Page 26 of 38
OG12.9 | Thyroid Disorders in Pregnancy — SDL Guide (Part 2)
Management of Thyroid Disorders in Pregnancy
The management of thyroid disorders in pregnancy requires careful drug selection, frequent monitoring, and anticipation of neonatal complications that can arise from both the disease itself and from its treatment. The guiding principle for both hypothyroidism and hyperthyroidism is to maintain the mother in a euthyroid state as defined by trimester-specific TSH targets while minimising fetal exposure to teratogenic drugs or thyroid-suppressive drug effects. The two conditions require opposite therapeutic approaches — one involving hormone replacement and the other hormone suppression — but both demand equally vigilant monitoring because under-treatment and over-treatment each carry distinct fetal risks.
MANAGEMENT OF HYPOTHYROIDISM:
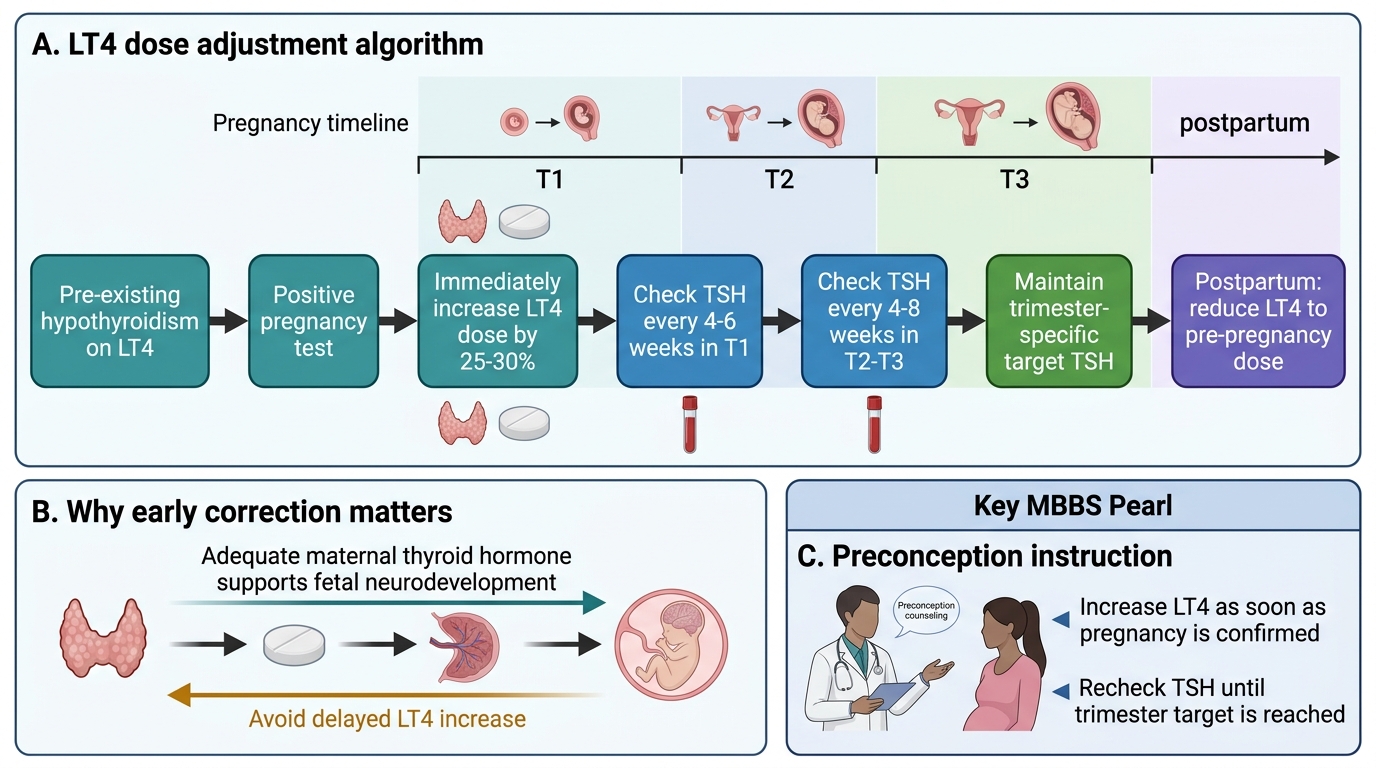
Levothyroxine (LT4) is the only treatment for hypothyroidism in pregnancy — it is safe, effective, and well-tolerated. All women with pre-existing hypothyroidism on LT4 must be counselled to increase their dose by approximately 25–30% as soon as pregnancy is confirmed (ideally a preconception counselling point). This increase is needed immediately because:
1. Rising TBG binds more T4, increasing the demand for total T4
2. Fetal iodine demands and placental T4 transfer increase T4 utilisation
3. The increase in GFR enhances LT4 clearance
For newly diagnosed hypothyroidism in pregnancy, the starting LT4 dose depends on severity: for subclinical hypothyroidism (mildly elevated TSH), start at 50–75 µg/day; for overt hypothyroidism, start at full replacement (1.6 µg/kg/day) and adjust rapidly. LT4 should be taken on an empty stomach (30–60 minutes before food) as calcium, iron, and antacids impair absorption.
