Page 23 of 38
OG12.8 | Iso-Immunization in Pregnancy — SDL Guide (Part 2)
Prophylaxis and Management of Iso-Immunization
The management of iso-immunization in pregnancy is divided into two fundamentally different scenarios: (1) the non-sensitised Rh-negative woman, for whom the goal is prevention of sensitisation with anti-D immunoglobulin, and (2) the already-sensitised woman, for whom prophylaxis is futile and the goal shifts entirely to fetal surveillance and timely intervention.
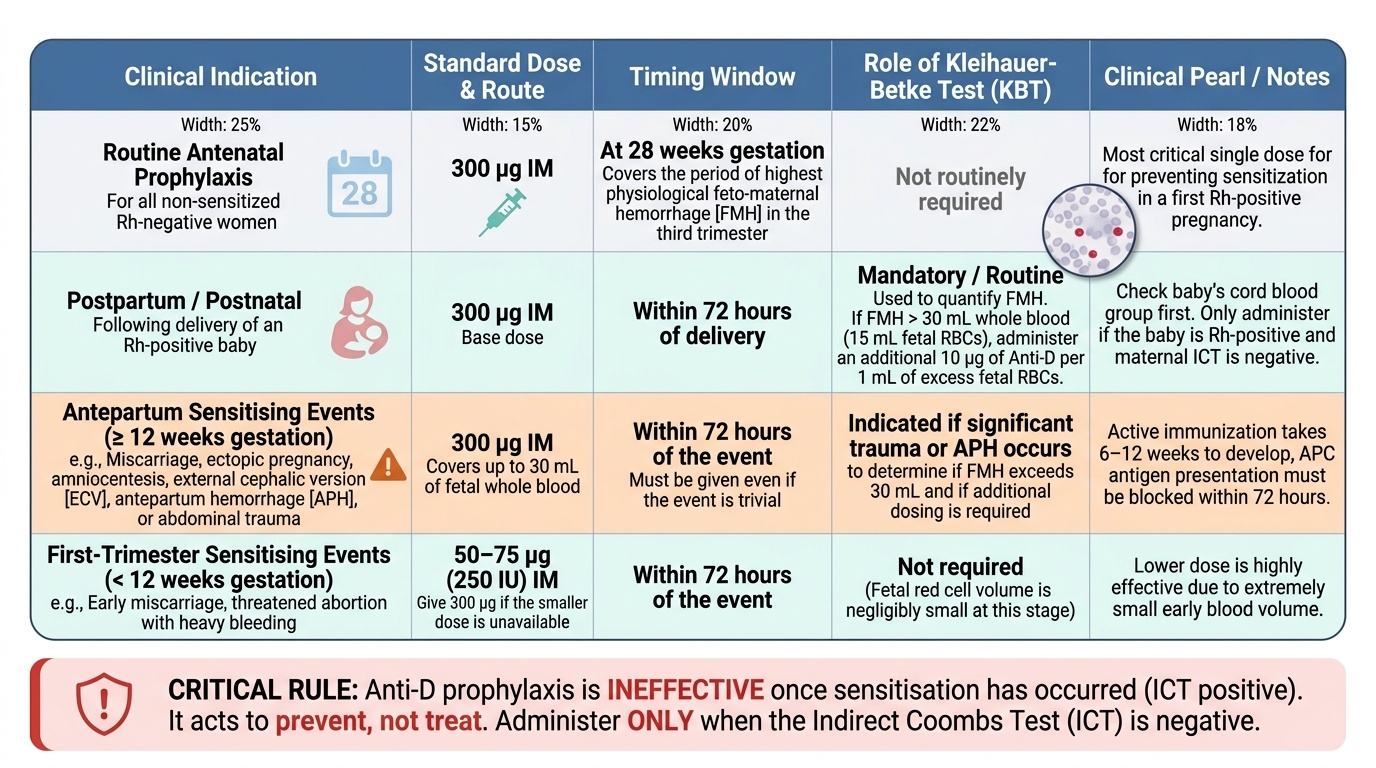
PROPHYLAXIS — Anti-D Immunoglobulin:
Anti-D immunoglobulin is a concentrated preparation of human polyclonal IgG anti-D antibodies derived from volunteer donors. Its mechanism is passive immunisation + clearance: the injected anti-D coats any fetal D-positive red cells in the maternal circulation before the mother's immune system can recognise them, targeting them for rapid splenic clearance — too fast for antigen-presenting cells to initiate a B-cell response. Prevention is thus a race against the primary immune response.
