Page 10 of 38
OG12.4 | Heart Disease in Pregnancy — SDL Guide
Learning Objectives
- Classify the common causes of heart disease complicating pregnancy and apply NYHA functional classification
- Describe the pathophysiological cardiovascular changes of normal pregnancy and explain why they stress a diseased heart
- Identify investigations required for cardiac assessment in pregnancy and apply WHO modified risk stratification
- Describe the adverse effects of cardiac disease on the mother and foetus
- Outline the management of heart disease in pregnancy, including antenatal care, intrapartum management, and postpartum surveillance
INSTRUCTIONS
Heart disease is a leading indirect cause of maternal mortality in India, accounting for 10–15% of all maternal deaths. The majority of cases represent rheumatic heart disease — a preventable consequence of inadequately treated streptococcal pharyngitis — making this a subject where clinical knowledge directly translates into preventable deaths. This module uses the OG disease arc to take you from recognising presentations to managing complex cardiac patients through labour, with emphasis on the dangerous lesions and NYHA classification that determine clinical decision-making.
References
- DC Dutta's Textbook of Obstetrics, 9th edition, Chapter 14 (textbook)
- Williams Obstetrics, 26th edition, Chapter 49 (textbook)
- ESC Guidelines on the Management of Cardiovascular Diseases during Pregnancy, 2018 (guideline)
- FOGSI Good Clinical Practice Recommendations: Cardiac Disease in Pregnancy (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Sunita, 24 years old, G2P1, presents at 28 weeks with progressively worsening breathlessness over the past two weeks. She is now breathless walking on the flat and woke twice last night with difficulty breathing. Her first delivery two years ago was uneventful, but she never had cardiac evaluation. On examination: pulse 110 bpm irregularly irregular, BP 100/70 mmHg, JVP elevated, bilateral basal crepitations, and a loud mid-diastolic murmur at the mitral area with an opening snap. The diagnosis is mitral stenosis in atrial fibrillation — a cardiac emergency in pregnancy that, if not recognised and managed promptly, carries a maternal mortality risk of 5–10%. Understanding why the cardiovascular changes of pregnancy have now pushed Sunita's fixed mitral obstruction to the point of decompensation is the foundation of this module.
WHY THIS MATTERS
Heart disease complicates approximately 1–3% of pregnancies globally but accounts for a disproportionately high 10–15% of maternal deaths in India. Unlike many developed countries where congenital heart disease now predominates, rheumatic heart disease (RHD) remains the dominant aetiology in India, accounting for up to 80% of cardiac disease in pregnancy — a reflection of ongoing Group A streptococcal infection, inadequate primary healthcare, and failed secondary prophylaxis in childhood. The obstetrician managing a woman with cardiac disease must understand not only the haemodynamic consequences of each lesion but also the physiological demands of pregnancy — because it is the interaction of disease and physiology, not disease alone, that determines outcome. Maternal mortality from cardiac disease is preventable with multidisciplinary management, appropriate risk stratification, and timely intervention.
RECALL
Before exploring cardiac disease in pregnancy, recall from your physiology course: cardiac output = heart rate × stroke volume; preload is the end-diastolic filling volume, and afterload is the systemic vascular resistance against which the heart ejects; the normal cardiac output at rest is 4–6 L/min. The mitral valve sits between the left atrium and left ventricle; stenosis creates a pressure gradient that impairs ventricular filling. Atrial fibrillation (AF) loses the atrial 'kick' and reduces ventricular filling by a further 20–25% — critical context for understanding why AF is so dangerous in mitral stenosis. Keep these haemodynamic principles in mind as you explore how pregnancy amplifies the stress on a compromised heart.