Monitoring: TSH should be checked every 4–6 weeks in the first trimester and every 4–8 weeks in T2 and T3. The target TSH is within the trimester-specific range, with many guidelines aiming for TSH 0.5–2.5 mIU/L in T1. After delivery, the LT4 dose should be reduced to the pre-pregnancy level and TSH checked at 6 weeks postpartum — postpartum hypothyroid exacerbation (Hashimoto's postpartum flare) is common.
MANAGEMENT OF HYPERTHYROIDISM — Antithyroid Drugs:
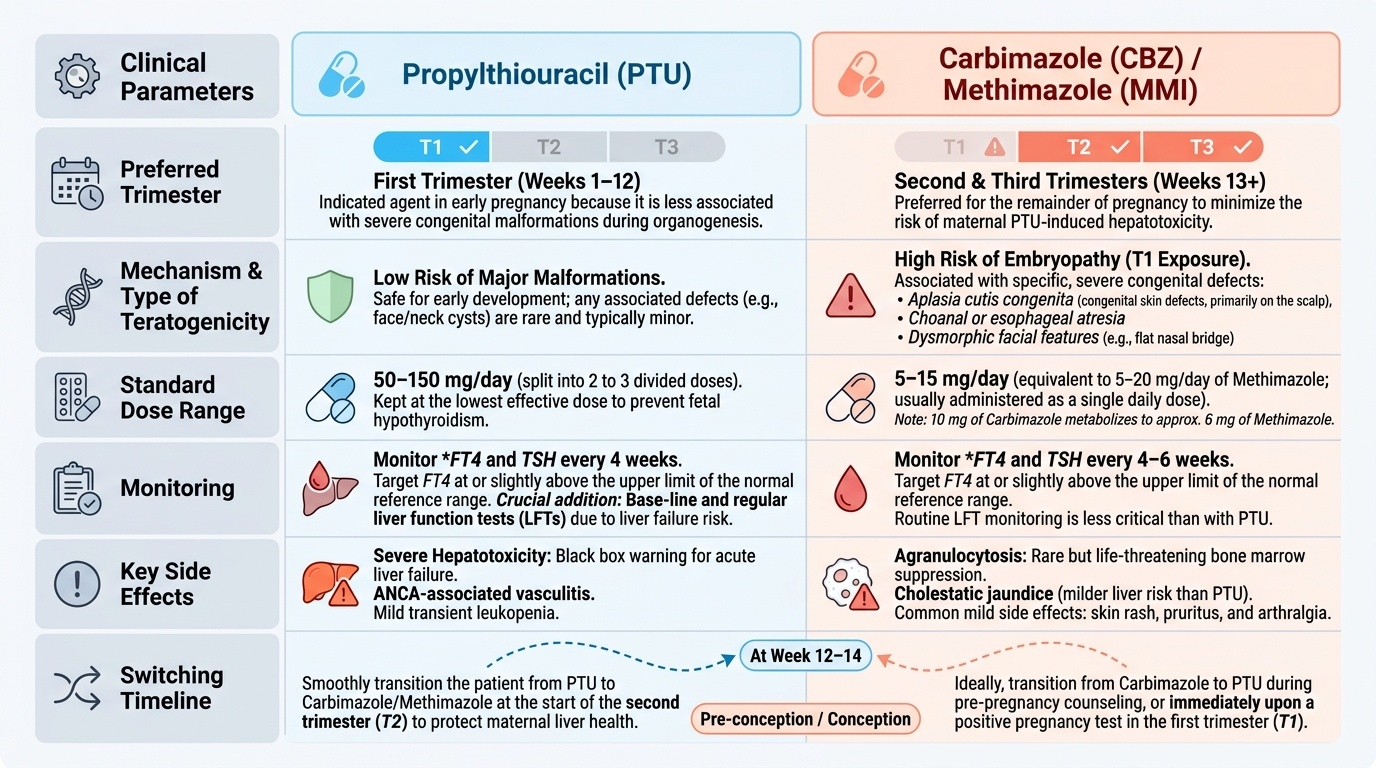
The choice of antithyroid drug in pregnancy is determined by trimester:
- First trimester → PTU (propylthiouracil) is preferred because methimazole (and its prodrug carbimazole) is teratogenic in T1: the specific defects are aplasia cutis (absent scalp skin), choanal atresia, oesophageal atresia, and methimazole embryopathy (a recognisable pattern of facial and cardiovascular defects). PTU does not share these teratogenic effects and is therefore preferred in T1 despite its hepatotoxicity risk.