The standard dose is 300 µg IM — this covers up to 30 mL of fetal whole blood (15 mL fetal red cells). If the Kleihauer-Betke test shows FMH exceeding 30 mL, additional anti-D at 10 µg per 1 mL of excess fetal RBCs is given.
Prophylaxis schedule:
- Routine antenatal prophylaxis at 28 weeks gestation (300 µg): covers the period of highest physiological FMH in the third trimester; this is the most important single dose for preventing sensitisation in a first Rh-positive pregnancy
- Within 72 hours of any sensitising event (miscarriage ≥12 weeks, ectopic, amniocentesis, ECV, APH, trauma) — MUST be given even if the sensitising event is trivial; the 72-hour window is the time within which passive anti-D can prevent immunisation (the primary immune response takes 6–12 weeks, but the antigen-presenting cell induction can be blocked up to 72 h post-exposure)
- Within 72 hours of delivery of an Rh-positive baby — check cord blood group; if the baby is Rh-positive, give 300 µg (confirm with KBT; give more if FMH >30 mL)
- After first-trimester sensitising events (miscarriage <12 weeks, threatened abortion with heavy bleeding): 50–75 µg (or 250 IU) is sufficient at <12 weeks as fetal red cell volume is small; 300 µg given if available
CRITICAL RULE: Anti-D prophylaxis is INEFFECTIVE once sensitisation has already occurred (ICT positive). It must only be given when the ICT is negative — it prevents, it does not treat.
MANAGEMENT OF ESTABLISHED SENSITISATION:
For the ICT-positive woman, the management is surveillance-and-intervention:
- Serial ICT titres — 4-weekly until titre reaches 1:16 (critical titre), then MCA Doppler takes over as the primary surveillance tool
- MCA-PSV Doppler — serial measurements every 1–2 weeks from 24 weeks when titre ≥1:16; refer to tertiary centre with IUT capability
- Cordocentesis ± Intrauterine Transfusion (IUT): when MCA-PSV >1.5 MoM, cordocentesis confirms fetal haemoglobin. If fetal Hb <10 g/dL (or haematocrit <30%), IUT is performed: O-negative packed red cells (CMV-negative, irradiated) are transfused directly into the umbilical vein under ultrasound guidance. The target post-transfusion haematocrit is 40–50%. IUT can be repeated every 2–4 weeks as needed. The gestational window for IUT is 18–34 weeks; below 18 weeks the umbilical vein is too small; above 34 weeks early delivery is preferred.
