Page 31 of 38
OG12.11,OG16.4 | Intrauterine Growth Retardation — SDL Guide
Learning Objectives
- Define IUGR and SGA and distinguish between them using customised growth charts
- Classify IUGR as symmetrical or asymmetrical and explain the pathophysiological basis of each type
- Enumerate the maternal, placental, and fetal causes of IUGR
- Describe the clinical assessment and ultrasound biometry used to diagnose IUGR
- Interpret fetal Doppler waveforms — umbilical artery, middle cerebral artery, cerebroplacental ratio, and ductus venosus — in the context of fetal surveillance
- Outline the principles of management, including evidence-based delivery timing (TRUFFLE/GRIT), antenatal corticosteroids, and MgSO4 neuroprotection
- Counsel a pregnant woman regarding recurrence risk, modifiable risk factors, and long-term fetal programming consequences
INSTRUCTIONS
IUGR is one of the leading causes of perinatal morbidity and mortality worldwide. The fetus that fails to reach its growth potential is at significantly heightened risk of stillbirth, neonatal hypoxia, metabolic complications, and long-term cardiometabolic disease. For a final-year medical student, the ability to identify IUGR early through clinical surveillance, interpret Doppler changes in a logical escalating sequence, and apply evidence-based delivery criteria represents a core obstetric skill. This module guides you through the full clinical journey — from the antenatal clinic where fundal height lags behind gestational age, to the labour ward where timing of delivery can be the difference between survival and tragedy.
References
- DC Dutta's Textbook of Obstetrics, 9th edition, Ch 25 (textbook)
- Williams Obstetrics, 25th edition, Ch 44 (textbook)
- RCOG Green-top Guideline No. 31: The Investigation and Management of the Small-for-Gestational-Age Fetus, 2013 (guideline)
- TRUFFLE Study (Trial of Umbilical and Fetal Flow in Europe), Lancet 2015 (trial)
- FOGSI Clinical Practice Guideline: Fetal Growth Restriction, 2020 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 30-year-old primigravida with a booking blood pressure of 130/85 mmHg attends your antenatal clinic at 32 weeks. Her last three fundal height measurements plot consistently below the 10th centile on the customised growth chart — the curve has not crossed upward. An urgent ultrasound confirms estimated fetal weight at the 7th centile, with a disproportionately small abdominal circumference relative to the head. The umbilical artery Doppler shows an elevated S/D ratio with absent end-diastolic flow. The fetus that seemed 'a bit small' has just revealed itself as significantly compromised. Your next decision — how urgently to act, what surveillance to start, and when to deliver — will determine whether this pregnancy ends in a healthy newborn or a perinatal tragedy.
WHY THIS MATTERS
Intrauterine growth retardation (IUGR) complicates 3–10% of pregnancies globally and is responsible for approximately 30% of stillbirths and a significant proportion of neonatal ICU admissions. In India, the burden is higher due to the prevalence of maternal undernutrition, anaemia, and hypertensive disorders — all recognised causes of IUGR. As a final-year student, you will routinely plot fundal height charts in antenatal clinics and must be able to recognise the growth-faltering pattern that triggers further assessment. The ability to escalate appropriately — from plotting a chart to organising a Doppler study to informing delivery timing — is a core competency (OG12.11, OG16.4) tested in clinical exams and essential for safe independent practice.
RECALL
Before proceeding, consolidate your foundational knowledge:
• Normal fetal growth is driven by genetic potential, substrate supply (oxygen and nutrients via the uteroplacental circulation), and fetal hormones (IGF-1, insulin). Fetal weight at term is approximately 3–3.5 kg.
• Placental physiology: trophoblastic invasion of spiral arteries converts them from high-resistance muscular vessels to low-resistance, high-flow conduits. This transformation occurs in two waves (6–8 and 16–18 weeks). Failure of remodelling → high resistance → reduced flow → fetal substrate deprivation.
• Customised growth charts (GROW charts): adjust for maternal height, weight, parity, and ethnicity to derive an individual's optimal birth weight — superior to population-based charts for identifying pathological smallness.
• Doppler physics basics: the pulsatility index (PI) and systolic/diastolic (S/D) ratio reflect downstream vascular resistance. As placental resistance rises, diastolic flow in the umbilical artery first decreases, then disappears, then reverses — a progressive deterioration mirroring fetal hypoxia.