- Second and third trimesters → switch to carbimazole or methimazole (equivalent potency per mg) because the teratogenic window has closed and the risk of PTU-induced hepatotoxicity (hepatic necrosis, potentially fatal) outweighs its benefits with prolonged use. Carbimazole is given at 15–40 mg/day initially and titrated down.
Titration target: maintain FT4 in the upper third of the normal range — the goal is to use the minimum effective dose of ATD because both PTU and carbimazole cross the placenta and can suppress the fetal thyroid (causing neonatal hypothyroidism if overtreatment occurs). The 'block-replace' regimen (ATD + LT4) is NOT recommended in pregnancy because ATD crosses the placenta but LT4 does not effectively compensate the fetus.
Beta-blockers (propranolol 10–40 mg TDS): for symptomatic control (palpitations, tremor) while awaiting ATD effect; not for long-term use (neonatal bradycardia risk with prolonged use).
Thyroid storm — emergency management:
Admit to ICU. Treat with: PTU 200–250 mg every 4–6 h (inhibits synthesis and peripheral conversion of T4→T3) + potassium iodide (Lugol's iodine — given 1 hour AFTER PTU to block hormone release) + propranolol IV + dexamethasone (reduces T4→T3 peripheral conversion + adrenal support) + cooling, IV fluids, and treatment of precipitating cause. Delivery once the mother is stabilised if close to term.
Gestational transient thyrotoxicosis: no ATDs needed; supportive care for hyperemesis; resolves spontaneously by 18–20 weeks.
Neonatal surveillance:
- Neonatal hypothyroidism risk: in women on ATD throughout pregnancy, neonatal thyroid function should be checked at birth and day 3–5 to detect transient hypothyroidism from transplacental ATD transfer
- Neonatal Graves' disease: if maternal TRAb >3× ULN at 36 weeks → TRAb crosses the placenta → neonatal thyroid is over-stimulated after birth; presents with tachycardia, irritability, poor feeding, goitre from 3–7 days of life (when maternal ATD clears from neonatal circulation); can persist 3–12 weeks; treat with ATD
Postpartum thyroiditis: occurs in 5–10% of all women, more commonly in those with anti-TPO positivity; a painless destructive thyroiditis presenting as transient hyperthyroid phase (weeks 1–4 postpartum) followed by hypothyroid phase (weeks 4–12); usually resolves by 12 months but 20–30% develop permanent hypothyroidism — requires TSH surveillance.
Provided image
Management of Pre-existing Hypothyroidism in Pregnancy
CLINICAL PEARL
Three practical pearls for thyroid disorders in pregnancy: (1) PTU in T1, switch to carbimazole in T2 — get the switch right. Carbimazole/methimazole causes aplasia cutis and methimazole embryopathy if given in organogenesis (weeks 6–10); PTU causes potentially fatal hepatic necrosis if given for months (liver function testing every 6 weeks while on PTU). The two drugs have different risk windows — PTU is the safer choice for the brief teratogenesis window, but carbimazole is safer for the long haul. (2) The fetal thyroid does not distinguish between maternal overtreatment with ATD and primary fetal hypothyroidism — fetal hypothyroidism from maternal overtreatment impairs fetal brain development just as maternal hypothyroidism does. Target FT4 in the upper normal range, use the minimum effective ATD dose, and check fetal growth and heart rate regularly. (3) A woman with pre-existing hypothyroidism on LT4 must increase her dose by 25–30% as soon as she has a positive pregnancy test — this instruction should be given at the preconception visit (or at the first ANC visit if she is already pregnant). Delay in recognising the increased need is the most common cause of untreated hypothyroidism in the critical first trimester.