Clinical Presentation of Heart Disease in Pregnancy
Heart disease in pregnancy presents a profound diagnostic challenge because normal pregnancy itself produces symptoms and signs that mimic cardiac disease. The physiological breathlessness of pregnancy, the dependent oedema from venodilation, the palpitations from an increased heart rate, and the soft systolic flow murmurs generated by the turbulent high-flow state are all expected findings in a healthy pregnant woman, yet each of these is also a potential symptom or sign of cardiac decompensation. Distinguishing physiological adaptation from early heart failure requires careful attention to severity, progression, timing, and the specific features described below. The consequence of missing a cardiac diagnosis in pregnancy is severe: mitral stenosis unmasked by pregnancy may deteriorate from NYHA Class II to Class III or IV within weeks during the period of peak cardiac output increase (28–32 weeks), and the difference in maternal mortality between managed and unmanaged disease at this stage can be tenfold. because many of the symptoms of a normal pregnancy — breathlessness on exertion, palpitations, ankle oedema, and fatigue — overlap with the symptoms of cardiac decompensation. The clinical skill lies in differentiating physiological from pathological symptoms and identifying the warning signs that demand urgent cardiac evaluation.
Normal pregnancy produces physiological breathlessness (due to the elevated diaphragm and progesterone-driven hyperventilation), ankle oedema (due to venodilation and reduced plasma oncotic pressure), and functional systolic flow murmurs (due to increased blood volume and turbulent flow). None of these are alarming in isolation. However, certain features are NOT physiological and demand urgent evaluation:
• Orthopnoea (breathlessness lying flat) and paroxysmal nocturnal dyspnoea — indicate pulmonary congestion
• Haemoptysis — in pregnancy, strongly associated with mitral stenosis (pulmonary venous hypertension)
• Cyanosis — indicates right-to-left shunting or severe arterial desaturation
• Diastolic murmurs and loud systolic murmurs — functional murmurs are soft (grade 1–2/6), systolic, and ejection quality; diastolic murmurs are ALWAYS pathological
• Syncope on exertion — suggests fixed cardiac output state (severe aortic stenosis, hypertrophic obstructive cardiomyopathy)
• Irregularly irregular pulse — may indicate atrial fibrillation
New York Heart Association (NYHA) Functional Classification is the cornerstone of clinical risk stratification in cardiac disease in pregnancy:
| NYHA Class | Description | Pregnancy Implications |
|---|---|---|
| I | No symptoms with ordinary physical activity | Safe; close monitoring |
| II | Slight limitation; symptomatic with strenuous activity | Safe with multidisciplinary care |
| III | Marked limitation; symptomatic with less-than-ordinary activity | High maternal risk; tertiary care essential |
| IV | Symptoms at rest; unable to perform any activity without discomfort | Pregnancy inadvisable; if pregnant, ICU-level care |
NYHA Class III and IV carry maternal mortality rates of 5–15% with standard care. The prognosis is lesion-specific: mitral stenosis in NYHA III with AF may carry mortality above 10%; cyanotic CHD with pulmonary hypertension (Eisenmenger syndrome) carries 30–50% maternal mortality regardless of NYHA class.
The typical presentation scenario in India is a young primigravida or grand-multipara who was never diagnosed with RHD in childhood, who presents in the second or third trimester when the haemodynamic demands of pregnancy unmask a previously compensated valvular lesion. The first presentation of cardiac disease in pregnancy is thus a common clinical scenario that every obstetrician must be equipped to recognise and manage.