• Fetal circulation redistribution (brain-sparing): in chronic hypoxia, fetal cardiac output is preferentially directed to the brain, heart, and adrenals; splanchnic and renal circulations are constricted — this is why the abdominal circumference (reflecting liver glycogen and fat stores) falls first.
Clinical Presentation and Recognition of IUGR
The recognition of IUGR begins in the antenatal clinic, where the earliest and most accessible screening tool is the symphysis-fundal height (SFH) measurement. In a normally growing pregnancy, the fundal height in centimetres approximates the gestational age in weeks (within ±2 cm after 20 weeks). When the SFH consistently measures below the 10th centile on a customised chart, or when serial measurements show a velocity that is too slow — crossing centile lines downward over two or more visits — IUGR must be actively excluded. This clinical sign has a sensitivity of approximately 27–76% and specificity of 85–88% for detecting a small-for-gestational-age fetus, meaning it is a useful prompt for referral but not a substitute for ultrasound confirmation.
The distinction between IUGR and SGA (small for gestational age) is clinically important and frequently examined. SGA is a descriptive term based on birth weight: a baby whose birth weight falls below the 10th centile for gestational age is classified as SGA. IUGR, by contrast, refers to a process — the failure of a fetus to achieve its genetic growth potential in utero, irrespective of birth weight centile. A constitutionally small but otherwise healthy fetus may be SGA without being growth restricted; conversely, a fetus may be IUGR even when its absolute weight appears within the population norm if its customised growth potential is significantly higher. In clinical practice, the two terms are often used interchangeably, but the underlying distinction drives management — only the growth-restricted fetus requires Doppler surveillance and delivery planning.
Risk factors that should heighten clinical suspicion during history-taking include hypertensive disorders of pregnancy (the single most common cause), previous IUGR (recurrence risk 20–25%), antiphospholipid syndrome, chronic renal disease, diabetes with vasculopathy, severe maternal undernutrition (BMI <18.5), heavy smoking (>10 cigarettes/day), alcohol use, and multiple pregnancy. A previous small-for-dates baby, preterm birth, or unexplained stillbirth in the obstetric history should always prompt customised growth monitoring from the second trimester.
Symmetrical vs Asymmetrical IUGR
Pathophysiology: Symmetrical vs Asymmetrical IUGR and Aetiological Mechanisms
Understanding the pathophysiology of IUGR requires appreciating two distinct mechanisms that produce growth restriction at different gestational ages, for different reasons, with different clinical and prognostic implications.
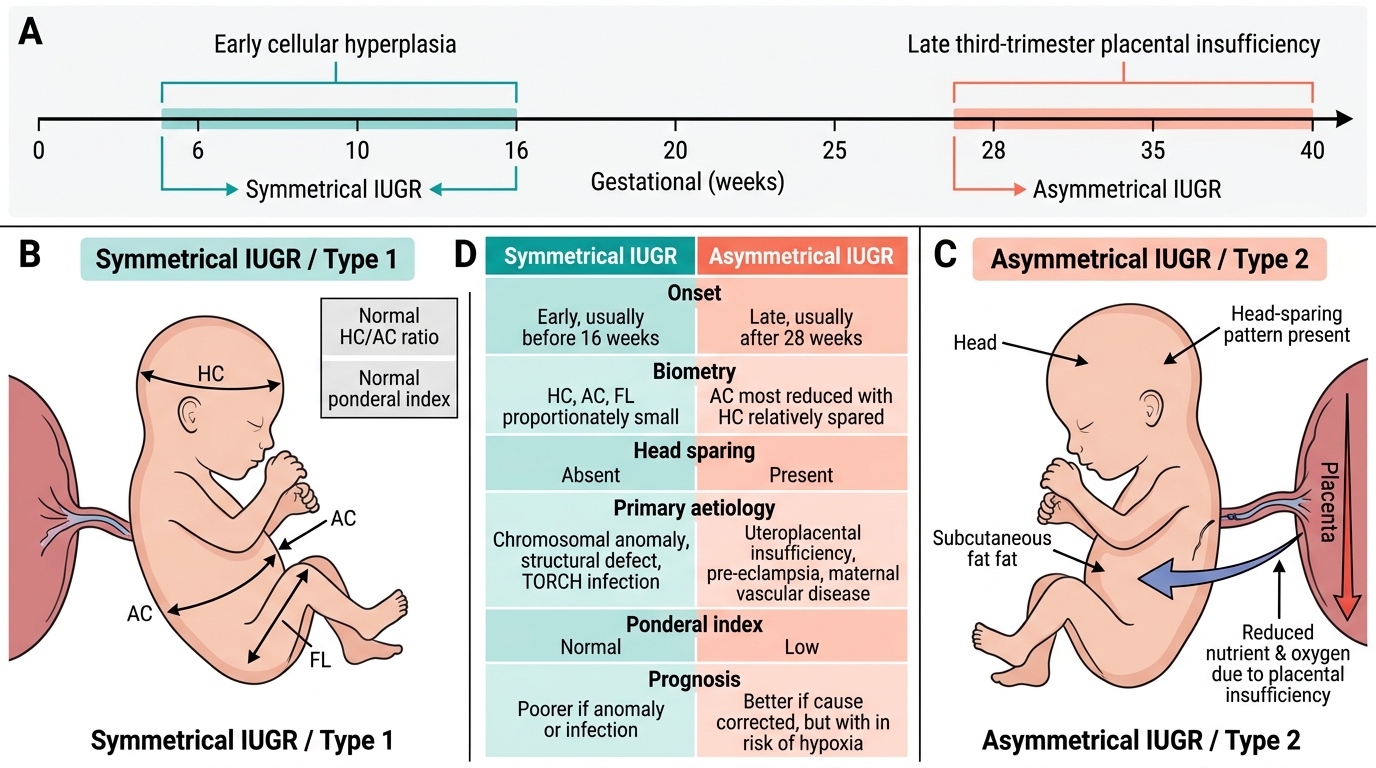
