Page 5 of 22
OG14.2 | Rupture Uterus — SDL Guide (Part 2)
Management of Uterine Rupture
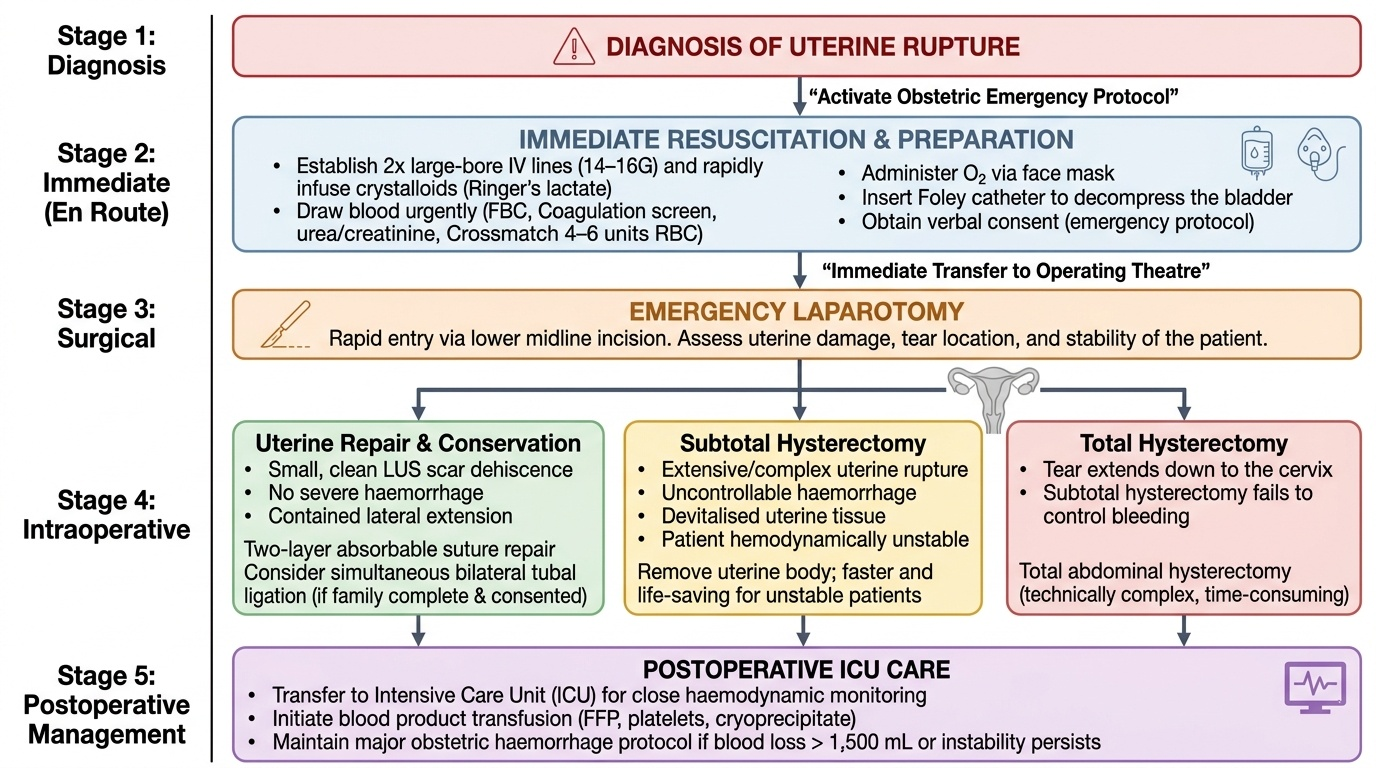
Management of uterine rupture is simultaneous resuscitation and emergency surgery — the two cannot be sequential because time is the critical variable. Every minute of delay translates directly into worse maternal and perinatal outcomes. The surgical decision — repair vs hysterectomy — is made in the operating theatre based on what is found at laparotomy, not before.
Immediate resuscitation: Call for help — activate the obstetric emergency protocol. Establish two large-bore IV cannulae (14–16G). Draw blood urgently for full blood count, coagulation screen, urea/creatinine, group and crossmatch (4–6 units packed red cells). Infuse crystalloid (Ringer's lactate) rapidly. Administer O₂ by face mask. The patient must be in theatre within minutes, so resuscitation is conducted en route to the operating theatre. Foley catheter to decompress the bladder. Consent may need to be verbal in an emergency.
