Page 3 of 17
OG16.1 | Post-Partum Haemorrhage — SDL Guide (Part 3)
Blood and Blood Product Transfusion in PPH
Severe PPH (blood loss >1000 mL with haemodynamic compromise) requires blood component therapy alongside haemostatic interventions. The goals of transfusion are to restore oxygen-carrying capacity, replace coagulation factors, and prevent the lethal triad of hypothermia, acidosis, and coagulopathy.
Packed Red Blood Cells (PRBCs) are transfused to maintain haemoglobin ≥8 g/dL in actively bleeding patients (some guidelines suggest ≥10 g/dL in the context of ongoing haemorrhage). One unit of PRBCs (approximately 250 mL) raises haemoglobin by approximately 1 g/dL in a non-bleeding adult.
Fresh Frozen Plasma (FFP) replaces clotting factors (I, II, V, VII, IX, X, XI, and von Willebrand factor) and is indicated when coagulation is compromised. Trigger: PT or APTT >1.5 times normal, or as part of a massive transfusion protocol. Usual dose: 10–15 mL/kg.
Platelet concentrate is transfused when platelet count falls below 50–75 × 10⁹/L in actively bleeding patients. In PPH-associated DIC, platelet counts fall because of consumption.
Cryoprecipitate is rich in fibrinogen (Factor I), Factor VIII, and von Willebrand factor. It is specifically indicated when fibrinogen falls below 2 g/dL — a critical threshold in PPH because fibrinogen is the first clotting factor to become critically depleted in massive haemorrhage. A fibrinogen level of 1 g/L in active PPH predicts progression to severe haemorrhage with high sensitivity. Each unit of cryoprecipitate contains approximately 200 mg fibrinogen.
Massive transfusion protocol (MTP) is activated when blood loss exceeds 1.5 litres or when clinical haemodynamic instability demands immediate unmatched product transfusion. The recommended ratio-based approach is PRBC:FFP:Platelets = 1:1:1 (empirical balanced transfusion), which mirrors the composition of whole blood and prevents the dilutional coagulopathy that develops when PRBCs are given without concurrent FFP and platelets. O-negative blood is issued in emergencies before group-specific blood is available.
DIC management requires simultaneous treatment of the trigger (evacuate the uterus, control bleeding, treat sepsis), replacement of consumed factors (FFP, cryoprecipitate, platelets), and correction of physiological derangements (tranexamic acid for fibrinolysis, warming for hypothermia, bicarbonate for severe acidosis if pH <7.1).
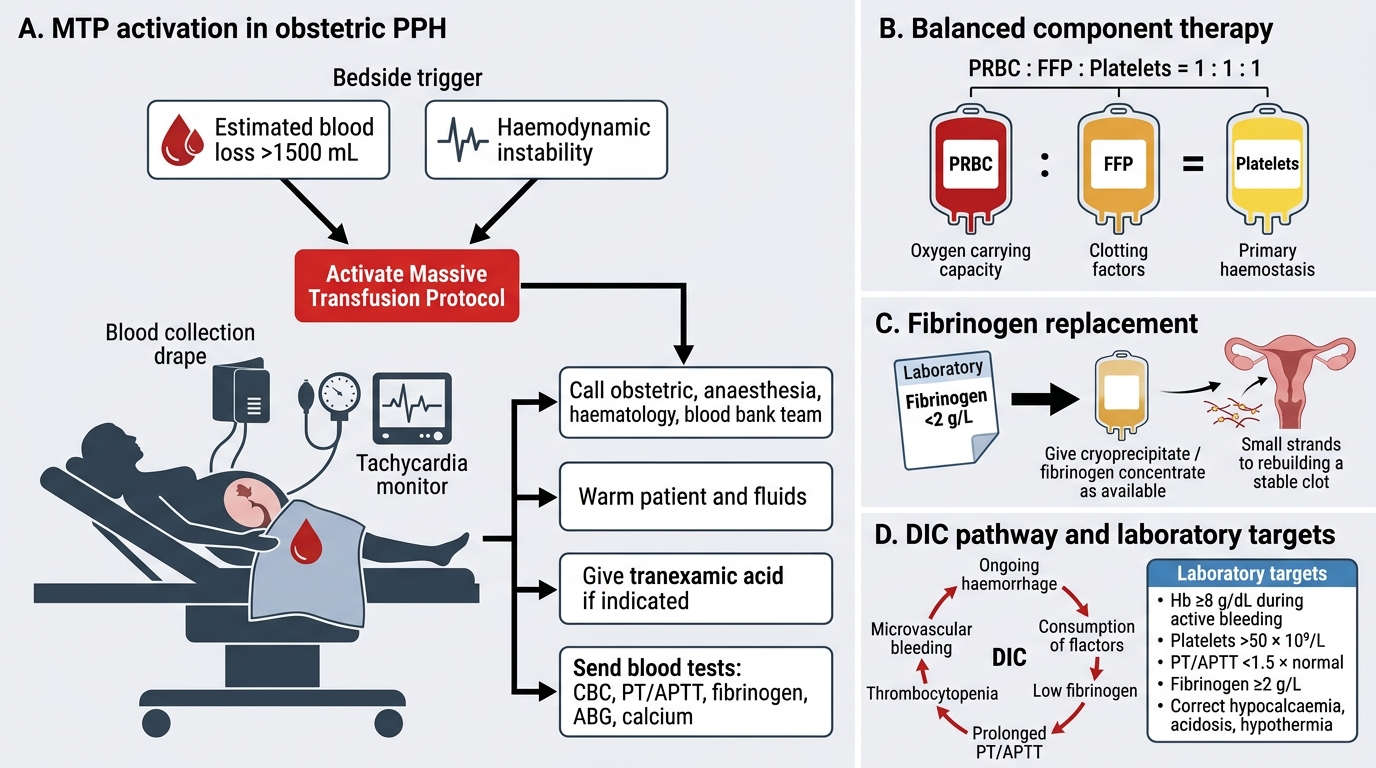
Massive Transfusion Protocol in Obstetric PPH
SELF-CHECK
In a patient with massive PPH and DIC, the fibrinogen level returns at 1.2 g/dL. Which blood product is most specifically indicated?