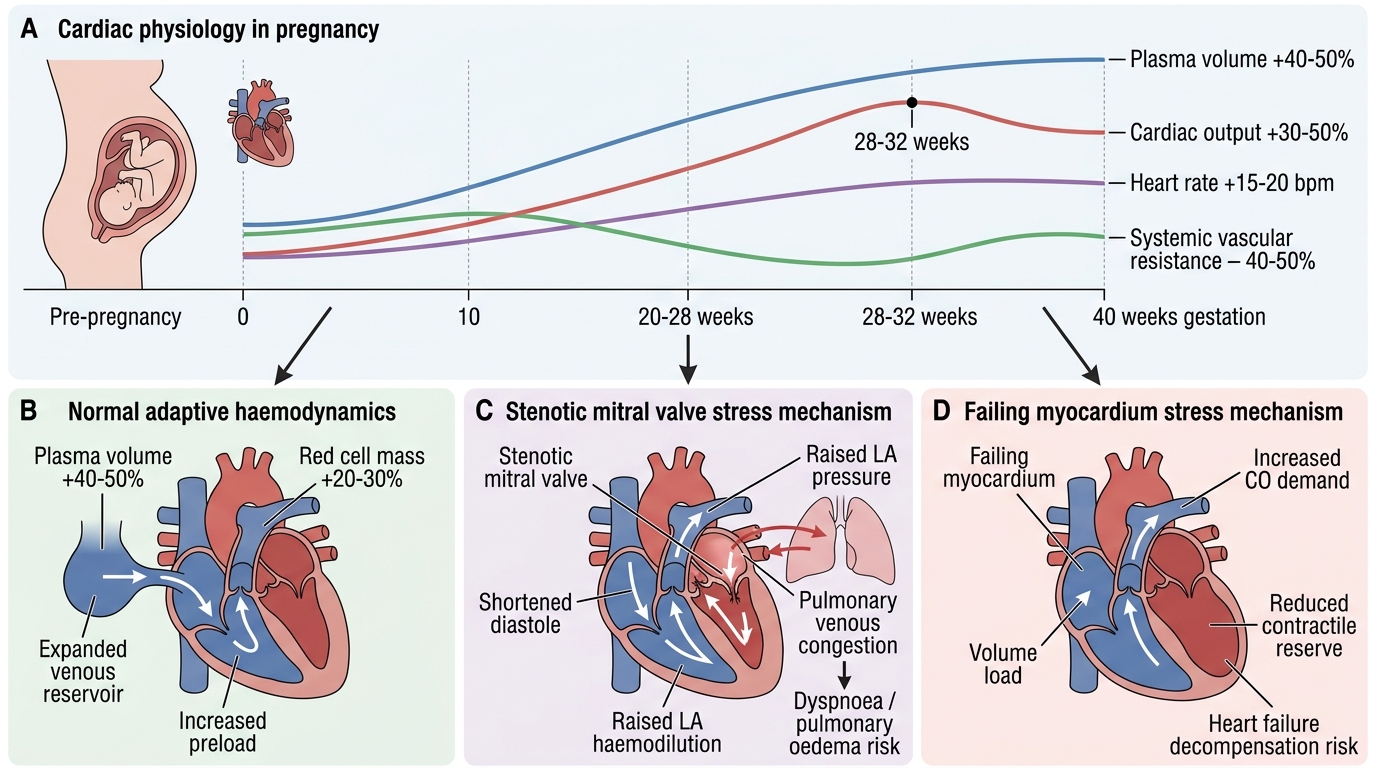
Pathophysiology — Cardiovascular Changes in Pregnancy
Pregnancy imposes a series of progressive and substantial haemodynamic changes on the maternal cardiovascular system, beginning in the first trimester and reaching their maximum at approximately 28–32 weeks. These changes are physiologically necessary to meet the increasing oxygen and nutritional demands of the growing foetus, to expand the uteroplacental circulation, and to prepare the body for the blood loss of delivery. In a normal heart this workload is accommodated without symptoms, and the woman may notice only mild palpitations and exertional breathlessness, which are considered normal. In a diseased heart — particularly one with a fixed valvular obstruction such as mitral stenosis, or with reduced myocardial reserve as in cardiomyopathy — these same physiological changes can tip the balance from compensated to decompensated, precipitating pulmonary oedema, arrhythmia, or acute cardiac failure. Understanding the timeline and magnitude of these haemodynamic changes is therefore the essential foundation for understanding why pregnancy unmasks cardiac disease, and why certain gestational ages and the peripartum period represent the highest-risk windows. that collectively create an enormous additional workload. In a normal heart this workload is accommodated without symptoms; in a diseased heart it can precipitate decompensation, arrhythmia, or acute cardiac failure. Understanding the timeline and magnitude of these changes allows the clinician to anticipate the highest-risk periods and plan accordingly.
