Page 1 of 38
OG12.1 | Hypertensive Disorders of Pregnancy — SDL Guide
Learning Objectives
- Define and classify the hypertensive disorders of pregnancy (chronic hypertension, gestational hypertension, pre-eclampsia, eclampsia, HELLP syndrome, and superimposed pre-eclampsia).
- Describe the aetiology and pathophysiology of pre-eclampsia, including abnormal trophoblast invasion, defective spiral-artery remodelling, and the anti-angiogenic sFlt-1/PlGF axis.
- State the diagnostic criteria and severe-feature thresholds for pre-eclampsia and eclampsia.
- Outline the investigations required in a woman with hypertensive disorders of pregnancy.
- Describe the principles of management: antihypertensive therapy, magnesium sulphate prophylaxis and treatment, timing and mode of delivery, and prevention.
INSTRUCTIONS
Hypertensive disorders of pregnancy (HDP) complicate 5–10% of all pregnancies worldwide and are a leading cause of maternal and perinatal morbidity and mortality in India. This module covers the full spectrum from gestational hypertension through pre-eclampsia to eclampsia and HELLP syndrome, with emphasis on early detection, the pathophysiological basis of organ damage, and evidence-based management including MgSO4 regimens. Mastery is essential for every clinician who will care for pregnant women at any level of the health system.
References
- DC Dutta's Textbook of Obstetrics, 9th ed. — Chapter on Hypertensive Disorders of Pregnancy (textbook)
- Williams Obstetrics, 26th ed. — Chapters 40–41: Hypertensive Disorders (textbook)
- FOGSI/ICMR Good Clinical Practice Recommendations: Hypertensive Disorders of Pregnancy (2024) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 26-year-old primigravida at 34 weeks of gestation is brought to the emergency labour room by her husband. She has been complaining of a severe throbbing headache for six hours and blurring of vision since morning. On examination her blood pressure is recorded at 172/110 mmHg on two readings taken 20 minutes apart. She has 3+ pitting oedema of both feet and legs. Urine dipstick shows protein 3+. As you begin your assessment, the patient suddenly arches her back, her jaw clenches, and she begins generalised tonic-clonic convulsions. You have two minutes to act. What is your immediate diagnosis, and what drug — at what dose — do you reach for first?
WHY THIS MATTERS
Hypertensive disorders of pregnancy (HDP) complicate approximately 5–10% of all pregnancies and collectively constitute one of the three leading causes of direct maternal mortality in India alongside haemorrhage and sepsis. Eclampsia alone contributes significantly to both maternal deaths and perinatal mortality, particularly in low-resource settings where antenatal surveillance is inconsistent. As a final-year student moving toward internship and postings in antenatal care, labour rooms, and emergency medicine, you will encounter HDP in every clinical year of your career. The ability to correctly classify a patient's condition, identify severe features promptly, and institute appropriate MgSO4 and antihypertensive therapy within minutes can be the difference between a live mother and a preventable death. Beyond acute management, understanding the pathophysiological basis of HDP equips you to counsel women on prevention, recognise early warning signs in the community, and audit maternal mortality cases during your career.
RECALL
Before proceeding, anchor this module to what you already know:
- Vascular physiology in pregnancy (PY/Year 1): In normal pregnancy, total peripheral resistance falls dramatically due to vasodilatory prostaglandins and nitric oxide; blood pressure actually dips in the second trimester before returning toward pre-pregnancy levels at term. You have learned how oestrogen and progesterone modify vascular tone — this context makes the endothelial dysfunction of pre-eclampsia all the more striking.
- Trophoblast invasion and spiral arteries: In Year 1 reproductive physiology you studied how cytotrophoblast cells migrate into the decidua and remodel the uterine spiral arteries from high-resistance muscular vessels into wide-bore, low-resistance conduits — the physiological transformation of pregnancy. Failure of this process is the upstream trigger for pre-eclampsia.
- Renal physiology in pregnancy (PY): GFR increases by ~50% in normal pregnancy; serum creatinine and uric acid fall. Upper limits of normal for creatinine and uric acid are therefore different in pregnancy — a 'normal' creatinine on standard lab reference ranges may represent impaired renal function in a pregnant woman.
- Coagulation (PY/Haematology): Pregnancy is a hypercoagulable state. When HDP progresses to HELLP syndrome and DIC becomes a complication, you will need to recall the coagulation cascade and interpret coagulation indices accurately.