Symmetrical IUGR (also called type 1) accounts for approximately 20–30% of cases. It arises when a pathological process impairs fetal growth from early in gestation — typically during the phase of cellular hyperplasia (before 16 weeks), when organ growth depends on an increase in cell number. The insult affects all organ systems equally, producing proportionate reduction in head circumference, abdominal circumference, and femur length. The HC/AC ratio remains normal (the head is not disproportionately large), and the ponderal index (birthweight / length³ × 100) is preserved within normal range. Brain sparing does not occur because the restriction is global and constitutional. The typical causes are chromosomal anomalies (trisomy 13, 18, 21), structural fetal defects, congenital infections (TORCH organisms — toxoplasmosis, rubella, cytomegalovirus, herpes), or severe early-onset uteroplacental disease before trophoblastic invasion is complete. The prognosis in symmetrical IUGR depends almost entirely on the underlying cause: chromosomal or structural causes carry high mortality and morbidity; infectious causes have variable but often poor neurodevelopmental outcomes.
Asymmetrical IUGR (type 2) constitutes the majority of clinical IUGR cases (70–80%). It results from uteroplacental insufficiency — inadequate transfer of oxygen and nutrients through a compromised placenta — occurring later in pregnancy during the phase of cellular hypertrophy (after 28 weeks). In response to chronic hypoxia and substrate deprivation, the fetal cardiovascular system redistributes cardiac output preferentially to the brain, myocardium, and adrenals at the expense of the splanchnic circulation (gut, liver, kidneys). This brain-sparing response produces the characteristic biometric signature: the head circumference is relatively preserved while the abdominal circumference (reflecting hepatic glycogen depletion and reduced subcutaneous fat) is disproportionately small — producing an elevated HC/AC ratio, the hallmark of asymmetrical IUGR. Skin-fold thickness is reduced; the neonate appears wasted. The ponderal index is low. Oligohydramnios develops because renal cortical vasoconstriction reduces fetal urine output — the combination of absent liquor and poor growth indicates advanced compromise.
The aetiological classification separates causes into three categories:
Maternal causes include hypertensive disorders of pregnancy (the most common single cause — up to 30–40% of cases), antiphospholipid syndrome, thrombophilias (factor V Leiden, protein C/S deficiency, antithrombin III deficiency), chronic renal disease, Type 1 diabetes with nephropathy, anaemia (especially severe iron-deficiency and sickle cell disease), malnutrition, low BMI, heavy smoking, alcohol, substance abuse, and living at high altitude.
Placental causes include failure of trophoblastic invasion (the primary event in most uteroplacental insufficiency), placental infarcts, circumvallate placenta, placenta praevia (low-lying, reducing perfusion), velamentous cord insertion (where umbilical vessels run unprotected through membranes), single umbilical artery, and twin-to-twin transfusion syndrome in monochorionic twins.
