Page 8 of 22
OG14.3 | Malpresentation and Malposition — SDL Guide (Part 2)
Management of Each Malpresentation
Management of each malpresentation is determined by the type of presentation, gestational age, fetal wellbeing, pelvic adequacy, and the availability of skilled operators. The overarching principle is to identify malpresentation antenatally whenever possible, as antenatal management (particularly ECV for breech) offers a window to convert to vertex before labour, avoiding the emergency element entirely. A structured approach — confirm the presentation on ultrasound, check for contraindications to version or vaginal delivery, counsel the woman about the options and risks with their probabilities, and make a shared decision about the delivery route — is the best framework. Different malpresentations have very different prognoses: breech at term is manageable with ECV or CS; a mentum posterior face in labour is a surgical emergency; a transverse lie with ruptured membranes is a cord prolapse crisis. Recognising which scenario you are in, and responding appropriately, is what this section consolidates.
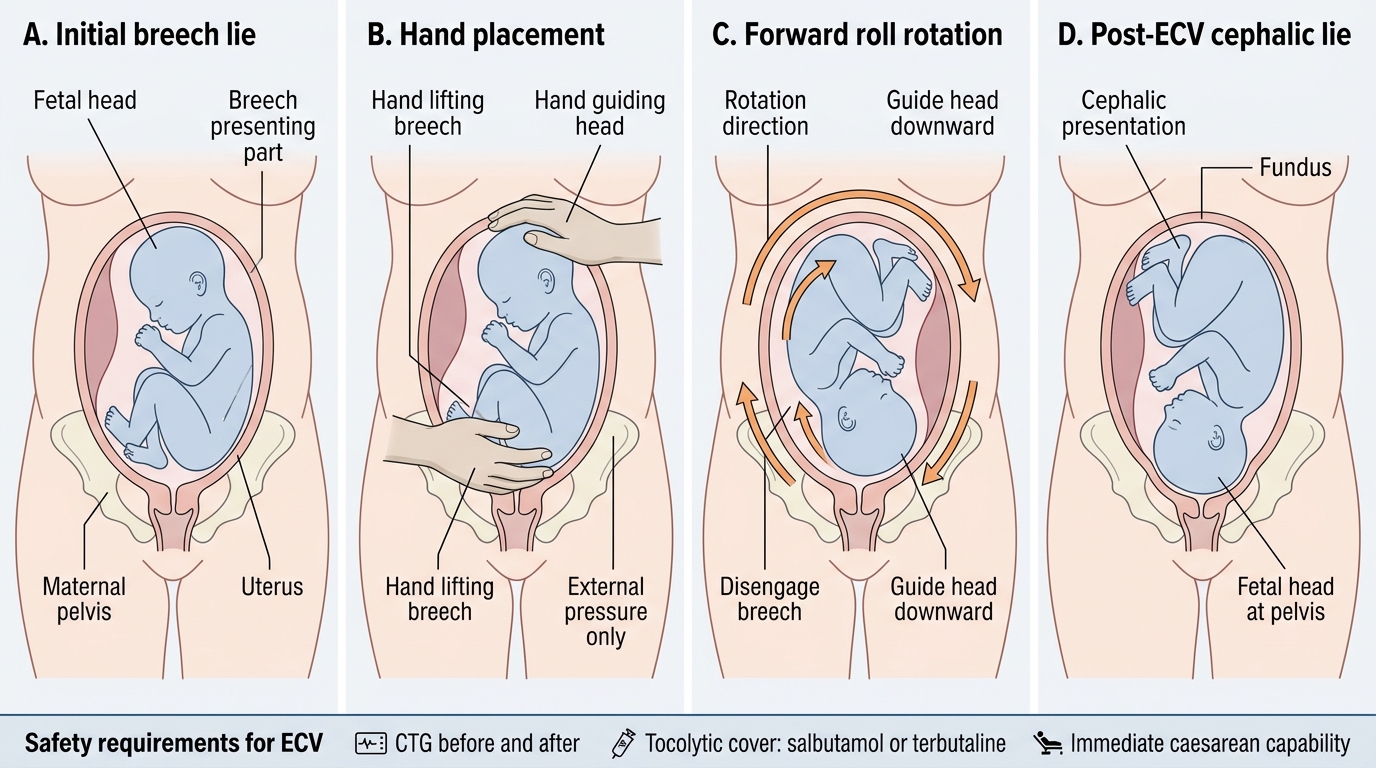
Breech presentation — antenatal management: At 36 weeks, any breech should be offered External Cephalic Version (ECV), which converts the presentation from breech to cephalic by external manipulation of the fetus through the maternal abdomen. ECV is offered from 36 weeks in nulliparas and 37 weeks in multiparas (RCOG guideline). The overall success rate is approximately 50–60%, higher in multiparas. Contraindications to ECV include:
- Absolute: placenta praevia, antepartum haemorrhage, ruptured membranes, evidence of fetal compromise, uterine anomaly
- Relative: previous CS scar, oligohydramnios, multiple pregnancy, severe pre-eclampsia, engagement of the breech
External Cephalic Version: Step-by-Step