Clinical Presentation and Spectrum of HDP
Hypertensive disorders of pregnancy encompass a heterogeneous spectrum of conditions united by the common feature of elevated blood pressure occurring in the context of pregnancy. The clinical presentation ranges from completely asymptomatic incidental blood-pressure elevation detected at an antenatal visit, through a florid multi-system syndrome of severe pre-eclampsia, to life-threatening convulsions and end-organ failure. Understanding the spectrum as a continuum — rather than as discrete isolated entities — is essential because a woman can move rapidly from one category to a more severe one, and the clinician must recognise the early stages while remaining vigilant for deterioration.
The cardinal symptom triad of pre-eclampsia comprises new-onset hypertension, proteinuria, and — in severe disease — symptoms of end-organ involvement. The neurological warning signs include a persistent, throbbing headache (classically frontal or occipital) that is unresponsive to simple analgesics, visual disturbances such as photophobia, blurred vision, or scotomata (reflecting cerebral and retinal arteriolar spasm), and hyperreflexia. Epigastric pain or right upper quadrant pain signals hepatic capsule distension or hepatic infarction and predicts imminent HELLP or eclampsia. Dependent oedema — particularly facial and hand oedema developing acutely — is clinically significant, though mild pedal oedema is common in normal pregnancy and alone is not diagnostic. Rapid excessive weight gain (more than 0.5 kg per week) may precede overt oedema. Eclampsia is the occurrence of new-onset generalised tonic-clonic convulsions in a woman with pre-eclampsia, in the absence of other explanatory causes; notably, a convulsion can occur without preceding severe hypertension or proteinuria in up to one-third of cases.
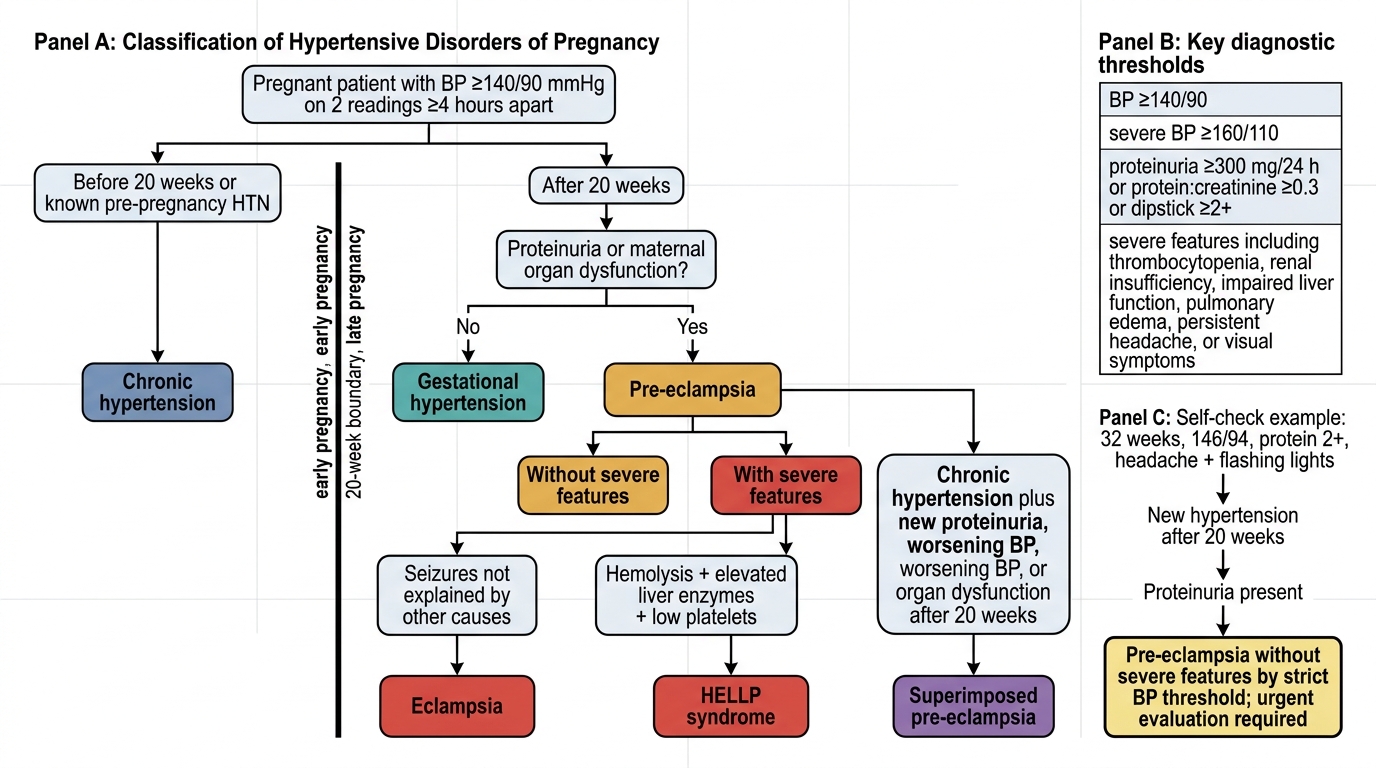
The internationally recognised classification of HDP is as follows:
- Chronic hypertension: Hypertension diagnosed before pregnancy or before 20 completed weeks of gestation, or persisting beyond 12 weeks postpartum. It may be primary (essential) or secondary.