Cardiovascular Changes in Pregnancy and Cardiac Disease Stress
The key haemodynamic changes of pregnancy are:
Blood volume and plasma expansion:
- Plasma volume expands by 40–50% (from approximately 2.6 L to 3.7 L)
- Red cell mass expands by 20–30%
- Net result: relative haemodilution, but substantially increased total circulating volume and preload
Cardiac output:
- Rises by 30–50% above the pre-pregnancy baseline, peaking at 28–32 weeks at approximately 6.5–8 L/min
- Increased cardiac output is driven by both increased heart rate (+15–20 bpm) and increased stroke volume (+20–30%)
- At full term, cardiac output begins to fall slightly, returning toward baseline in the immediate postpartum period (though with transient surges during uterine contractions)
Systemic vascular resistance (SVR):
- Falls progressively from the first trimester (nadir at 20–28 weeks) due to progesterone-mediated systemic vasodilation, placental arteriovenous shunting, and increased prostaglandins
- The fall in SVR is a key protective mechanism — it offloads the left ventricle and reduces afterload. For regurgitant lesions (mitral regurgitation, aortic regurgitation) where a fall in afterload is beneficial, this is protective. For stenotic lesions (mitral stenosis, aortic stenosis) where reduced SVR may cause systemic hypotension without the ability to increase forward flow through the stenosed valve, it is potentially hazardous.
The critical period — labour and the immediate postpartum:
- Each uterine contraction returns 300–500 mL of blood to the central circulation (autotransfusion effect), creating transient surges in cardiac output of 20–25%
- Immediately after delivery, the relief of aortocaval compression increases venous return sharply
- The involuting uterus releases its blood volume over 24–72 hours — creating a second peak of fluid mobilisation that can precipitate pulmonary oedema in women with mitral stenosis, cardiomyopathy, or impaired left ventricular function
Why mitral stenosis is the most dangerous lesion:
The mitral valve in stenosis creates a fixed obstruction between the left atrium and left ventricle. As pregnancy increases the demand for cardiac output, the heart cannot increase flow through the stenotic valve proportionally. Left atrial pressure rises (to overcome the gradient across the stenosed valve), transmitting back to the pulmonary veins — causing pulmonary venous hypertension and ultimately pulmonary oedema. When atrial fibrillation supervenes (triggered by the dilated, hypertensive left atrium), the loss of the atrial 'kick' and the rapid ventricular rate dramatically impair diastolic filling, precipitating acute decompensation. This is Sunita's scenario — and it is the single most common obstetric cardiac emergency in India.
SELF-CHECK
A pregnant woman at 30 weeks with known mitral stenosis develops sudden onset atrial fibrillation. Why is this particularly dangerous in her case?
A. Atrial fibrillation causes pulmonary embolism directly
B. Loss of atrial contraction reduces ventricular filling through the already-obstructed mitral valve, precipitating acute haemodynamic decompensation
C. Atrial fibrillation causes placental abruption
D. Mitral stenosis is only dangerous in the first trimester
Reveal Answer
Answer: B. Loss of atrial contraction reduces ventricular filling through the already-obstructed mitral valve, precipitating acute haemodynamic decompensation
In mitral stenosis, the stenotic valve already restricts left ventricular filling. Atrial fibrillation (AF) causes two additional problems: (1) loss of the atrial 'kick' reduces ventricular filling by 20–25%; and (2) the rapid ventricular rate in uncontrolled AF shortens diastole — the time available for blood to flow across the obstructed valve. Both effects reduce forward cardiac output and raise left atrial pressure, triggering pulmonary oedema. AF in MS is a cardiac emergency requiring rate control (digoxin or beta-blocker) and anticoagulation.
