Page 13 of 38
OG12.5 | Urinary Tract Infection in Pregnancy — SDL Guide
Learning Objectives
- Describe the clinical features of asymptomatic bacteriuria (ASB), acute cystitis, and acute pyelonephritis in pregnancy
- Explain how pregnancy modifies the urinary tract to increase susceptibility to infection
- Describe the impact of UTI on pregnancy outcomes including preterm birth and maternal sepsis
- Outline the management of UTI in pregnancy including antibiotic selection, ASB screening, and pyelonephritis treatment
INSTRUCTIONS
Urinary tract infection is the most common bacterial infection encountered in pregnancy, affecting 2–10% of women as asymptomatic bacteriuria alone. Its importance in obstetric care lies not in the lower urinary symptoms but in the 20–40% risk of progression to acute pyelonephritis when left untreated — a complication that can cause maternal sepsis, preterm labour, and stillbirth. This module gives you the clinical framework to screen, diagnose, and treat UTI at every stage of its presentation.
References
- DC Dutta's Textbook of Obstetrics, 9th edition, Chapter 14 (textbook)
- Williams Obstetrics, 26th edition, Chapter 53 (textbook)
- RCOG and NICE Guidelines on UTI in Pregnancy (2019 update) (guideline)
- Kass EH. Bacteriuria and the diagnosis of infections of the urinary tract. Arch Intern Med 1957 (research)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Lakshmi is a 28-year-old primigravida, 14 weeks pregnant, attending her booking antenatal visit. She has no complaints — no dysuria, no frequency, no fever. A mid-stream urine culture is sent as part of routine antenatal screening. Three days later, the laboratory reports Escherichia coli at 100,000 CFU/mL. She is completely well and asks why she needs antibiotics. The answer to her question — that this silent infection carries a 20–40% risk of escalating to acute pyelonephritis during her pregnancy, with potentially serious consequences for both her and her baby — is the core lesson of this module. Understanding why pregnancy is uniquely permissive for bacterial ascent in the urinary tract, and what that means for screening, diagnosis, and treatment, is a daily antenatal care competency.
WHY THIS MATTERS
Urinary tract infection (UTI) is the most common serious bacterial infection encountered during pregnancy, with a prevalence of 2–10% for asymptomatic bacteriuria alone. Its clinical importance is disproportionate to its apparent mildness: while an isolated positive urine culture in a non-pregnant woman might be observed rather than treated, in pregnancy it demands prompt antibiotic therapy. The rationale — established by Kass's landmark studies in the 1960s and confirmed by multiple Cochrane reviews — is that untreated asymptomatic bacteriuria progresses to acute pyelonephritis in 20–40% of pregnant women, compared with only 1–2% in the non-pregnant state. Acute pyelonephritis in pregnancy carries the risk of gram-negative sepsis, acute respiratory distress syndrome (ARDS), preterm labour (triggered by endotoxin-mediated prostaglandin release), and perinatal mortality. A three-day course of antibiotics at the asymptomatic stage prevents this cascade — making UTI screening one of the most cost-effective interventions in routine antenatal care.
RECALL
Before exploring UTI in pregnancy, recall from anatomy and physiology: the female urethra is approximately 4 cm long, located in close proximity to the rectum and perineum — both of which are colonised by faecal bacteria, particularly E. coli; the ureters carry urine from the renal pelvis to the bladder through smooth-muscle peristalsis; the vesicoureteral junction normally acts as a one-way valve preventing reflux from the bladder to the kidneys. In a non-pregnant woman, the short urethra makes retrograde ascent of bacteria from the perineum to the bladder relatively easy; normal voiding and ureteral peristalsis then wash bacteria before they can colonise the upper tract. In pregnancy, as you will see, these defence mechanisms are specifically impaired — explaining the dramatically increased risk of upper UTI.
Clinical Presentation of UTI in Pregnancy
Urinary tract infection in pregnancy encompasses three distinct clinical entities that represent a spectrum from clinically silent to life-threatening, and each must be recognised and managed differently. The three forms differ in their symptoms, physical signs, urine findings, systemic features, and the urgency of treatment, though they share the same underlying microbiology — predominantly Gram-negative enteric bacteria, with Escherichia coli accounting for approximately 80% of cases across all three presentations.
1. Asymptomatic bacteriuria (ASB) is the most prevalent form and the clinical entity that most distinguishes obstetric from non-obstetric management. By definition, ASB produces NO urinary symptoms — no dysuria, no frequency, no suprapubic discomfort — and no systemic features of infection. It is detectable only on urine culture. The diagnosis requires a mid-stream urine (MSU) culture demonstrating ≥100,000 colony-forming units (CFU/mL) of a single uropathogen on two consecutive specimens (or a single specimen if collected by catheter). The prevalence in pregnancy is 2–10%; it is higher in women with diabetes, sickle cell trait, urinary tract anomalies, and lower socioeconomic status.