- Gestational hypertension: New-onset hypertension (systolic BP ≥140 mmHg or diastolic BP ≥90 mmHg) arising after 20 weeks of gestation, without proteinuria or end-organ dysfunction, and resolving within 12 weeks postpartum.
- Pre-eclampsia: New-onset hypertension (BP ≥140/90 mmHg) after 20 completed weeks of gestation, accompanied by proteinuria (≥300 mg in 24 hours, or PCR ≥30 mg/mmol, or dipstick ≥2+) OR — in the absence of proteinuria — any of the following end-organ features: thrombocytopaenia (<100 × 10⁹/L), renal insufficiency (creatinine >97 µmol/L or doubling of baseline), impaired liver function (transaminases twice normal, with or without severe RUQ/epigastric pain), pulmonary oedema, or new-onset headache or visual disturbance unresponsive to medication. Pre-eclampsia is further classified as without severe features (meeting minimum diagnostic criteria) or with severe features (BP ≥160/110 mmHg on two occasions, or any of the above end-organ criteria met to a severe degree).
- Eclampsia: The onset of generalised convulsions (not explained by other pathology) in a woman with pre-eclampsia. It is considered a complication and obstetric emergency, not a separate entity.
- HELLP syndrome: A severe variant characterised by Haemolysis (microangiopathic haemolytic anaemia on peripheral blood film), Elevated Liver enzymes (AST/ALT typically >70 IU/L), and Low Platelets (<100 × 10⁹/L). HELLP may occur in the context of pre-eclampsia but can also present with minimal or absent hypertension and proteinuria.
- Superimposed pre-eclampsia: Development of pre-eclampsia in a woman with pre-existing chronic hypertension. It carries a higher risk of adverse outcomes than either condition alone.
IMPORTANT NOTE: The 20-week gestational boundary is definitional for gestational hypertension and pre-eclampsia. Hypertension presenting before 20 weeks is almost always chronic or secondary in aetiology (gestational trophoblastic disease is a rare exception that may cause early-onset features); it should not be labelled pre-eclampsia.
Classification of Hypertensive Disorders of Pregnancy
SELF-CHECK
A 28-year-old primigravida at 32 weeks gestation has two blood pressure readings of 146/94 mmHg four hours apart. Urinalysis shows protein 2+ on dipstick. She complains of headache and sees 'flashing lights'. Which classification most accurately describes her condition?
A. Gestational hypertension
B. Pre-eclampsia without severe features
C. Pre-eclampsia with severe features
D. Chronic hypertension with superimposed pre-eclampsia
Reveal Answer
Answer: B. Pre-eclampsia without severe features
This patient has new-onset hypertension (≥140/90 mmHg) after 20 weeks of gestation, plus proteinuria (2+ dipstick ≥ the threshold of ≥2+), meeting the diagnostic criteria for pre-eclampsia. The BP readings are below the severe-feature threshold of 160/110 mmHg. While she has neurological symptoms (headache, visual disturbance), these alone do not automatically upgrade to 'severe features' unless the BP meets the ≥160/110 threshold or the symptoms are unresponsive to medication with no other explanation. In clinical practice, her symptom complex would prompt urgent evaluation and low threshold for classifying as severe features, but strictly by the classification, she meets pre-eclampsia without severe features based on the stated BP readings. Chronic HTN with superimposed pre-eclampsia requires known pre-existing hypertension before 20 weeks.