A. Packed red blood cells — to correct the anaemia
B. Fresh frozen plasma — contains all clotting factors including fibrinogen
C. Cryoprecipitate — concentrated fibrinogen, indicated when fibrinogen falls below 2 g/dL
D. Platelet concentrate — DIC consumes platelets, which is the priority to replace
Reveal Answer
Answer: C. Cryoprecipitate — concentrated fibrinogen, indicated when fibrinogen falls below 2 g/dL
A fibrinogen level of 1.2 g/dL is below the critical threshold of 2 g/dL. Cryoprecipitate is the most concentrated source of fibrinogen (each unit contains approximately 200 mg fibrinogen) and is specifically indicated for hypofibrinogenaemia in PPH-DIC. FFP contains some fibrinogen but in much lower concentration; very large volumes would be needed to raise fibrinogen adequately. PRBCs correct anaemia but do not replace coagulation factors. Platelets are also consumed in DIC but the specific deficit identified here is fibrinogen, and cryoprecipitate targets this most efficiently.
Self-Assessment
The following clinical scenario asks you to integrate everything covered in this module — definition and classification of PPH, the 4 T's causative framework, haemodynamic assessment using the shock index, the uterotonic ladder with its contraindications, and blood product thresholds. Work through each question before revealing the answer. The ability to rapidly synthesise these elements in a time-pressured clinical situation — correctly selecting a uterotonic based on the patient's comorbidities, calculating the shock index, and knowing when to trigger a massive transfusion protocol — is the core competency this module builds toward. If any answer surprises you, revisit the corresponding section before proceeding to clinical placements.
Case: Mrs. Kamala, 34 years old, G4P3, delivered a 4.2 kg male baby vaginally after a labour augmented with oxytocin. The placenta delivered completely. 20 minutes after delivery the midwife calls urgently: the uterine fundus is at the level of the umbilicus and soft on palpation; blood is draining freely through the vagina with clots. Estimated blood loss is 650 mL, heart rate 118/min, BP 94/64 mmHg.
Consider these questions:
1. What is the most likely cause of PPH in this patient, and what risk factors are present?
2. Calculate the shock index and interpret it.
3. What is the first uterotonic you would administer, at what dose, and by what route?
4. If the uterus remains atonic after two doses of oxytocin and the patient is not known to have asthma, which drug would you add next?
5. At what fibrinogen threshold would you administer cryoprecipitate?
Answers:
1. Uterine atony (soft, non-contracting uterus; complete placenta delivered) — risk factors: grand multiparity (G4P3), macrosomia (4.2 kg), oxytocin augmentation (downregulation of receptors).
2. Shock index = 118 ÷ 94 = 1.26 — haemodynamic compromise; requires immediate intervention (IV access, uterotonics, IV fluid resuscitation, prepare for blood transfusion).
3. Oxytocin 10 IU IM (or IV infusion 10–20 IU in 500 mL normal saline) — first-line uterotonic, administered immediately.
4. Carboprost 250 µg IM — second-line after oxytocin failure (ergometrine would also be an option in a normotensive patient, but carboprost is appropriate here; ergometrine is contraindicated if she were hypertensive).
5. Fibrinogen <2 g/dL (or 2 g/L) — administer cryoprecipitate.
SELF-CHECK
Which of the following is the single most common cause of primary postpartum haemorrhage?
A. Retained placenta (Tissue) — incomplete placental delivery in the third stage
B. Uterine atony (Tone) — failure of myometrial contraction after placental delivery
C. Genital tract lacerations (Trauma) — cervical and vaginal tears after instrumental delivery
D. Coagulopathy (Thrombin) — DIC triggered by placental abruption
Reveal Answer
Answer: B. Uterine atony (Tone) — failure of myometrial contraction after placental delivery
Uterine atony — failure of the myometrium to contract and retract after placental delivery — is responsible for 70–80% of all primary PPH cases. The other causes (retained placenta, genital tract trauma, and coagulopathy) each account for smaller proportions. Recognising atony as the dominant cause guides the priority intervention: uterotonic therapy (oxytocin first).
CLINICAL PEARL
The single most important intervention to prevent PPH is giving oxytocin 10 IU IM within 1 minute of delivery of the baby — this simple act, part of AMTSL, reduces PPH incidence by approximately 40%. When PPH occurs despite prevention, remember to reassess all four causes (4 T's) because atony and trauma can co-exist: treat the atonic uterus AND repair the laceration. A critical drug safety rule: ergometrine raises blood pressure and is absolutely contraindicated in hypertension and pre-eclampsia — giving it to a pre-eclamptic patient can precipitate a stroke. When in doubt about the diagnosis, the 'tissue test' (examine the delivered placenta and membranes for completeness) and a gentle exploration of the lower genital tract under good lighting are low-risk, high-yield diagnostic steps.