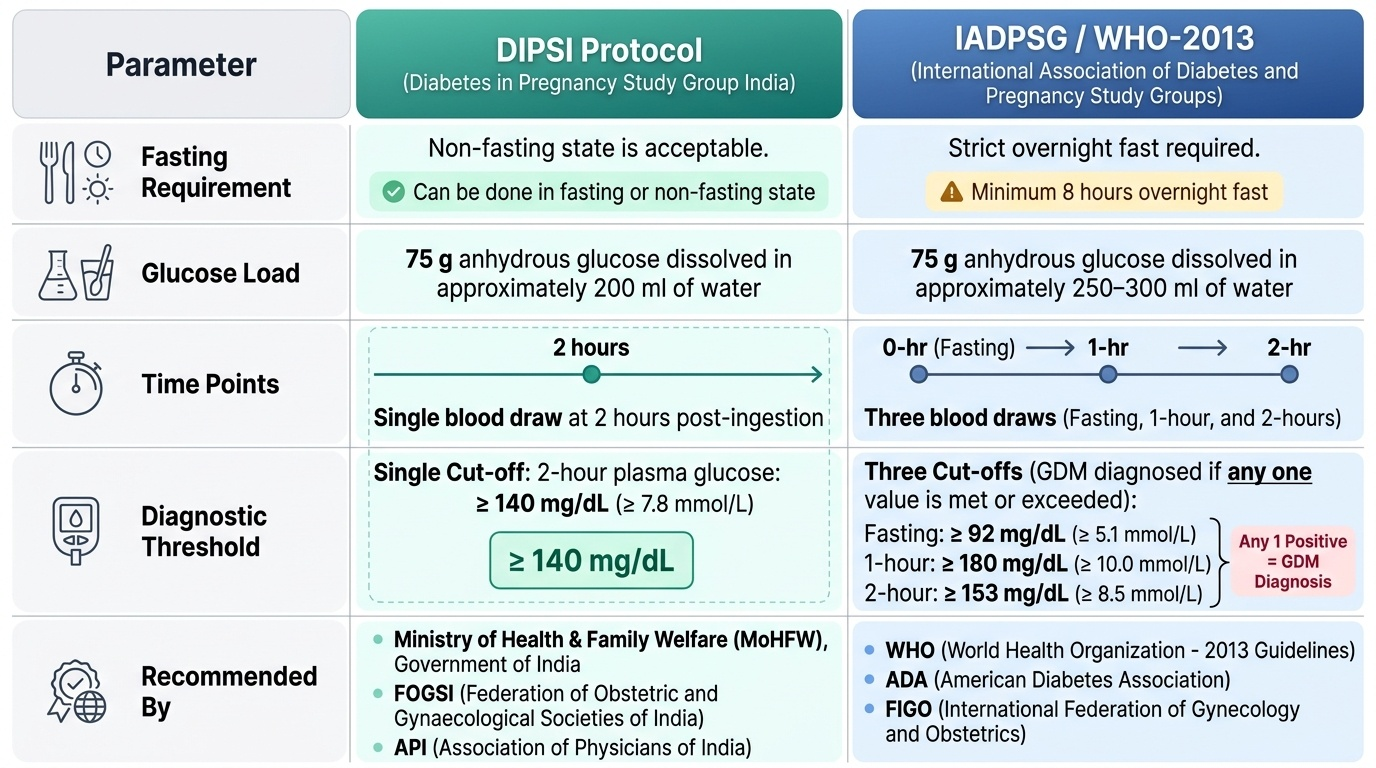
The correct diagnosis of GDM requires not only knowing the diagnostic threshold but knowing WHICH protocol it belongs to, and WHY they differ. This distinction is clinically important: applying the wrong protocol's threshold to the wrong test condition can lead to either missed GDM (if the IADPSG 2-hour threshold of 153 mg/dL is applied to a DIPSI test, which uses a cut-off of 140 mg/dL) or inappropriate diagnosis (if DIPSI's lower threshold is applied to an IADPSG test). The two protocols also have different logistical implications — DIPSI's non-fasting design makes it far more practical for high-volume antenatal settings in India, whereas IADPSG's three-point measurement provides greater sensitivity at the cost of requiring a pre-scheduled fasting test. Both use the same glucose load (75 g) but are otherwise distinct tools and must not be conflated. Confusing the two protocols is one of the most common factual errors in obstetric examinations and clinical practice. They use different pre-test conditions, measure different time points, and apply different cut-offs — they are NOT interchangeable.