Pathophysiology: From Placental Ischaemia to Endothelial Dysfunction
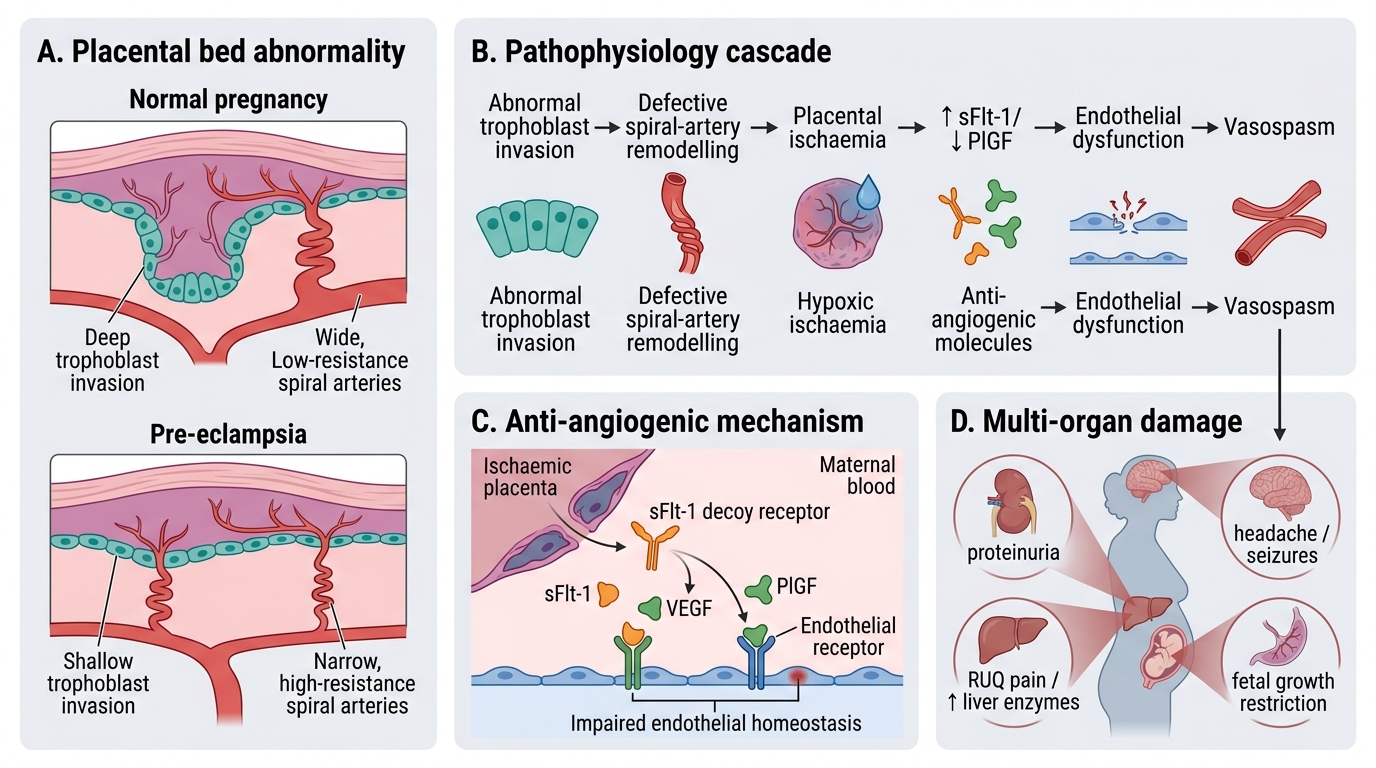
Pre-eclampsia is fundamentally a placental disorder with systemic maternal consequences. The initiating defect occurs long before clinical symptoms appear — typically in the first trimester when trophoblast cells fail to remodel the uterine spiral arteries adequately. Understanding this two-stage model of pre-eclampsia is essential for interpreting both the clinical syndrome and emerging preventive strategies.