ECV requires continuous CTG before and after the procedure, a setting with immediate CS capability, and should be performed with tocolytic cover (salbutamol or terbutaline IM to relax the uterus). If ECV succeeds, the woman can await spontaneous labour onset as a vertex. If ECV fails, the options are: elective CS (most common choice in high-resource settings, particularly following the Term Breech Trial evidence), or carefully selected vaginal breech delivery by an experienced operator (frank or complete breech, adequate pelvis, normal fetal weight, experienced team, woman's informed choice).
Breech in labour: If breech labour is underway and delivery is imminent, the key principles of assisted breech delivery are: allow the breech to deliver spontaneously to the umbilicus (hands-off until this point), then assist delivery of the shoulders and aftercoming head using Lovset's manoeuvre (shoulder delivery by rotation) and the Mauriceau-Smellie-Veit manoeuvre (delivery of the aftercoming head by jaw flexion + suprapubic pressure). The Burns-Marshall technique (body held by the feet and swung in an arc) is an alternative for the aftercoming head. The umbilical cord must not be allowed to compress between the head and the pelvis for more than 5 minutes — this causes fetal asphyxia.
Face presentation: Mentum anterior can deliver vaginally with patience — the chin sweeps under the pubic symphysis and the head delivers by flexion. Mentum posterior is an absolute indication for CS. If a mentum anterior is identified in labour, allow progress with CTG monitoring; no augmentation. Mentum posterior — proceed to CS.
Brow presentation: Almost always requires CS. May convert to either vertex or face during labour — if conversion occurs and the new presentation is deliverable, vaginal delivery may proceed. Without conversion, the mentovertical diameter (~13.5 cm) cannot negotiate most pelvic inlets.
Transverse/oblique lie: CS is mandatory unless ECV can convert the lie to cephalic before or in very early labour. Cord prolapse is the main intrapartum emergency — if membranes rupture with a shoulder or arm presenting, cord prolapse is imminent and emergency CS is required.