SELF-CHECK
A woman with Graves' disease on carbimazole 30 mg/day is found to be 7 weeks pregnant. What change in management is most important?
A. Continue carbimazole — it is safe throughout pregnancy
B. Switch to PTU immediately — carbimazole is teratogenic in the first trimester
C. Stop all antithyroid drugs — they are all contraindicated in pregnancy
D. Switch to levothyroxine — it is safer than antithyroid drugs
Reveal Answer
Answer: B. Switch to PTU immediately — carbimazole is teratogenic in the first trimester
Carbimazole (and its active metabolite methimazole) is teratogenic in the first trimester — specific defects include aplasia cutis, choanal atresia, oesophageal atresia, and methimazole embryopathy. The organogenesis window is weeks 6–10. At 7 weeks, she is within this critical window and must be switched to PTU immediately. PTU does not share these teratogenic effects. Stopping ATDs entirely risks maternal thyroid storm and fetal exposure to uncontrolled thyrotoxicosis. Levothyroxine does not treat hyperthyroidism — it replaces thyroid hormone, not suppresses its overproduction.
SELF-CHECK
A woman with Graves' disease has TRAb levels 5× upper limit of normal at 36 weeks gestation (despite controlled FT4/FT3 on ATD). What does this predict and what action should be taken?
A. Maternal relapse — increase ATD dose immediately
B. Neonatal Graves' disease — alert the neonatologist and plan neonatal thyroid surveillance
C. Fetal growth restriction — organise additional growth scans
D. No clinical significance — TRAb levels do not predict neonatal outcomes
Reveal Answer
Answer: B. Neonatal Graves' disease — alert the neonatologist and plan neonatal thyroid surveillance
TRAb (TSH-receptor antibodies) cross the placenta via IgG transport. High maternal TRAb (>3× ULN) at 36 weeks predicts a significant risk of neonatal Graves' disease: TRAb persists in the neonatal circulation after birth and stimulates the neonatal thyroid, causing thyrotoxicosis 3–7 days after birth (when maternal ATD has cleared). The neonatologist must be alerted, and the neonate requires thyroid function monitoring (TSH + FT4 on day 3–5 of life). If neonatal Graves' develops, it is treated with low-dose ATD and resolves within 3–12 weeks as maternal TRAb is cleared.
Self-Assessment — Thyroid Disorders in Pregnancy
The scenarios below are designed to test your ability to apply trimester-specific TSH reference ranges, make the PTU-vs-carbimazole switch decision correctly, and identify when the fetus or neonate requires additional surveillance. These are the types of questions that appear in written examinations and clinical viva assessments — where a single wrong drug choice (carbimazole in T1) or a missed dose increase (LT4 in first trimester) will distinguish a strong clinical student from a borderline one. Work through each scenario systematically before checking the answers.
Scenario A: Lekha, a 30-year-old G1, has been on levothyroxine 75 µg/day for Hashimoto's hypothyroidism. She presents at 6 weeks gestation. Her pre-pregnancy TSH was 1.8 mIU/L. She has not changed her LT4 dose since learning of the pregnancy.
- What change do you make to her LT4 dose and why?
- When should her TSH next be checked?
Scenario B: Fatima, 28 weeks pregnant, has Graves' disease. She has been on PTU 200 mg TDS since 6 weeks gestation. Her liver enzymes are now elevated (ALT 85 IU/L, AST 72 IU/L). FT4 is in the upper normal range. TRAb is 2× ULN.
- What change in ATD should be made at 28 weeks?
- Is the TRAb level at 28 weeks clinically significant for neonatal planning?
Self-check answers: A1: Increase LT4 by 25–30% — to approximately 100 µg/day (75 × 1.3 = 97.5 µg, round to 100 µg); this is needed immediately because TBG rises within weeks of conception, increasing T4 demand. A2: TSH in 4–6 weeks (first-trimester monitoring interval). B3: Switch from PTU to carbimazole at 28 weeks — PTU's teratogenic window (T1) has passed; PTU hepatotoxicity risk increases with prolonged use (months); carbimazole is now the safer choice. B4: TRAb at 28 weeks is 2× ULN — below the 3× threshold for high neonatal Graves' risk; reassuring but re-check TRAb at 36 weeks; if still elevated, alert neonatologist for neonatal surveillance at day 3–5.