In a normal pregnancy, cytotrophoblast cells invade the decidua basalis and the walls of the maternal spiral arteries in two waves: the first at 8–10 weeks of gestation and the second at 16–20 weeks. This endovascular invasion replaces the muscular wall of the spiral arteries with fibrinoid material, converting them from narrow, high-resistance, vasoconstrictive vessels into wide-bore, low-pressure conduits. The result is an approximately 10-fold increase in blood flow to the intervillous space, securing the metabolic needs of the rapidly growing fetus and placenta. In pre-eclampsia, this transformation is incomplete — defective spiral-artery remodelling leaves vessels in a persistent high-resistance state. The uterine spiral arteries retain their muscular media, remain vasoresponsive, and fail to deliver adequate blood flow to the placenta, resulting in placental ischaemia and intermittent hypoxia-reperfusion injury.
The ischaemic placenta responds by secreting a cascade of factors that enter the maternal circulation and act on the systemic vascular endothelium. The most important of these are the anti-angiogenic factors: sFlt-1 (soluble fms-like tyrosine kinase-1) is a circulating decoy receptor that binds and neutralises two pro-angiogenic vascular growth factors — VEGF (vascular endothelial growth factor) and PlGF (placental growth factor). In pre-eclampsia, maternal serum sFlt-1 is markedly elevated and PlGF is markedly reduced. The resulting VEGF and PlGF deficiency disrupts normal vascular endothelial homeostasis throughout the maternal systemic vasculature.
Endothelial dysfunction is the central mechanism linking placental ischaemia to the clinical syndrome. Dysfunctional endothelium loses its anti-thrombotic, vasodilatory, and barrier properties:
- Vasospasm — reduced nitric oxide production and increased endothelin release cause generalised arteriolar vasoconstriction, raising systemic vascular resistance and blood pressure. This is the haemodynamic basis of hypertension.
- Increased capillary permeability — endothelial barrier breakdown allows protein-rich fluid to leak into the interstitial space (oedema) and into the urine (proteinuria via glomerular endotheliosis — the characteristic renal lesion of pre-eclampsia).
- Platelet activation and consumption — endothelial injury promotes platelet aggregation; in severe disease this leads to the thrombocytopaenia of HELLP syndrome.
- Multi-organ involvement — the same endothelial dysfunction affects every organ bed:
- Kidney: glomerular endotheliosis → proteinuria, elevated creatinine, hyperuricaemia (reduced uric-acid clearance is an early biomarker).
- Liver: hepatic sinusoidal fibrin deposition → elevated transaminases, subcapsular haematoma, RUQ pain; in HELLP syndrome, liver infarction may occur.
- Brain: cerebral arteriolar vasospasm + increased permeability → hypertensive encephalopathy, cerebral oedema, seizures (eclampsia). The mechanism of eclamptic convulsions is multifactorial but cerebral vasospasm and posterior reversible encephalopathy syndrome (PRES) are central.
- Placenta and fetus: chronic ischaemia → fetal growth restriction (FGR), oligohydramnios, placental abruption.
- Coagulation: endothelial injury + thrombocytopaenia → risk of disseminated intravascular coagulation (DIC), especially in HELLP and placental abruption.
The clinical importance of the sFlt-1/PlGF ratio as a predictive biomarker stems directly from this pathophysiology — an elevated ratio (>38 or validated laboratory cut-off) in a symptomatic woman is highly predictive of imminent or confirmed pre-eclampsia, and a low ratio can effectively rule out pre-eclampsia for up to one week in a suspected case. While sFlt-1/PlGF testing is not universally available in Indian settings, its underpinning science helps explain why aspirin (acting partly through thromboxane/prostacyclin balance and trophoblast invasion) and calcium (acting on vascular tone and potentially trophoblast function) reduce pre-eclampsia risk.
Pathophysiology of Pre-eclampsia
SELF-CHECK
In the pathogenesis of pre-eclampsia, the primary role of elevated soluble fms-like tyrosine kinase-1 (sFlt-1) is to:
A. Directly cause vasoconstriction by activating smooth muscle calcium channels
B. Act as a decoy receptor that neutralises circulating VEGF and PlGF, impairing endothelial homeostasis
C. Stimulate platelet aggregation via thromboxane A2 upregulation
D. Promote trophoblast invasion and spiral-artery remodelling
Reveal Answer
Answer: B. Act as a decoy receptor that neutralises circulating VEGF and PlGF, impairing endothelial homeostasis
sFlt-1 is a truncated, soluble form of the VEGF/PlGF receptor (Flt-1/VEGFR-1) that is secreted in excess by the ischaemic placenta. It circulates in the maternal bloodstream and acts as a decoy receptor, binding free VEGF and PlGF and preventing them from interacting with their endothelial receptors. The resulting VEGF and PlGF deficiency impairs endothelial cell survival, increases vascular permeability, and promotes vasospasm — collectively producing the systemic manifestations of pre-eclampsia. It does not directly act on smooth muscle calcium channels or thromboxane. Rather, sFlt-1 promotes, not inhibits, invasion failure — the ischaemic placenta releases sFlt-1 as a consequence of defective trophoblast invasion, not as a cause of it.