Fetal causes include chromosomal anomalies, genetic syndromes (Russell-Silver syndrome — IUGR with body asymmetry and relative macrocephaly), multiple pregnancy, and severe structural defects.
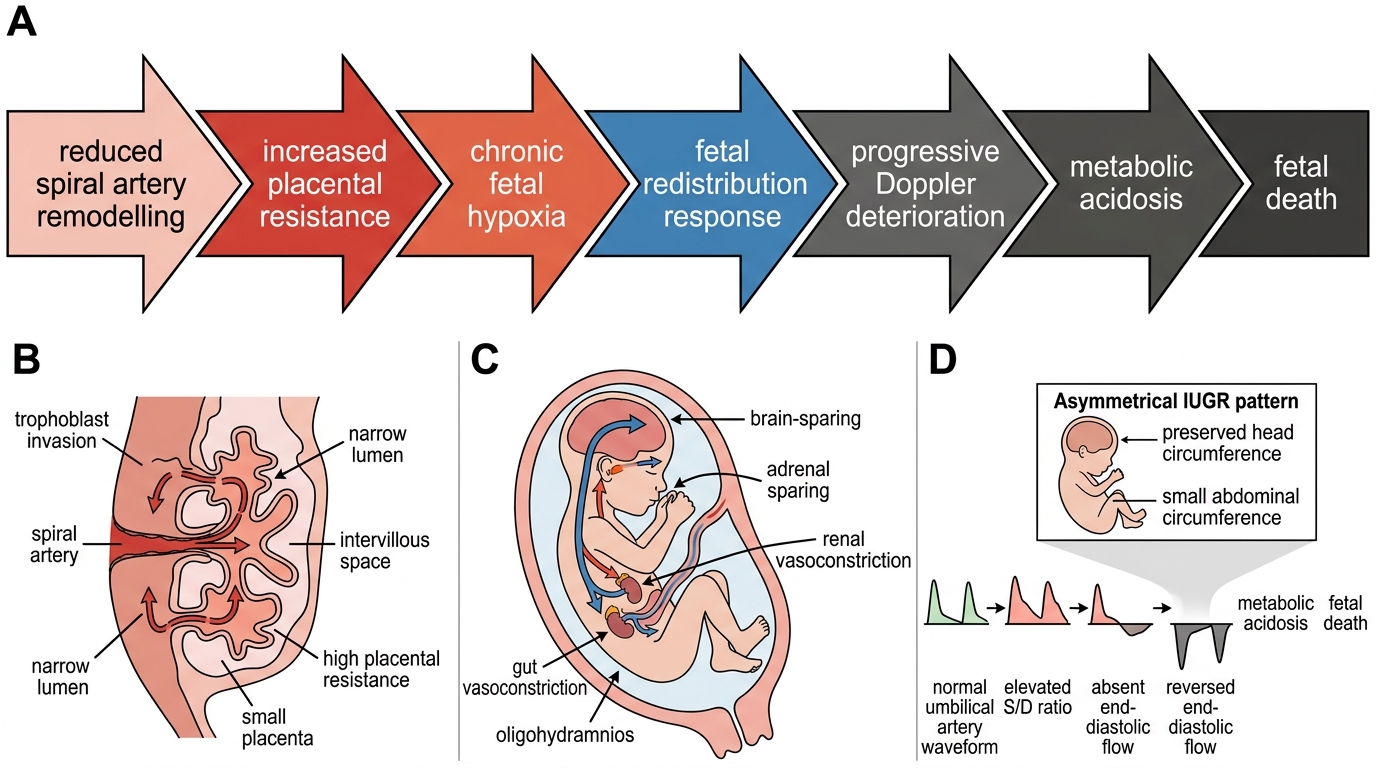
Uteroplacental Insufficiency Pathway in Asymmetrical IUGR
SELF-CHECK
A 28-week fetus has biometry showing head circumference on the 50th centile, abdominal circumference on the 4th centile, and femur length on the 40th centile. Amniotic fluid index is 4 cm. The umbilical artery shows elevated S/D ratio. Which type of IUGR does this pattern represent?