Surgical management: The abdomen is opened (lower midline incision for fastest access in emergency) and the findings assessed:
- Repair with conservation: For small, clean LUS scar dehiscence without haemorrhage, or a contained lateral extension, the tear can be repaired with two layers of absorbable suture. Tubal ligation is often performed simultaneously if the family is complete, with informed consent.
- Subtotal (supracervical) hysterectomy: When the rupture is extensive, bleeding is uncontrollable, or uterine tissue is devitalised, the uterus must be removed to save the mother's life. Subtotal hysterectomy is faster than total and may be life-saving in a haemodynamically unstable patient.
- Total hysterectomy: Required when the tear extends to the cervix or when subtotal hysterectomy does not control bleeding; technically more difficult and time-consuming.
Provided image
Blood product transfusion is almost always required — major obstetric haemorrhage protocols should be activated early (typically when estimated blood loss exceeds 1,500 mL or haemodynamic instability persists). Fresh frozen plasma, platelets, and cryoprecipitate may be needed if disseminated intravascular coagulation (DIC) develops. Postoperative intensive care with close monitoring of urine output, coagulation, and haemodynamic status is mandatory.
Prevention and Self-Assessment
Prevention of uterine rupture requires a two-pronged approach: preventing the underlying causes (particularly obstructed labour and injudicious oxytocin use, addressed in the obstructed labour module), and careful risk stratification and counselling of women with uterine scars. As caesarean section rates continue to rise globally, the latter is increasingly the dominant preventive challenge.
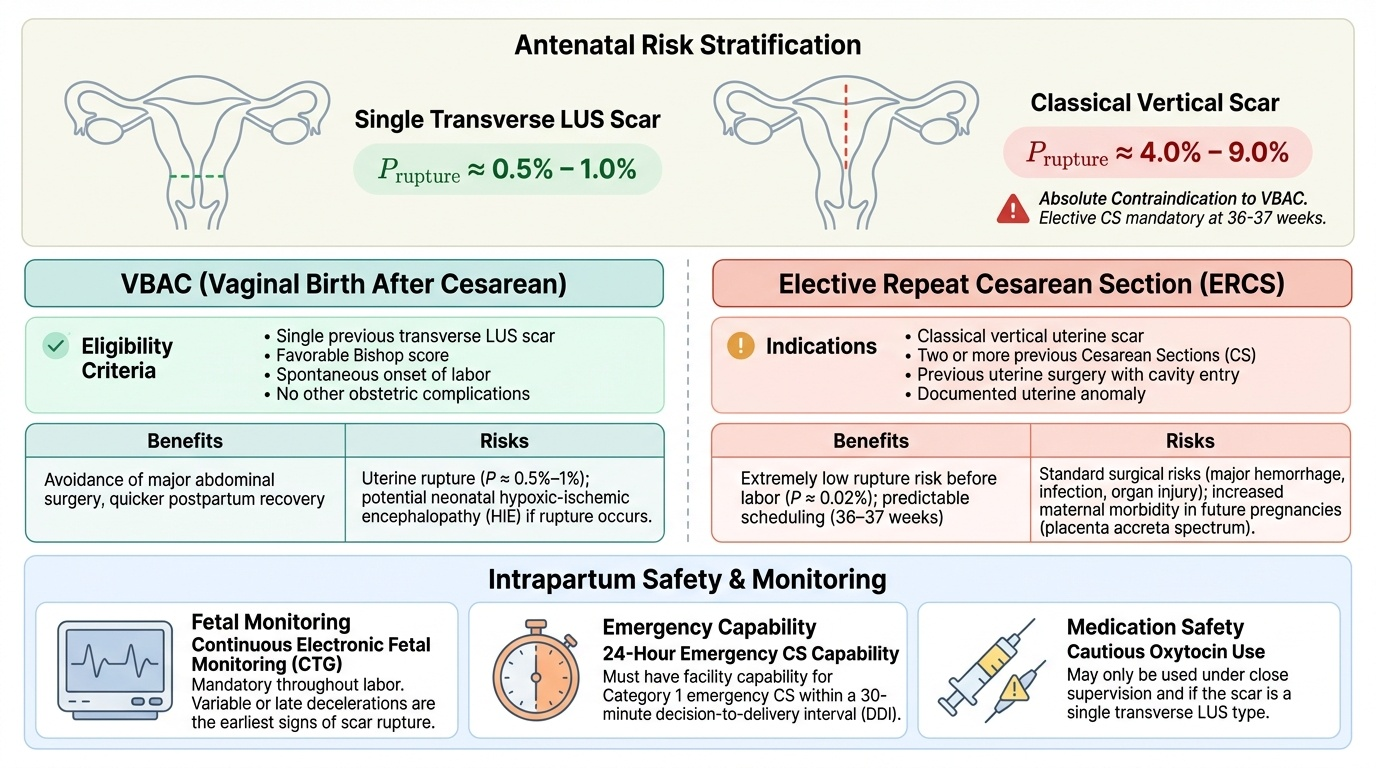
Antenatal risk stratification for scarred uterus: All women with a previous uterine scar must be counselled about the rupture risk associated with VBAC versus elective repeat CS. The risk of uterine rupture in VBAC labour after a single previous transverse lower-segment CS is approximately 0.5–1% — low, but real, and significantly higher than after elective repeat CS (0.02%). A previous classical vertical CS has a much higher rupture risk (4–9%) and is an absolute contraindication to VBAC — elective repeat CS is mandatory, typically at 36–37 weeks before onset of labour. Women with two or more previous CS, previous uterine surgery with cavity entry, or a documented uterine anomaly should also undergo elective CS. Conversely, women with a single previous transverse LUS scar, a favourable Bishop score, spontaneous onset of labour, and no other obstetric complications are reasonable VBAC candidates with appropriate informed consent and intrapartum monitoring.