Diagnosis and Investigation
The diagnosis of hypertensive disorders of pregnancy rests on accurate blood pressure measurement, detection of proteinuria, and clinical and laboratory assessment for end-organ involvement. Standardised measurement technique is critical because white-coat hypertension, anxiety, and positional artefact are common in pregnancy. BP should be measured in the sitting or semi-recumbent position (never supine, to avoid aortocaval compression), after five minutes of rest, with the arm supported at heart level, using a validated device. Two readings taken at least four hours apart are required for the diagnosis of gestational hypertension or pre-eclampsia, or readings taken two minutes apart if BP is ≥160/110 and rapid treatment is urgently indicated. The importance of accurate technique cannot be overstated: a falsely elevated reading from incorrect positioning or an anxious patient may lead to unnecessary intervention, while a falsely normal reading from poor technique may provide false reassurance in a deteriorating woman. Investigations serve a dual purpose — confirming the diagnosis by quantifying proteinuria and end-organ markers, and monitoring for progression and complications that signal the need for urgent delivery. The full assessment also includes mandatory fetal surveillance because uteroplacental insufficiency may compromise the fetus even before maternal indices reach critical thresholds.
Diagnostic thresholds:
- A systolic BP ≥140 mmHg or diastolic BP ≥90 mmHg on two occasions ≥4 hours apart, arising after 20 completed weeks of gestation, defines hypertension in the context of HDP.
- Proteinuria threshold: ≥300 mg of protein in a 24-hour urine collection, OR a spot urine protein:creatinine ratio (PCR) ≥30 mg/mmol (or equivalently ≥0.3 mg/mg), OR dipstick ≥2+ on a freshly voided, midstream specimen in the absence of urinary infection. Dipstick alone is the least reliable method but remains the screening tool at primary and secondary care levels in India. A 24-hour collection or PCR is required to confirm significant proteinuria before diagnosis. Proteinuria is NOT required for the diagnosis of pre-eclampsia if end-organ features are present.
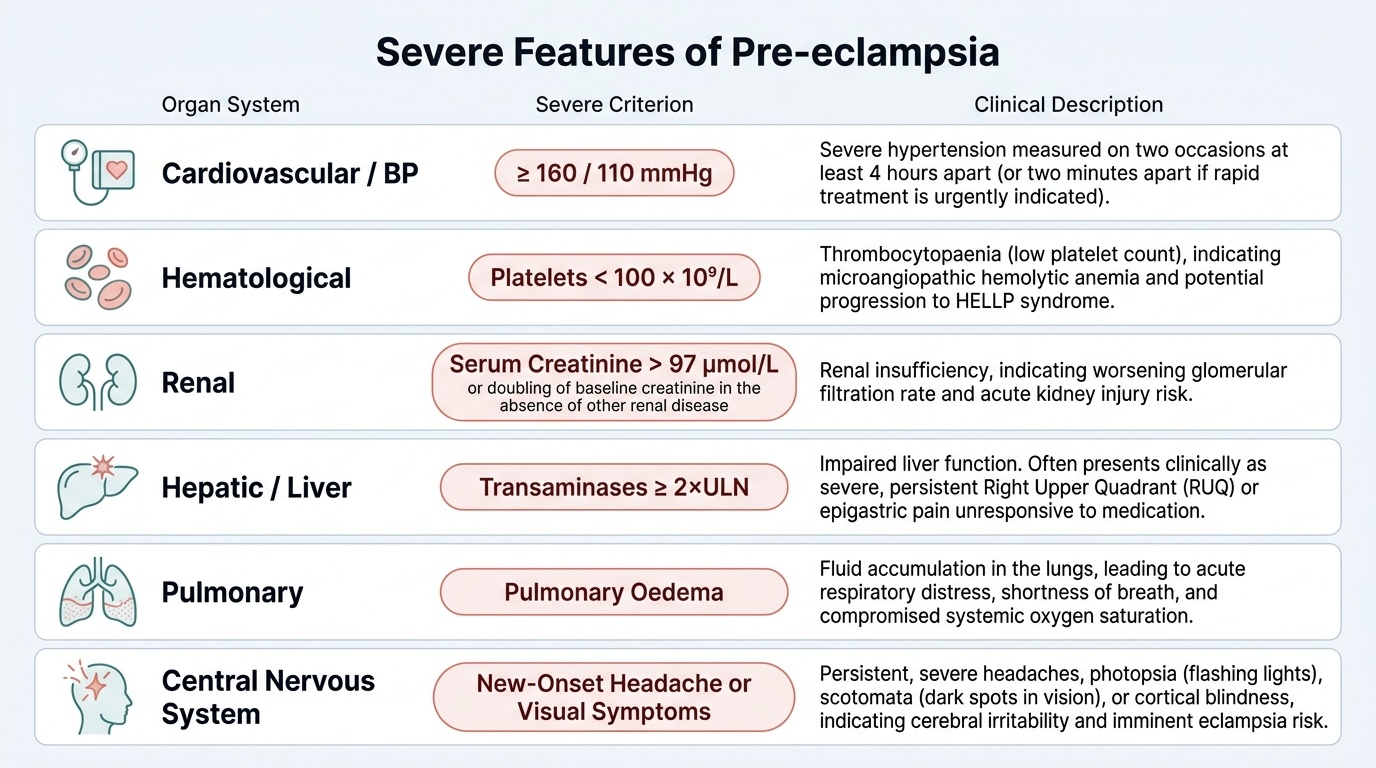
Severe-feature criteria (any one suffices):