2. Acute cystitis (symptomatic lower UTI) is characterised by the classical lower urinary tract symptoms — dysuria, frequency, urgency, and suprapubic discomfort or pain — without fever or systemic illness. These symptoms overlap with the normal urinary frequency and nocturia of pregnancy (due to uterine pressure on the bladder), making clinical distinction difficult; urine dipstick and culture are required to confirm infection. Acute cystitis occurs in 1–3% of pregnancies.
3. Acute pyelonephritis (upper UTI — renal infection) represents the most serious form and an obstetric emergency. It typically presents with:
- High fever (>38.5°C) with rigors and chills
- Loin or flank pain (unilateral or bilateral) with costovertebral angle tenderness on examination
- Nausea and vomiting, general malaise
- Lower urinary tract symptoms may or may not be present
- Tachycardia, signs of systemic sepsis in severe cases
Pyelonephritis complicates approximately 1–2% of all pregnancies; the right side is more commonly affected (compression of the right ureter by the dextrorotated pregnant uterus). It represents the most common non-obstetric cause of hospitalisation in pregnancy.
| Feature | Asymptomatic Bacteriuria | Acute Cystitis | Acute Pyelonephritis |
|---|---|---|---|
| Urinary symptoms | None | Dysuria, frequency, urgency | May be present |
| Suprapubic pain | None | Present | Absent or mild |
| Fever | None | None | High fever >38.5°C |
| Loin pain | None | None | Present; CVA tenderness |
| Systemic illness | None | None | Often severe |
| Urine WBCs | Variable | Positive | Strongly positive |
| Urine culture | ≥10⁵ CFU/mL | ≥10⁵ CFU/mL | ≥10⁵ CFU/mL |
| Treatment urgency | Outpatient, 7 days | Outpatient, 7 days | Inpatient IV antibiotics |
Pathophysiology — Effect of Pregnancy on the Urinary Tract
The dramatic increase in the risk of upper urinary tract infection (pyelonephritis) in pregnant women with untreated bacteriuria — from 1–2% in non-pregnant women to 20–40% in pregnancy — is not coincidental; it is the direct consequence of specific anatomical and physiological changes that pregnancy imposes on the urinary tract at multiple levels simultaneously. These changes collectively impair the normal defence mechanisms that prevent bacterial ascent from the bladder to the renal pelvis: normal ureteral peristalsis, which washes bacteria downward with each urinary bolus; the competent vesicoureteral junction, which prevents reflux; and the regular complete bladder emptying that removes colonising bacteria before they can multiply to a critical density. When all of these defences are simultaneously weakened by the hormonal and mechanical effects of pregnancy, the ascent of a perineal commensal bacterium — principally E. coli — from bladder to ureter to renal pelvis becomes far more likely than in the non-pregnant state. Understanding each mechanism individually, and recognising how they compound one another, is essential for understanding both why screening is necessary and why treatment of even asymptomatic bacteriuria is mandatory. (pyelonephritis) in pregnant women with untreated bacteriuria — from 1–2% in non-pregnant women to 20–40% in pregnancy — is not a coincidence; it is the direct consequence of specific anatomical and physiological changes that pregnancy imposes on the urinary tract. Understanding these mechanisms is essential for explaining to students and patients why ASB that would be observed in a non-pregnant woman must be treated in pregnancy.