Intrapartum monitoring in VBAC: VBAC labour must be conducted in a facility with 24-hour capability for emergency CS within 30 minutes (Category 1 decision-to-delivery interval). Continuous electronic fetal monitoring (CTG) is mandatory throughout VBAC labour — the earliest sign of scar rupture is often a CTG abnormality (variable or late decelerations). Oxytocin may be used cautiously in VBAC if the scar is a single transverse LUS scar, but with a lower dose ceiling and greater vigilance than for an unscarred uterus; prostaglandins are contraindicated for cervical ripening in a scarred uterus due to the risk of uterotonic hyperstimulation.
Provided image
Preventing unscarred-uterus rupture: This requires the same measures as preventing obstructed labour — universal partograph use, skilled birth attendance, timely referral, and avoiding oxytocin augmentation in the presence of malpresentation or CPD. Grand multiparas (≥5 previous deliveries) have a uterine wall prone to thinning and should be monitored with heightened caution during labour, with very conservative oxytocin use if augmentation is needed.
SELF-CHECK
Which of the following is an absolute contraindication to VBAC (trial of labour after previous caesarean)?
A. Single previous transverse lower-segment CS with spontaneous onset of labour
B. Previous classical (vertical) uterine incision
C. Bishop score of 6 at 39 weeks in a VBAC candidate
D. Maternal age above 35 years with previous LSCS
Reveal Answer
Answer: B. Previous classical (vertical) uterine incision
Previous classical (vertical) CS carries a uterine rupture risk of 4–9% in labour — far higher than the 0.5–1% for a transverse LUS scar. Classical CS is an absolute contraindication to VBAC; elective repeat CS at 36–37 weeks before labour onset is mandatory. A single previous transverse LUS scar with spontaneous labour and a favourable Bishop score is a reasonable VBAC candidate, as is a woman over 35 with no other risk factors.
SELF-CHECK
At laparotomy for suspected uterine rupture, you find a 4 cm lateral extension of the LUS incision with active arterial haemorrhage. The patient is G3P2 and haemodynamically unstable despite resuscitation. What is the most appropriate surgical management?
A. Primary repair of the tear with two-layer closure and uterine conservation
B. Subtotal (supracervical) hysterectomy to control haemorrhage
C. Total abdominal hysterectomy as the first choice in all ruptures
D. Packing the uterus with gauze and closing the abdomen
Reveal Answer
Answer: B. Subtotal (supracervical) hysterectomy to control haemorrhage
A haemodynamically unstable patient with extensive rupture and active haemorrhage requires subtotal hysterectomy — the fastest effective surgical option. Subtotal hysterectomy removes the uterine body (the site of bleeding) while leaving the cervix, reducing operative time compared to total hysterectomy. Simple repair is inappropriate when the tear is extensive and haemostasis cannot be achieved conservatively. Total hysterectomy is preferred when the tear extends to the cervix. Uterine packing is not a definitive treatment for rupture.
CLINICAL PEARL
The most dangerous feature of scar rupture is its subtlety. Unlike the dramatic presentation of unscarred-uterus rupture, an LUS scar may separate silently — without abdominal pain or maternal haemodynamic change — and the first clue may be a prolonged CTG deceleration or a drop in the baseline FHR. In VBAC labour, treat any unexplained CTG abnormality as scar rupture until proven otherwise. The cost of a false-positive emergency CS is an unnecessary operation; the cost of a missed rupture is maternal and fetal death.