- Timing of delivery: without IUT, aim for 37–38 weeks (avoiding prolonged intrauterine exposure); with IUT, delivery at 34–37 weeks after confirmation of fetal lung maturity (corticosteroids if <34 weeks).
NEONATAL MANAGEMENT (HDNB):
- Cord blood: Hb, bilirubin, DCT (Coombs), blood group
- Phototherapy for hyperbilirubinaemia (converts unconjugated bilirubin to water-soluble photoisomers)
- Exchange transfusion for rapidly rising bilirubin (>20 mg/dL or rising >1 mg/dL/h) or severe anaemia at birth (Hb <12 g/dL with hydrops): removes antibody-coated cells + bilirubin + maternal anti-D
- IVIG (intravenous immunoglobulin) may reduce exchange transfusion need in some centres by saturating Fc receptors on macrophages
Provided image
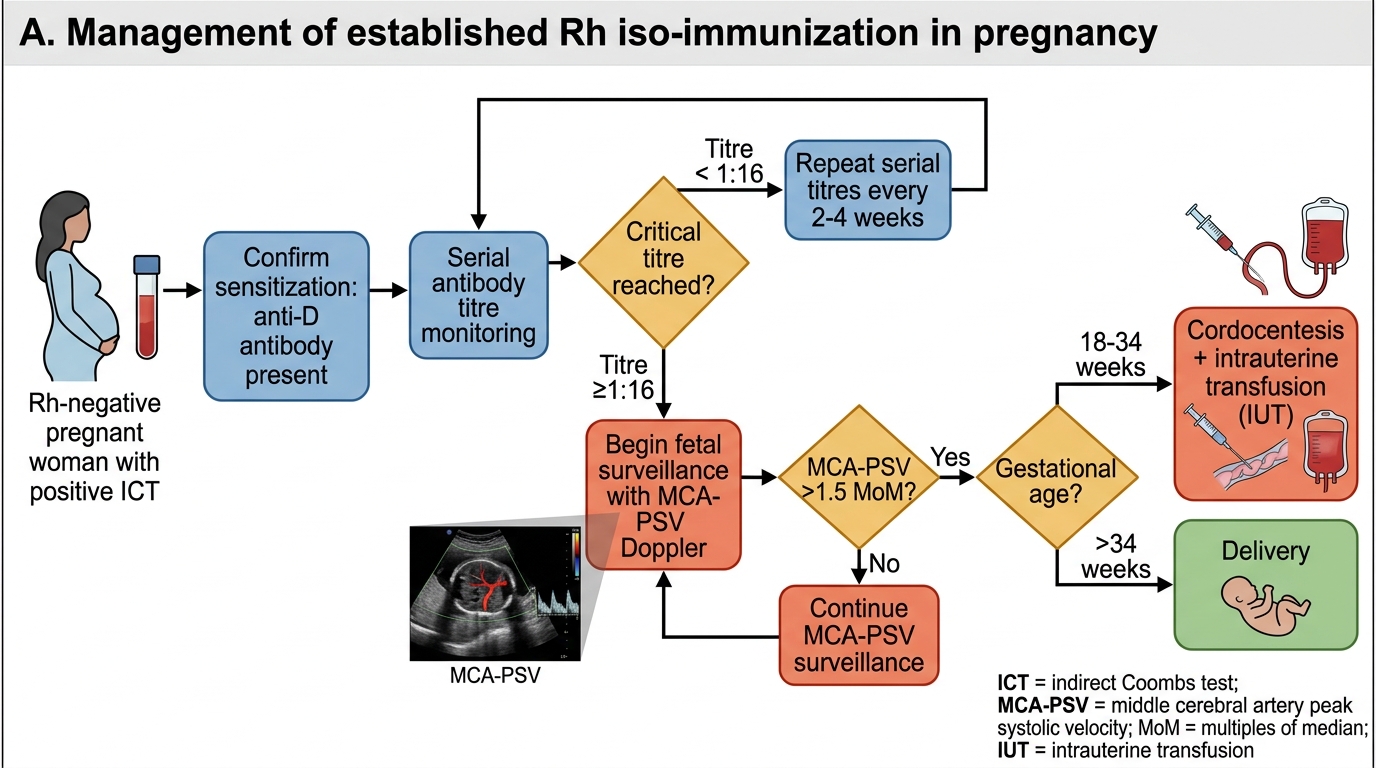
Management of Established Rh Iso-immunization
CLINICAL PEARL
The two cardinal rules: (1) Anti-D must be given within 72 hours of any sensitising event — and must NOT be given if ICT is already positive. The most common error is omitting anti-D after a first-trimester miscarriage at a peripheral facility; this one omission can condemn every subsequent Rh-positive pregnancy to severe haemolytic disease. (2) MCA-PSV Doppler has replaced the Liley curve (amniotic fluid optical density) as the primary non-invasive monitoring tool — it is more sensitive, avoids the risk of amniocentesis-induced further FMH, and should be available at every tertiary centre managing sensitised pregnancies. The critical titre of ≥1:16 is the threshold above which MCA-PSV takes precedence over antibody titres for fetal monitoring. A third teaching point: the 72-hour window for anti-D is not a hard biological absolute — there is evidence of partial effectiveness up to 10 days post-exposure, but 72 hours is the operational standard; beyond 72 hours in a previously unsensitised woman, anti-D should still be given if available rather than withheld.
SELF-CHECK
A Rh-negative woman undergoes amniocentesis at 18 weeks gestation. Her ICT is NEGATIVE. What should she receive?