Occipitoposterior Position and Malposition
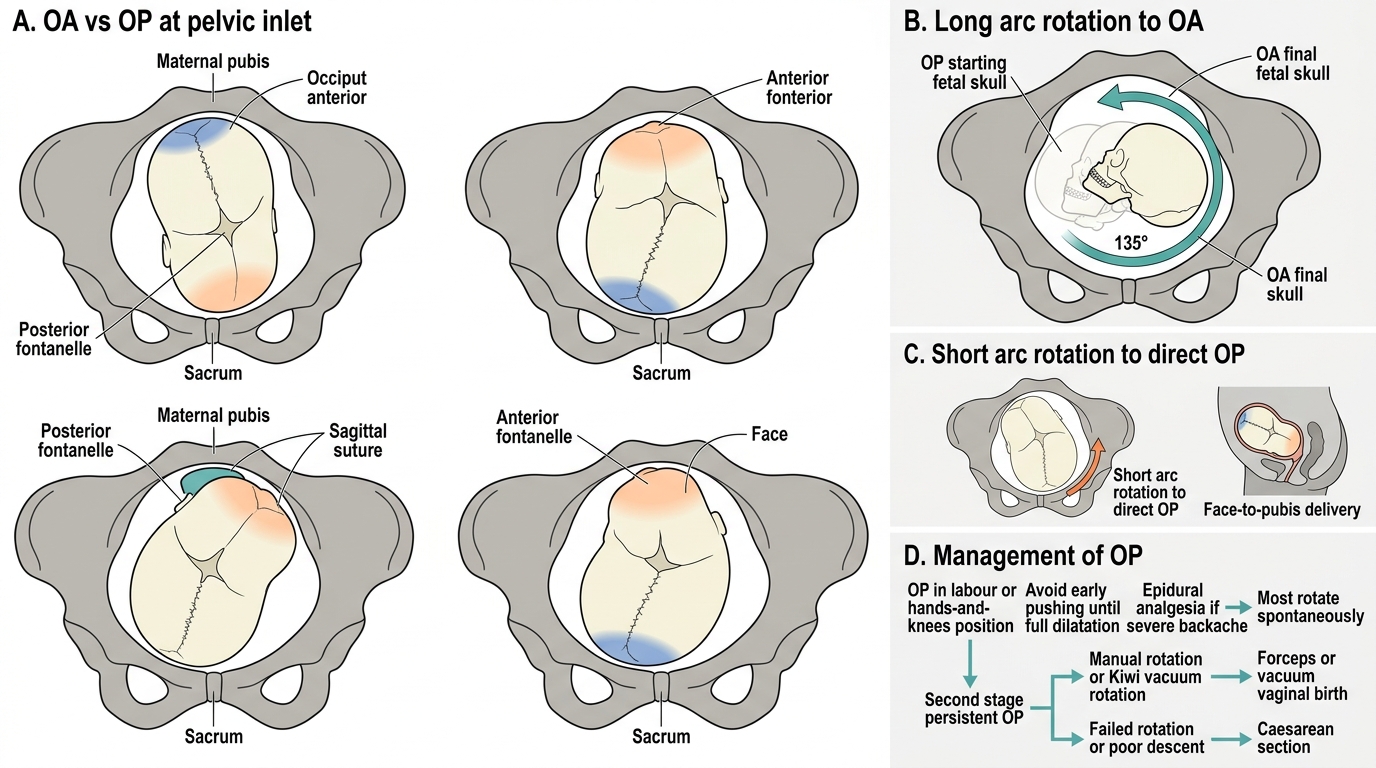
Occipitoposterior (OP) position is the most common malposition, present in approximately 5% of labours at onset. In OP, the fetal occiput faces the maternal sacrum instead of the pubic symphysis, and the fetus faces forward (face to pubis). It results in a slightly larger presenting diameter, posterior deflexion, and a more difficult fit through the pelvis, making labour longer, more painful (intense backache), and more likely to require intervention.
The majority of OP positions (approximately 65–70%) rotate spontaneously to occipitoanterior (OA) during labour, either through a long arc rotation (135° rotation from OP to OA) or by a short arc rotation (45° rotation to direct OP with face-to-pubis delivery). Long arc rotation is more common and typically occurs during the second stage. Approximately 5–10% of labours reach the second stage with persistent OP, requiring either manual rotation, vacuum or forceps rotation, or delivery in the direct OP position (face-to-pubis).
Clinical recognition: On vaginal examination, the anterior fontanelle (diamond-shaped, four suture lines) is felt anteriorly; the posterior fontanelle (triangular, three suture lines) is at or near the sacrum. Backache is severe and labour is often prolonged with slow progress in the active phase. The woman frequently experiences an urge to push early (before full dilatation) due to the fetal head pressing on the posterior perineum.