Classification and Investigations
A systematic classification of the underlying cardiac lesion — combined with objective quantification of its severity through investigations — is essential for determining the risk profile of the pregnancy and selecting the appropriate management pathway. No single clinical sign can reliably grade the severity of a valvular lesion; the combination of NYHA class (subjective functional limitation) and echocardiographic parameters (objective structural and haemodynamic data) forms the basis of risk stratification. In India, because rheumatic heart disease dominates the clinical landscape, the most commonly encountered scenario is a young woman presenting for antenatal care with previously undiagnosed mitral stenosis or combined mitral valve disease. The classification scheme below organises the common causes by aetiology, followed by the investigations used to characterise each lesion and the WHO mWHO risk stratification framework that translates the diagnosis into a management plan. — combined with objective assessment of its severity — is essential for determining the risk of the pregnancy and guiding management decisions. In India, the predominant lesion encountered is rheumatic mitral stenosis, but a complete differential must be considered in every woman presenting with cardiac symptoms in pregnancy.
Classification by aetiology:
1. Rheumatic Heart Disease (RHD) — accounts for approximately 80% of cardiac disease in pregnancy in India
- Mitral stenosis (MS): most common and most dangerous rheumatic lesion in pregnancy; fixed obstruction limits the increase in cardiac output required by pregnancy; poor tolerance of tachycardia, AF, and increased preload
- Mitral regurgitation (MR): generally better tolerated than MS because the fall in SVR in pregnancy reduces regurgitant fraction; risk of AF and left ventricular failure with severe MR
- Aortic stenosis (AS): uncommon as rheumatic in young women; more often congenital (bicuspid aortic valve); severe AS (valve area <1 cm²) carries maternal mortality risk; fixed output prevents accommodation of pregnancy demands
- Aortic regurgitation (AR): relatively well tolerated; fall in SVR in pregnancy reduces regurgitant fraction
- Combined lesions (MS + AR, etc.): complex management; requires specialist cardiology input
2. Congenital Heart Disease (CHD) — increasing proportion as corrected CHD patients survive to reproductive age