A. No anti-D — the fetus may be Rh-negative, so prophylaxis is unnecessary
B. Anti-D 300 µg IM within 72 hours of the procedure
C. Anti-D is only needed after 28 weeks, not at 18 weeks
D. Anti-D only if Kleihauer-Betke confirms FMH >0.1 mL
Reveal Answer
Answer: B. Anti-D 300 µg IM within 72 hours of the procedure
Amniocentesis is a sensitising event because it involves a needle passing through the uterus and potentially the placenta, directly causing fetomaternal haemorrhage. Any sensitising procedure in a non-sensitised (ICT-negative) Rh-negative woman mandates anti-D 300 µg IM within 72 hours, regardless of gestational age or suspected fetal Rh status. Waiting for Kleihauer-Betke results is incorrect — anti-D should be given empirically; KBT is used to determine whether ADDITIONAL anti-D is needed above the standard 300 µg. Fetal Rh status is not checked before giving prophylaxis because the result may not be available within the 72-hour window.
SELF-CHECK
Kleihauer-Betke test on a postpartum Rh-negative woman shows 2% fetal cells. Maternal blood volume is assumed to be 5,000 mL. What volume of fetomaternal haemorrhage has occurred, and how much anti-D is required?
A. FMH = 100 mL; one standard 300 µg dose is adequate
B. FMH = 100 mL; additional anti-D required above the standard 300 µg dose
C. FMH = 10 mL; one standard 300 µg dose is adequate
D. FMH = 500 mL; multiple additional doses required
Reveal Answer
Answer: B. FMH = 100 mL; additional anti-D required above the standard 300 µg dose
FMH = (2/100) × 5,000 mL = 100 mL of fetal whole blood (or approximately 50 mL fetal red cells). The standard 300 µg anti-D dose covers only 30 mL of fetal whole blood. Since 100 mL > 30 mL, additional anti-D is required: calculate excess FMH above 30 mL = 70 mL, convert to fetal RBC volume = 35 mL, add 10 µg anti-D per 1 mL fetal RBCs = additional 350 µg (in practice, round up and give the next 300 µg vial, then recheck KBT after 1 hour to verify clearance).
Self-Assessment — Iso-Immunization in Pregnancy
The following scenarios test your clinical reasoning and application of the key decision points in the management of Rh iso-immunization in pregnancy. Each scenario isolates a different phase of the clinical journey — booking blood typing and ICT, a sensitising event requiring prophylaxis, established sensitization with rising MCA-PSV, and the neonatal presentation. Work through each one before checking the answers, paying particular attention to the precise timing of anti-D administration and the interpretation of the MCA-PSV threshold.
Scenario A: Meena is a 26-year-old G2P1 at 10 weeks gestation. She has vaginal bleeding and on ultrasound the fetus is found to have no cardiac activity — missed miscarriage confirmed. She is Rh-negative; her husband is Rh-positive. ICT is negative. She undergoes surgical uterine evacuation.
- Should she receive anti-D? If so, what dose and by when?
- Why does it matter that the ICT is negative before giving anti-D?
Scenario B: Divya is a Rh-negative woman at 34 weeks with a known sensitized pregnancy (ICT 1:32 at booking). Her weekly MCA-PSV Doppler shows 1.62 MoM this week.
- What is the next investigation and management step?
- If cordocentesis confirms fetal haemoglobin 7.2 g/dL, what procedure is indicated?
Scenario C: A baby is born to an Rh-negative mother; cord blood DCT is positive, serum bilirubin at 6 hours of life is 8 mg/dL and rising at 1.2 mg/dL/hour.
- At what bilirubin level would you consider exchange transfusion? What is the neonatal condition?
Self-check answers: A1: Yes — 300 µg anti-D IM within 72 hours of the procedure (uterine evacuation is a sensitising event; at 10 weeks, 300 µg is standard in India). A2: If ICT is positive, sensitization has already occurred — anti-D prophylaxis is futile and giving it is a waste of a scarce resource; anti-D only prevents sensitization, it does not treat it. B3: Cordocentesis (umbilical vein blood sampling under USS) to confirm fetal haemoglobin; IUT standby. B4: Intrauterine transfusion — fetal Hb 7.2 g/dL is significantly below the 10 g/dL threshold at 34 weeks; transfuse with O-negative irradiated packed red cells via umbilical vein under USS guidance; target haematocrit 40–50%. C5: Exchange transfusion threshold is typically total serum bilirubin >20 mg/dL in term infant or rising >1 mg/dL/h — bilirubin already rising at 1.2 mg/dL/h at 6 hours; phototherapy immediately + prepare for exchange transfusion if bilirubin trajectory continues. Condition: Haemolytic Disease of the Newborn (HDNB).