Pregnancy-Induced Predisposing Factors for UTI
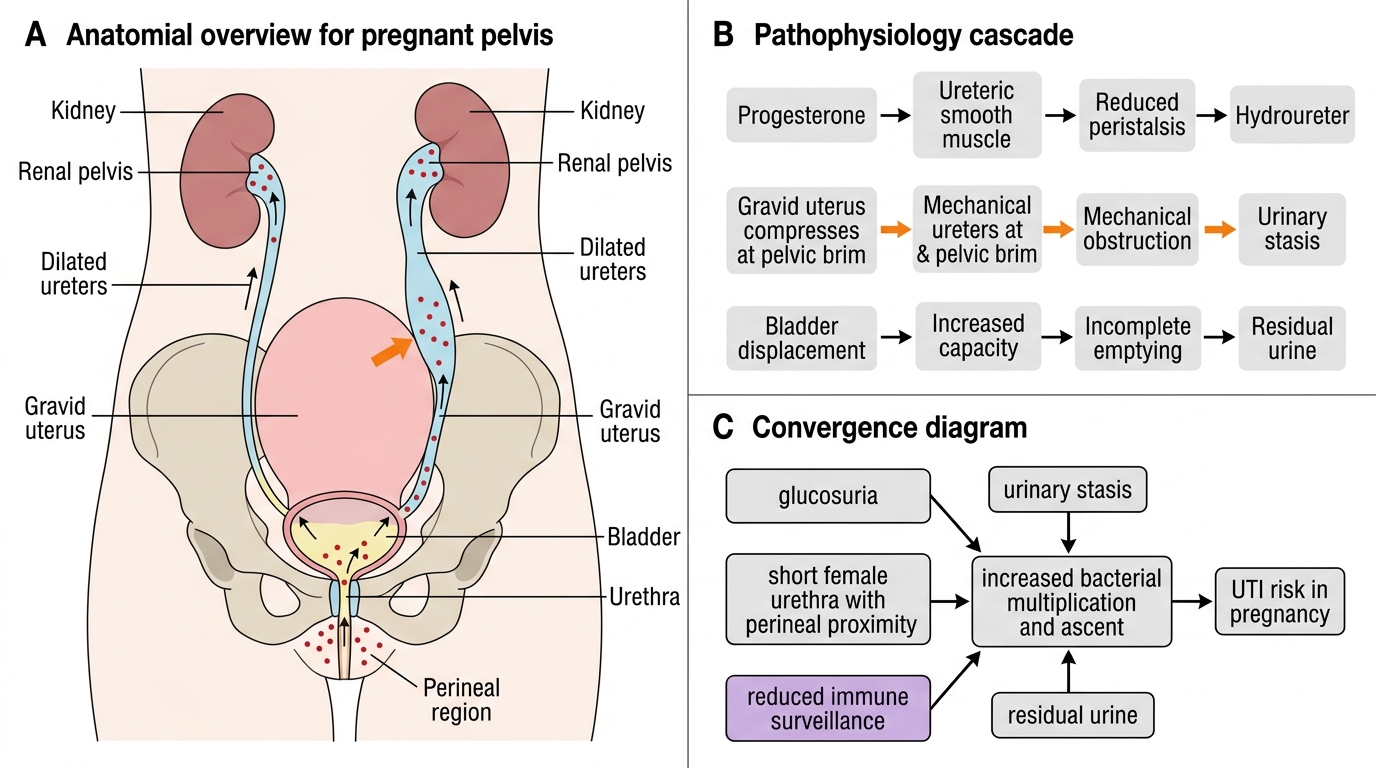
The key pathophysiological mechanisms are:
1. Physiological hydronephrosis and hydroureter:
- Progesterone causes smooth muscle relaxation throughout the body, including the ureteric smooth muscle; ureteric tone and peristaltic contractions diminish, reducing the urine flow that normally flushes bacteria from the ureter before they colonise the renal pelvis
- The enlarged pregnant uterus compresses the ureters at the pelvic brim (more pronounced on the right side, where the uterus is dextrorotated); this creates mechanical obstruction and bilateral hydroureter/hydronephrosis, detected in up to 90% of pregnant women on ultrasound by the third trimester
- Ureteric stasis creates a static column of urine in the dilated ureter — an ideal environment for bacterial multiplication and ascending infection
2. Increased bladder capacity and reduced emptying:
- The bladder is displaced anteriorly and superiorly by the growing uterus; bladder capacity increases and voiding efficiency reduces, promoting residual urine volumes
- Residual urine acts as a culture medium for ascending bacteria
3. Glucosuria:
- The increased glomerular filtration rate (GFR) of pregnancy (rising 50% above baseline) exceeds the tubular reabsorptive capacity for glucose, producing physiological glucosuria in many pregnant women
- Glucose in the urine is a growth-promoting medium for E. coli and other uropathogens
4. Vesicoureteral reflux:
- The altered angle of ureteric entry into the bladder wall (due to uterine displacement) and the increased bladder volume during pregnancy may impair the flap-valve mechanism at the vesicoureteral junction, permitting retrograde reflux of bacteria-laden urine toward the kidneys
5. Immunological changes:
- Pregnancy is a state of relative immunological suppression (necessary to tolerate the semi-allogeneic foetus); reduced cell-mediated immunity decreases local mucosal defence against uropathogens
Collectively, these changes explain why bacteria that might be cleared by normal voiding and ureteral peristalsis in a non-pregnant woman can ascend unchecked to the renal pelvis in pregnancy, causing pyelonephritis. The right kidney is more commonly affected because the right ureter experiences greater mechanical compression from the dextrorotated pregnant uterus.