A. Symmetrical IUGR due to a chromosomal anomaly
B. Asymmetrical IUGR due to uteroplacental insufficiency
C. Constitutional smallness — no intervention needed
D. Macrosomia — abdominal circumference should be plotted separately
Reveal Answer
Answer: B. Asymmetrical IUGR due to uteroplacental insufficiency
This is the classic pattern of asymmetrical IUGR: head circumference is relatively preserved (50th centile) while abdominal circumference is disproportionately small (4th centile) with oligohydramnios (AFI 4 cm) and elevated UA resistance — all pointing to uteroplacental insufficiency and the brain-sparing response. Symmetrical IUGR would show proportionate reduction of all biometric parameters.
Diagnosis, Investigations, and Monitoring of Fetal Wellbeing
The diagnosis of IUGR integrates clinical assessment, ultrasound biometry, amniotic fluid evaluation, and Doppler surveillance into a structured surveillance protocol. No single test is sufficient — the clinical picture must be built progressively, with each abnormal finding prompting the next level of investigation.
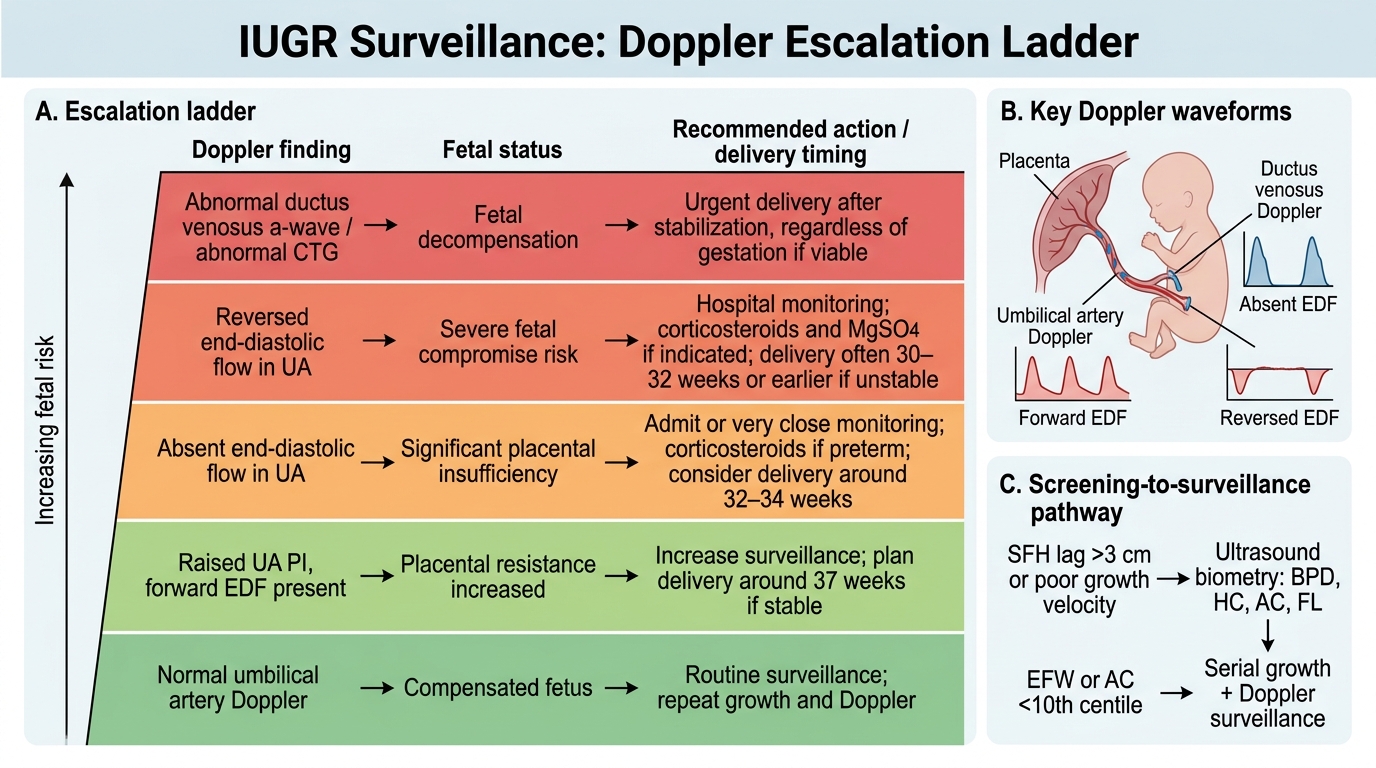
Clinical assessment begins with serial SFH measurements plotted on a customised chart. An SFH lagging by more than 3 cm below the expected value, or serial measurements demonstrating growth velocity below the 10th centile of the customised chart, triggers a referral for detailed ultrasound.