- Atrial septal defect (ASD): often undiagnosed until pregnancy; generally well tolerated; risk of paradoxical embolism
- Ventricular septal defect (VSD): small VSDs well tolerated; large VSDs risk Eisenmenger physiology
- Patent ductus arteriosus (PDA): small well tolerated; large risk of Eisenmenger
- Eisenmenger syndrome: pulmonary hypertension with reversed right-to-left shunting; maternal mortality 30–50%; pregnancy is absolutely contraindicated
- Tetralogy of Fallot (corrected): risk depends on residual pulmonary regurgitation and right ventricular function
- Coarctation of the aorta: risk of dissection with hypertension in pregnancy
3. Cardiomyopathies
- Peripartum cardiomyopathy (PPCM): pregnancy-specific dilated cardiomyopathy presenting in the last month of pregnancy or within 5 months postpartum, in the absence of prior cardiac disease, with left ventricular ejection fraction (LVEF) below 45%; mechanism includes myocarditis, nutritional deficiency (selenium), and prolactin-mediated cardiotoxicity; recurrence risk in subsequent pregnancy if LVEF has not normalised
- Hypertrophic obstructive cardiomyopathy (HOCM): risk of syncope on exertion; generally well tolerated in pregnancy if outflow obstruction is not severe
4. Ischaemic heart disease — uncommon in women of reproductive age but increasing with obesity, smoking, and older maternal age; acute MI in pregnancy carries high mortality
Provided image
Investigations:
| Investigation | Key findings in cardiac disease | Notes |
|---|---|---|
| ECG | AF, ventricular hypertrophy, ischaemia, axis deviation | Safe in pregnancy; first-line |
| Echocardiography (2D + Doppler) | Valve area, pressure gradients, EF, wall motion, pulmonary artery pressure | Safe; diagnostic gold standard |
| Chest X-ray | Cardiomegaly, pulmonary vascular congestion, pleural effusion | Safe (shielded); useful in acute decompensation |
| BNP/NT-proBNP | Elevated in cardiac failure; prognostic marker | |
| Pulse oximetry | SpO₂ <94% at rest suggests significant shunt or pulmonary hypertension | |
| Exercise testing | Contraindicated in high-risk lesions in pregnancy |
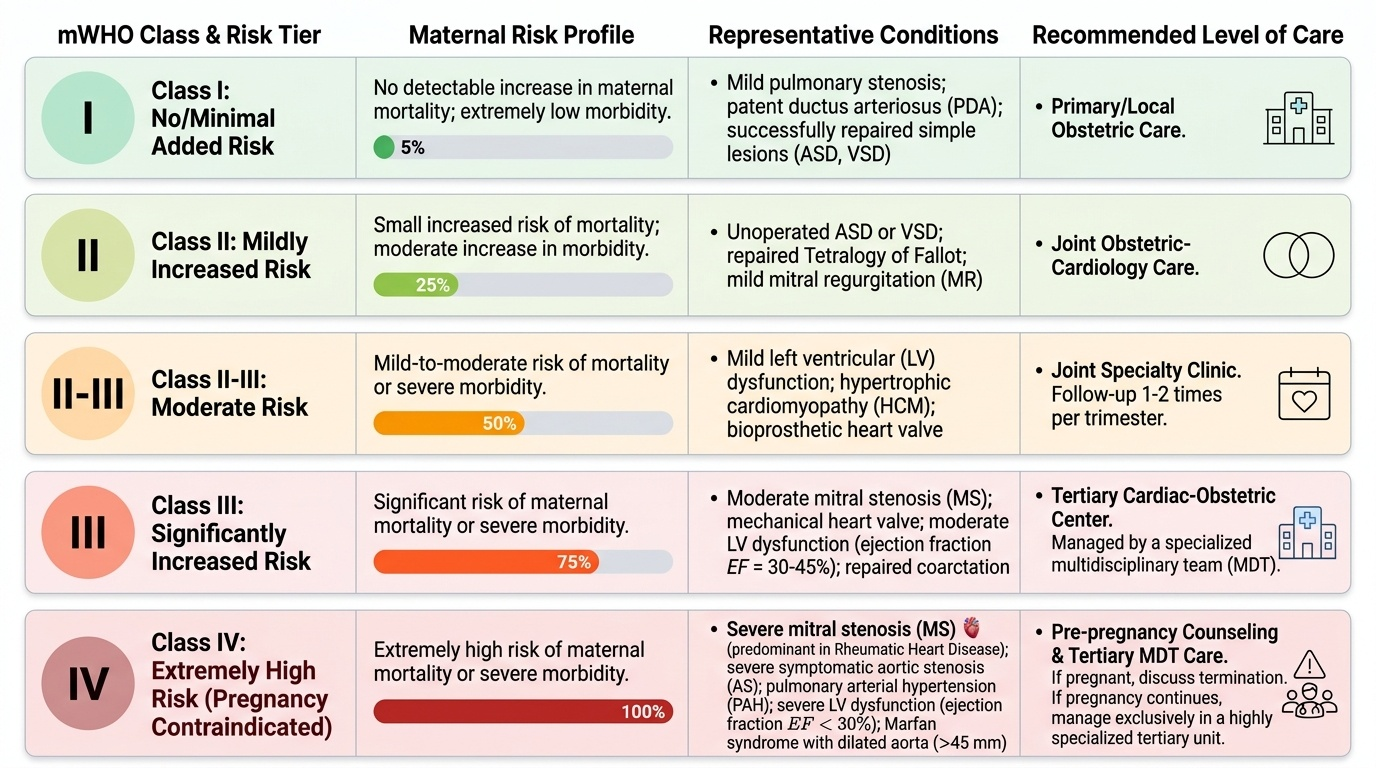
The WHO modified classification (mWHO) provides a validated risk stratification framework: mWHO I = no detectable increased risk of maternal mortality; mWHO II–III = moderate risk; mWHO IV = extremely high risk (pregnancy contraindicated or requires ICU-level management). This classification guides the level of care required and the composition of the multidisciplinary team.