Occipitoposterior and Occipitoanterior Positions: Rotation Pathways and Management
Management of OP: Encourage the woman to adopt lateral or hands-and-knees positions, which may facilitate anterior rotation. Avoid early pushing — the cervix may not be fully dilated despite the urge. Epidural analgesia is appropriate for the severe backache. Most OP positions will rotate with conservative management. In the second stage with persistent OP, vacuum extraction with rotation (Kiwi cup) or manual rotation followed by forceps or vacuum delivery can achieve vaginal birth. If rotation fails and descent is inadequate, CS is appropriate.
SELF-CHECK
A woman in active labour at 7 cm complains of severe backache. Vaginal examination reveals the anterior fontanelle anteriorly and the head deflexed. CTG is normal. What is the most appropriate management?
A. Proceed to immediate emergency CS for abnormal presentation
B. Augment with oxytocin at the highest tolerated dose to expedite delivery
C. Encourage lateral or hands-and-knees positioning, provide epidural analgesia, and allow labour to progress with CTG monitoring
D. Perform immediate internal rotation and forceps delivery at 7 cm
Reveal Answer
Answer: C. Encourage lateral or hands-and-knees positioning, provide epidural analgesia, and allow labour to progress with CTG monitoring
The findings describe an occipitoposterior (OP) position — anterior fontanelle anteriorly, deflexion, backache. This is a malposition, not a malpresentation. The majority of OP positions rotate spontaneously to OA. At 7 cm with a normal CTG, the appropriate management is conservative: encourage position changes (lateral or hands-and-knees to facilitate anterior rotation), analgesia, and close monitoring. Immediate CS, high-dose oxytocin, and forceps at 7 cm are all inappropriate.
SELF-CHECK
Which of the following is an absolute contraindication to external cephalic version (ECV)?
A. Frank breech at 37 weeks in a nullipara with normal CTG and normal AFI
B. Placenta praevia with a breech presentation at 36 weeks
C. A previous lower-segment CS in a woman with breech at 36 weeks
D. Fetal weight estimated at 3.6 kg on ultrasound
Reveal Answer
Answer: B. Placenta praevia with a breech presentation at 36 weeks
Placenta praevia is an absolute contraindication to ECV — manipulating the uterus with a low-lying placenta risks catastrophic antepartum haemorrhage. A previous transverse LUS scar is a relative (not absolute) contraindication — ECV is cautiously offered in some guidelines. Frank breech at 37 weeks with normal CTG and AFI in a nullipara is the ideal candidate. Estimated fetal weight of 3.6 kg is not a contraindication, though macrosomia may lower the success rate.