The DIPSI Protocol (Diabetes in Pregnancy Study Group India)
The Diabetes in Pregnancy Study Group India (DIPSI) protocol was developed and validated in the Indian population specifically to address the practical limitations of fasting OGTT in a resource-constrained, high-volume antenatal care setting. The key innovation is its non-fasting design:
- The patient arrives in the non-fasting state (no requirement for overnight fast)
- She is given 75 g of oral glucose dissolved in water
- A single venous plasma glucose sample is collected 2 hours after the glucose load
- Diagnostic threshold: 2-h plasma glucose ≥ 140 mg/dL = GDM
If the 2-hour value is below 120 mg/dL, GDM is excluded. If it is 120–139 mg/dL, repeat testing is advised. The non-fasting design makes the test logistically simpler (no appointment required for fasting state), reducing the non-attendance rates that are common when fasting OGTT is mandated. FOGSI endorses DIPSI as the preferred screening strategy for India. Timing: DIPSI is performed at 24–28 weeks for average-risk women; at booking (first visit) for high-risk women, repeated at 24–28 weeks if the first test is negative.
The IADPSG/WHO-2013 Protocol (International Association of Diabetes and Pregnancy Study Groups)
The IADPSG criteria were developed following the landmark HAPO (Hyperglycaemia and Adverse Pregnancy Outcomes) study (2008), a multinational cohort study of over 25,000 pregnant women that demonstrated a continuous graded relationship between maternal blood glucose levels and adverse perinatal outcomes (macrosomia, primary caesarean section, neonatal hypoglycaemia, cord blood C-peptide). The WHO adopted IADPSG criteria in 2013.
The IADPSG/WHO-2013 protocol requires:
- The patient must be in the fasting state (overnight fast of ≥8 hours)
- 75 g oral glucose is administered
- Venous plasma glucose is measured at three time points: fasting (0 min), 1 hour, and 2 hours
- GDM is diagnosed if ANY ONE of the following thresholds is met:
- Fasting plasma glucose ≥ 92 mg/dL
- 1-hour plasma glucose ≥ 180 mg/dL
- 2-hour plasma glucose ≥ 153 mg/dL
The IADPSG criteria are more sensitive than older criteria (Carpenter-Coustan, NDDG) because they are based on continuous risk data rather than arbitrary cut-offs derived from older populations. However, because ANY ONE threshold triggers the diagnosis, the prevalence of GDM rises substantially (up to 17–18% in some Indian cohorts), raising debate about over-medicalisation of normal pregnancy.
The key distinction — do not merge these protocols:
| Feature | DIPSI | IADPSG/WHO-2013 |
|---|---|---|
| Fasting required? | No (non-fasting) | Yes (overnight fast ≥8 h) |
| Glucose load | 75 g | 75 g |
| Time points measured | 2-h only | Fasting, 1-h, 2-h |
| Diagnostic cut-off | 2-h ≥ 140 mg/dL | Fasting ≥ 92, OR 1-h ≥ 180, OR 2-h ≥ 153 mg/dL |
| Diagnostic logic | Single threshold | ANY ONE of three = positive |
| Setting | India; pragmatic universal screening | International; most studies/guidelines |
A 2-h value of 145 mg/dL is positive by DIPSI but NOT necessarily positive by IADPSG — the IADPSG 2-h threshold is 153 mg/dL. Never apply a DIPSI result using the IADPSG cut-off, or vice versa.
Overt diabetes in pregnancy is distinguished from GDM by higher thresholds detected at any time in pregnancy: fasting glucose ≥ 126 mg/dL, or random glucose ≥ 200 mg/dL with symptoms, or HbA1c ≥ 6.5% — these represent probable pre-gestational diabetes first detected in pregnancy, not GDM.
SELF-CHECK
A woman at 26 weeks has a DIPSI test: 75 g glucose given without fasting; 2-hour venous plasma glucose = 148 mg/dL. Which statement is correct?
A. The test is negative because 148 mg/dL is below the IADPSG 2-hour threshold of 153 mg/dL
B. The test is positive for GDM because the DIPSI threshold is ≥140 mg/dL
C. The test is inconclusive; she needs a fasting OGTT to confirm
D. A 75 g non-fasting glucose test cannot diagnose GDM; only fasting OGTT is valid
Reveal Answer
Answer: B. The test is positive for GDM because the DIPSI threshold is ≥140 mg/dL
The DIPSI protocol uses 75 g glucose (non-fasting) and a single 2-hour cut-off of ≥140 mg/dL. A value of 148 mg/dL exceeds this threshold, making this a positive DIPSI test — GDM is diagnosed. The IADPSG/WHO-2013 protocol requires fasting and uses different thresholds (2-h cut-off 153 mg/dL); these are separate protocols and MUST NOT be mixed. The DIPSI protocol is FOGSI-endorsed for India and IS a valid diagnostic method.