Investigations and Diagnosis
The investigation of UTI in pregnancy requires a methodical approach that escalates in intensity according to the clinical presentation. At the screening end of the spectrum, a first antenatal visit requires only a mid-stream urine (MSU) culture — a rapid, cheap, and highly informative test that identifies bacteriuria before it has caused any symptoms. At the acute end of the spectrum, a febrile woman with loin pain, tachycardia, and rigors requires blood cultures, a full septic screen including renal function, and close foetal monitoring. The guiding principle is proportionality: over-investigation of simple ASB wastes resources and causes unnecessary anxiety, while under-investigation of severe pyelonephritis risks missing life-threatening complications such as bacteraemia, AKI, and ARDS. The following investigation plan moves from rapid point-of-care tests through to the full inpatient work-up required for the most severe presentations, and includes the screening protocol that should be applied routinely to all pregnant women at their antenatal visits. that moves from rapid screening tests to definitive microbiological diagnosis. The specific investigations required depend on the clinical severity — a well woman with positive dipstick at an antenatal clinic needs a urine culture and, at most, outpatient antibiotics; a febrile, tachycardic woman with loin pain needs urine culture, blood cultures, a full septic screen, and IV antibiotics as an inpatient. Understanding this graduated approach prevents both under-investigation of serious infection and over-investigation of simple ASB.
A. Urine dipstick (rapid screening test)
A urine dipstick tests for:
- Nitrites: produced when Gram-negative bacteria (especially E. coli, Klebsiella) reduce dietary nitrates to nitrites; high specificity for Gram-negative UTI but low sensitivity (a negative nitrite does NOT exclude infection, particularly with Gram-positive organisms)
- Leucocyte esterase: enzyme released by white blood cells; indicates pyuria; sensitive but not specific (false positives from contamination, vaginal secretions)
- The combination of positive nitrite AND leucocyte esterase has a positive predictive value of approximately 75–80% for significant bacteriuria; urine culture is still required for definitive diagnosis and antibiotic sensitivity
B. Mid-stream urine (MSU) culture — the gold standard
- Patient instructed on clean-catch technique: cleanse labia, start voiding, then collect the middle portion of the stream — reducing perineal contamination
- Diagnostic threshold for significant bacteriuria: ≥100,000 CFU/mL (10⁵ CFU/mL) of a single uropathogen
- Mixed growth with multiple organisms at lower counts typically represents contamination
- Sensitivity and susceptibility testing must accompany diagnosis to guide antibiotic selection
C. Screening protocol for ASB in pregnancy
- Routine MSU culture at the first antenatal (booking) visit for ALL pregnant women — this is the universal screening recommendation (unlike in non-pregnant women where ASB is not routinely treated)
- Repeat culture at 28 weeks in high-risk women (previous UTI, diabetes, urinary tract anomaly, sickle cell trait)
- Some guidelines recommend repeating culture each trimester in high-risk groups
D. Additional investigations for acute pyelonephritis
- Blood cultures (before starting antibiotics): bacteraemia occurs in approximately 20% of cases of pyelonephritis
- Full blood count: leucocytosis (neutrophilia); thrombocytopaenia in severe sepsis
- Serum creatinine and electrolytes: acute kidney injury occurs in up to 20% of pyelonephritis in pregnancy (due to endotoxin-mediated renal vasoconstriction)
- C-reactive protein (CRP): elevated; useful to monitor treatment response
- Renal ultrasound: if diagnosis is in doubt (to exclude renal abscess, obstructive uropathy, calculi); not routinely required for uncomplicated pyelonephritis
- Chest X-ray: in severely ill women (ARDS risk — endotoxin-mediated acute lung injury complicates severe pyelonephritis in 2–8% of cases)
E. Foetal monitoring
In acute pyelonephritis: CTG to assess for foetal heart rate changes associated with maternal fever and sepsis; ultrasound assessment if preterm contractions suspected.
SELF-CHECK
A 22-week pregnant woman has a routine MSU culture showing Escherichia coli at 100,000 CFU/mL. She has no urinary symptoms and is completely well. The correct management is:
A. Reassure her and repeat the culture in 4 weeks — this is likely a contaminant
B. Treat with a 7-day course of appropriate antibiotics (asymptomatic bacteriuria requires treatment in pregnancy)
C. Order an IV urogram to exclude structural urinary tract disease
D. Treat only if she develops symptoms in the next 2 weeks
Reveal Answer
Answer: B. Treat with a 7-day course of appropriate antibiotics (asymptomatic bacteriuria requires treatment in pregnancy)
Asymptomatic bacteriuria (≥100,000 CFU/mL of a single organism) MUST be treated in pregnancy, regardless of the absence of symptoms. The risk of progression to acute pyelonephritis without treatment is 20–40%, compared with 1–2% in non-pregnant women. This is one of the key differences between obstetric and non-obstetric management of bacteriuria. A 7-day course of an antibiotic guided by sensitivities (cefalexin or nitrofurantoin if not at term) is standard. Post-treatment test-of-cure culture at 2 weeks is recommended to confirm eradication.