Clinical Application and Self-Assessment
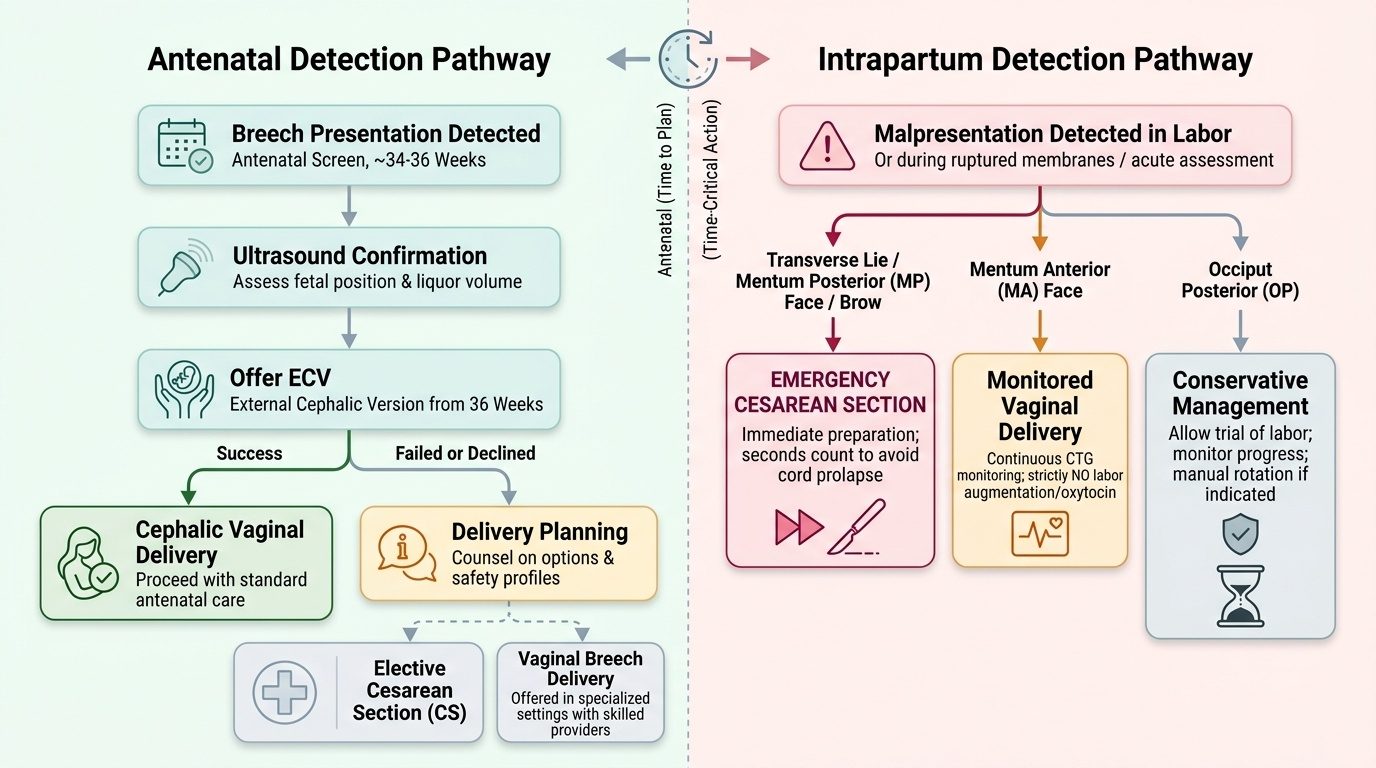
Synthesising the knowledge from this module requires thinking about malpresentation as a clinical problem that spans both the antenatal and intrapartum periods — not just a labour-room emergency to react to, but a condition that can be anticipated, screened for, and often corrected before labour begins. The clinician who detects breech at 34 weeks has time — time to counsel, time to attempt ECV at 36 weeks, time to plan elective CS if ECV fails. The clinician who first detects a transverse lie in a woman with ruptured membranes and a prolapsed cord has seconds. Both are malpresentation scenarios, but they demand entirely different responses and different clinical skills. Final-year students must be fluent in both ends of this spectrum: the unhurried antenatal counselling conversation and the emergency decision to proceed to immediate CS.
Provided image
A practical synthesis across malpresentation types:
- Breech at term: offer ECV from 36 weeks; if fails or declined → elective CS (most settings) or vaginal breech in a specialised setting
- Mentum anterior face: allow vaginal delivery with CTG monitoring; no augmentation
- Mentum posterior face: emergency CS — no vaginal delivery is possible
- Brow: almost always CS; await possible conversion in early labour
- Transverse/shoulder: CS mandatory unless ECV early in labour converts to cephalic; membranes must not be ruptured
- OP position: conserve — position change, analgesia, patience; instrumental rotation or CS only for persistent OP in second stage with failure to descend
CLINICAL PEARL
When examining for malpresentation, remember the denominator mnemonics: vertex = occiput (O), face = mentum (M/Ch), breech = sacrum (S), shoulder = acromion (A). In face presentation, the key decision is mentum anterior (MA) vs mentum posterior (MP): MA can deliver vaginally (chin under symphysis, head delivers by flexion); MP cannot (chin faces sacrum, head cannot flex further — CS is mandatory). A useful bedside test: if you can feel the mouth clearly with hard gum pads on both sides on vaginal examination, determine which way the chin faces by finding the malar (cheek) bones and the nose — if the chin is anterior, the nose points toward the sacrum.