Ultrasound biometry is the cornerstone of IUGR diagnosis. The four key parameters are the biparietal diameter (BPD), head circumference (HC), abdominal circumference (AC), and femur length (FL). Estimated fetal weight (EFW) is derived using formulae (most commonly Hadlock) that incorporate two or more of these. IUGR is diagnosed when the EFW or AC falls below the 10th centile on a customised growth chart. A single measurement is insufficient; serial biometry at 2–4 week intervals establishes the growth velocity — a flattening curve (growth velocity below the normal range) is more predictive of adverse outcome than a single centile position. Amniotic fluid volume is assessed simultaneously: oligohydramnios (AFI ≤5 cm or deepest vertical pocket <2 cm) indicates reduced fetal renal perfusion and is a marker of moderate-to-severe compromise.
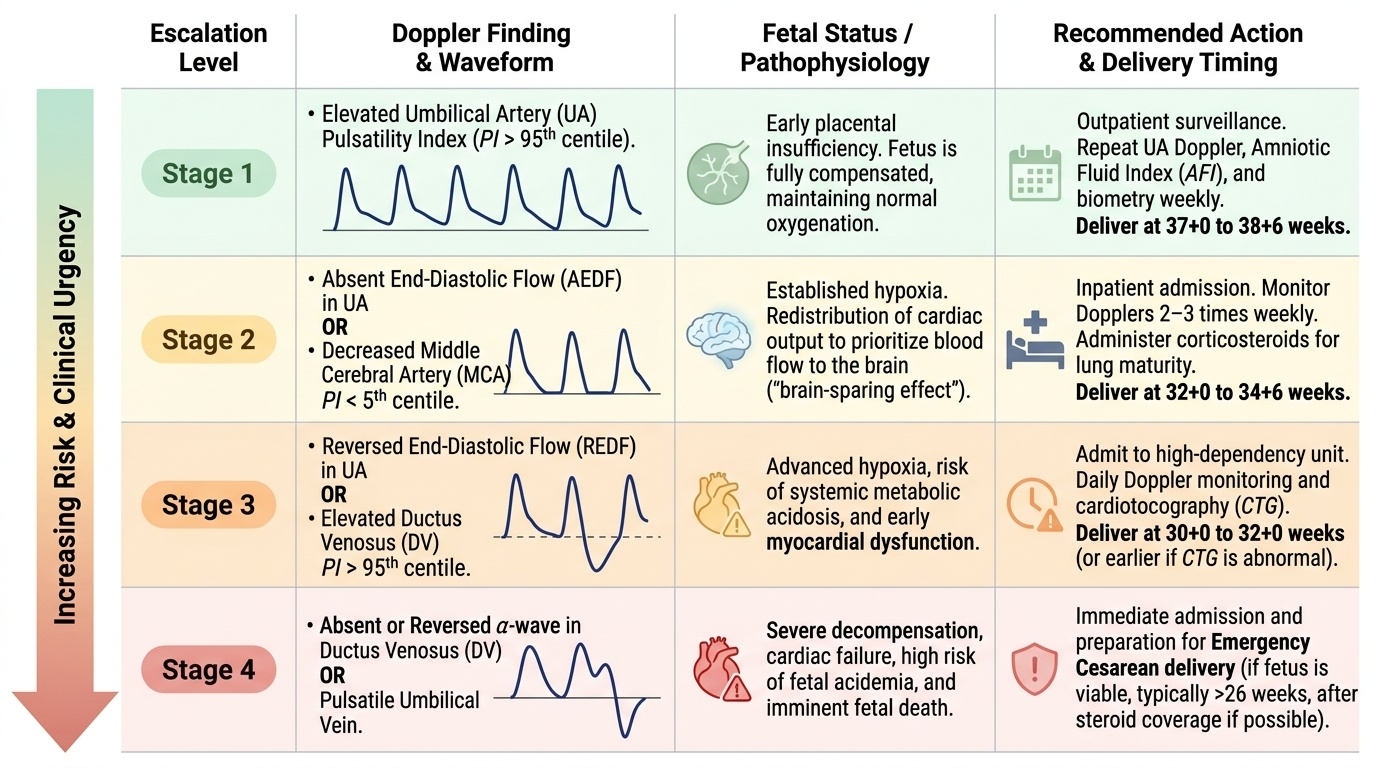
Doppler surveillance is the key tool for assessing fetal wellbeing in IUGR and follows a logical escalation from the umbilical artery outward to the venous circuit:
- Umbilical artery (UA) Doppler: reflects placental vascular resistance. As placental villous obliteration progresses, diastolic flow first rises in resistance (elevated PI/S:D ratio), then disappears (absent end-diastolic flow, AEDF), then reverses (reversed end-diastolic flow, REDF). AEDF appears when approximately 60–70% of placental villous vessels are obliterated; REDF indicates >70–80% obliteration. AEDF doubles perinatal mortality; REDF carries up to 10-fold increased risk of perinatal death. These findings mandate immediate escalation of surveillance.