- Systolic BP ≥160 mmHg or diastolic BP ≥110 mmHg on two occasions.
- Thrombocytopaenia: platelets <100 × 10⁹/L.
- Renal insufficiency: serum creatinine >97 µmol/L (>1.1 mg/dL) in the absence of other renal disease, or doubling of baseline creatinine.
- Impaired liver function: elevated transaminases (AST or ALT twice the upper limit of normal) with or without severe right upper quadrant or epigastric pain refractory to medication.
- Pulmonary oedema.
- New-onset headache unresponsive to medication and not accounted for by alternative diagnoses, or new visual symptoms.
Provided image
Laboratory investigations required in all women with suspected or confirmed pre-eclampsia:
| Investigation | Rationale / What to look for |
|---|---|
| Full blood count (CBC) + peripheral blood film | Thrombocytopaenia, microangiopathic haemolytic anaemia (schistocytes) in HELLP |
| Serum urea, creatinine, uric acid | Renal function; uric acid ≥5.5 mg/dL is an early marker of disease severity |
| Liver function tests (AST, ALT, LDH, bilirubin) | Hepatic involvement; elevated LDH + haemolysis supports HELLP |
| Serum albumin | Oedema mechanism; hypoalbuminaemia in severe disease |
| Urine PCR or 24-hour urine protein | Quantify proteinuria |
| Coagulation (PT, APTT, fibrinogen, D-dimer) | DIC screen if platelets <100 or clinical suspicion |
| Blood group and crossmatch | Pre-delivery preparation |
| sFlt-1/PlGF ratio (where available) | Risk stratification; ratio >38 = high risk of progression |
Fetal surveillance:
Because uteroplacental insufficiency may cause fetal compromise before delivery becomes inevitable, continuous fetal monitoring is mandatory in any woman with severe features or in labour:
- Non-stress test (NST) / cardiotocography (CTG): baseline rate, variability, accelerations, decelerations.
- Obstetric ultrasound: fetal biometry (detect FGR — abdominal circumference <10th centile), amniotic fluid index (oligohydramnios), placenta localisation.
- Umbilical artery Doppler: absent or reversed end-diastolic flow indicates severe uteroplacental insufficiency and is an indication for delivery or intensive surveillance depending on gestational age.
- Middle cerebral artery (MCA) Doppler: assess fetal brain-sparing response.
- Biophysical profile (BPP): composite score (NST + ultrasound) ≤4/10 suggests acute fetal compromise.