- Middle cerebral artery (MCA) Doppler: measures cerebrovascular resistance. In brain-sparing, cerebral vasodilation occurs to maintain oxygen delivery to the brain, reducing the MCA pulsatility index. MCA PI below the 5th centile for gestation indicates significant cerebral redistribution. However, MCA alone is an imperfect predictor — it can normalise just before fetal demise (pseudo-normalisation).
- Cerebroplacental ratio (CPR): CPR = MCA PI / UA PI. A CPR below 1.0 (or below the 5th centile for gestational age) indicates that cerebral resistance has fallen to less than placental resistance — the brain-sparing threshold has been crossed. CPR is more sensitive than UA alone for identifying fetuses at risk of adverse outcomes, particularly in late-onset IUGR where UA Doppler may be normal despite significant compromise.
- Ductus venosus (DV) Doppler: the most ominous Doppler finding. The DV 'a' wave corresponds to atrial contraction; absent or reversed 'a' wave indicates elevated central venous pressure and right heart dysfunction — a pre-terminal finding reflecting imminent cardiac decompensation. DV abnormality precedes biophysical profile deterioration by hours to days and is the trigger for delivery in the TRUFFLE trial protocol.
Biophysical profile (BPP) combines five parameters: fetal breathing movements (≥1 episode of ≥30 seconds in 30 min), gross body movements (≥3 in 30 min), fetal tone (active limb flexion-extension), amniotic fluid volume (DVP ≥2 cm), and non-stress test (NST; reactive = ≥2 accelerations ≥15 bpm for ≥15 sec in 20 min). Each is scored 0 or 2; total 8–10 = normal, 6 = borderline (repeat in 24 hours), ≤4 = abnormal (consider immediate delivery). In IUGR, breathing movements are typically the last Doppler-independent parameter to be lost; tone is the most resistant.
Investigations for underlying cause should be considered in early-onset IUGR (before 32 weeks) where a treatable or recurrence-relevant aetiology may exist: full blood count and haematinics (anaemia), renal function, blood pressure, urine protein (hypertensive disorders), antiphospholipid antibodies (APS), TORCH serology, fetal karyotype (if structural anomaly or growth restriction with no obvious maternal/placental cause).
Provided image
IUGR Doppler Surveillance Escalation Ladder
SELF-CHECK
A 31-week growth-restricted fetus has UA Doppler showing absent end-diastolic flow (AEDF). The MCA PI is below the 5th centile. The BPP scores 6/10 (absent fetal breathing movements). Which statement best guides immediate management?
A. Discharge home with weekly UA Doppler — AEDF at 31 weeks is an expected finding
B. Admit, administer antenatal corticosteroids and MgSO4, arrange twice-weekly ductus venosus Doppler, and plan delivery when DV becomes abnormal or BPP ≤4
C. Immediate caesarean section — AEDF + abnormal MCA is an absolute indication for emergency delivery
D. Repeat BPP in 24 hours and discharge if it improves to 8/10
Reveal Answer
Answer: B. Admit, administer antenatal corticosteroids and MgSO4, arrange twice-weekly ductus venosus Doppler, and plan delivery when DV becomes abnormal or BPP ≤4
At 31 weeks with AEDF and brain-sparing (MCA PI <5th centile), the correct management is admission, corticosteroids for fetal lung maturation, MgSO4 neuroprotection, and close Doppler surveillance with ductus venosus monitoring. Delivery is triggered by DV abnormality or BPP ≤4, not by AEDF alone at this gestation — the risks of extreme prematurity must be weighed against in-utero hypoxia. Emergency immediate delivery is not warranted when the BPP is 6/10 (borderline, not severely abnormal) and DV is still normal.