Page 15 of 22
OP1.5 | Amblyopia: Types, Prevention and Refractive Treatment — SDL Guide
Learning Objectives
- Define amblyopia and explain the role of the critical period in its development
- Enumerate and describe the four types of amblyopia with their mechanisms
- Identify the clinical features that distinguish amblyopia from organic visual loss
- Describe the prevention of amblyopia through early detection and optical correction
- Outline the treatment of refractive amblyopia: spectacle correction, occlusion therapy, and atropine penalisation
INSTRUCTIONS
Amblyopia is the most common cause of monocular visual impairment in children in developed and developing countries, affecting approximately 2–4% of the general population. It is unique in ophthalmology because the window of treatment is strictly time-limited: beyond the critical period, the visual cortex loses its plasticity and amblyopia becomes permanent. Early detection — through school vision screening, child welfare checks, and a reflex of testing VA in every child who presents to a clinic — is therefore a public health imperative. This module establishes the neurobiological basis for amblyopia and equips you to identify, diagnose, and initiate management for the most important preventable cause of lifelong monocular visual impairment.
References
- Khurana AK. Comprehensive Ophthalmology, 7th ed. New Age International, 2019. Ch 14, Amblyopia and Strabismus. (textbook)
- Parsons J, Duke-Elder S. Diseases of the Eye, 22nd ed. Elsevier, 2011. Ch 22, Amblyopia. (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Preethi is 8 years old and brought to school screening by her teacher, who noticed that she holds her textbook very close to her face. VA testing reveals: RE 6/6, LE 6/60. With a pinhole, LE VA remains 6/60 — no improvement. The school health nurse refers her urgently. At the paediatric ophthalmology clinic, cycloplegic refraction shows RE +1.00 D and LE +4.50 D. The left eye fundus is completely normal; the disc and macula are healthy. There is no cataract and no media opacity. The diagnosis is anisometropic amblyopia: the left eye has been functionally suppressed for years because of its higher, uncorrected refractive error. Preethi is 8. The question is: have we arrived too late?
WHY THIS MATTERS
Amblyopia affects 2–4% of the global population — making it the single most common cause of monocular visual loss in people under 40 years old. In India, population-based studies suggest similar prevalence, and uncorrected refractive errors contribute substantially. The tragedy of amblyopia is that it is preventable — if detected and treated during the critical period — yet many cases reach school age or adulthood untreated because the child had no symptoms (the other eye sees well and compensates) and no one tested VA. As a doctor — whether in a PHC, a paediatric clinic, or an adult OPD — you are in a position to detect amblyopia early by testing VA in every child, checking for anisometropia by cycloplegic refraction, examining the red reflex in neonates, and acting on asymmetric VA promptly. The treatment window is narrow and the consequences of missing it are lifelong.
RECALL
From OP1.1, recall: the primary visual cortex (V1, area 17) is organised in ocular dominance columns — alternating columns responding to input from each eye — established and refined during early postnatal development. From OP1.2, recall: anisometropia (significant refractive error difference between the two eyes) is a major risk factor for amblyopia because the brain receives a chronically defocused image from the more ametropic eye. From OP1.3, recall: VA testing in children requires cycloplegic refraction — a child's powerful accommodation can mask even large hypermetropic errors; amblyopia is diagnosed when VA does not improve to the expected level with the best optical correction, and no structural cause is found. These concepts now connect into the pathophysiology of amblyopia.
Clinical Presentation: How Amblyopia Comes to Clinical Attention
Amblyopia is, by definition, a silent disease from the child's perspective. The amblyopic eye does not hurt. It does not look abnormal. The child does not complain of double vision, because the brain suppresses the image from the affected eye rather than fusing it. The only objective sign — reduced visual acuity in one eye — is invisible unless someone specifically measures it. This is why amblyopia is so frequently missed until school age or later: the child functions normally using the good eye, and neither the parents nor the child can identify which eye is seeing poorly.
The presentations that bring amblyopic children to medical attention follow one of four patterns. First, a routine school vision screening or child welfare check detects an inter-eye VA asymmetry on Snellen testing — the child passes with 6/6 in the right eye and fails with 6/36 in the left. Second, a parent notices the child squinting or tilting their head, or covering one eye repeatedly — which may indicate strabismus as the underlying cause, or may be the child's own compensatory strategy. Third, the child is brought for evaluation of a visible squint, and VA testing during that assessment reveals reduced acuity in the deviated eye. Fourth, a neonatal or infant check reveals an absent red reflex, leukocoria, or a dense congenital cataract — all of which trigger referral before amblyopia has even developed, precisely to prevent it. In each of these pathways, the physician's alertness to the possibility of amblyopia — and the reflex of testing VA in each eye separately whenever any child presents with an eye complaint — is the difference between early detection and a missed diagnosis that closes the treatment window permanently.
Pathophysiology: Critical Period, Visual Cortical Plasticity and Amblyogenesis
Amblyopia is defined as a unilateral (or, rarely, bilateral) reduction in best-corrected visual acuity that is not explained by any structural abnormality of the eye or visual pathway, and that is caused by abnormal visual experience during the critical period of visual development. It is a disorder of cortical development, not of the eye itself — the eye is structurally normal, but the visual cortical circuits representing it are underdeveloped.
The critical period is the window of heightened neural plasticity during which the visual cortex requires appropriate visual input to develop normal spatial vision. In humans, this period extends from birth to approximately 7–8 years, with the greatest plasticity in the first 2–3 years of life. The key concept is: if one eye consistently receives a degraded, defocused, or suppressed image during this period, the cortical representation of that eye fails to develop normally. This is not a reversible refractive problem — it is a permanent rearrangement of cortical connectivity.
The neurobiological mechanism, elucidated in Hubel and Wiesel's Nobel Prize-winning experiments (monocular deprivation in kittens), involves competitive synaptic plasticity. The inputs from the two eyes compete for synaptic territory in V1 ocular dominance columns. When one eye's input is consistently weaker (suppressed, defocused, or physically occluded), the dominant eye's cortical representation expands at the expense of the weaker eye. Ocular dominance shift — the cortex becomes dominated by the fellow eye — is the cortical substrate of amblyopia.
The three conditions that can cause this abnormal experience during the critical period are:
1. A constant misalignment (strabismus) causing suppression of the deviated eye's image
2. Defocus from a significant refractive error in one or both eyes (anisometropia, or bilateral high ametropia)
3. Deprivation — a physical obstacle (cataract, ptosis, corneal opacity) blocking formed visual input entirely
After the critical period closes, the cortex loses its plasticity and the amblyopia becomes permanent — which is why early detection and treatment are so urgently time-constrained.
Types of Amblyopia: Strabismic, Anisometropic, Deprivation and Ametropic
Understanding the type of amblyopia guides the treatment strategy. The four types differ in mechanism, laterality, severity, and urgency of intervention.
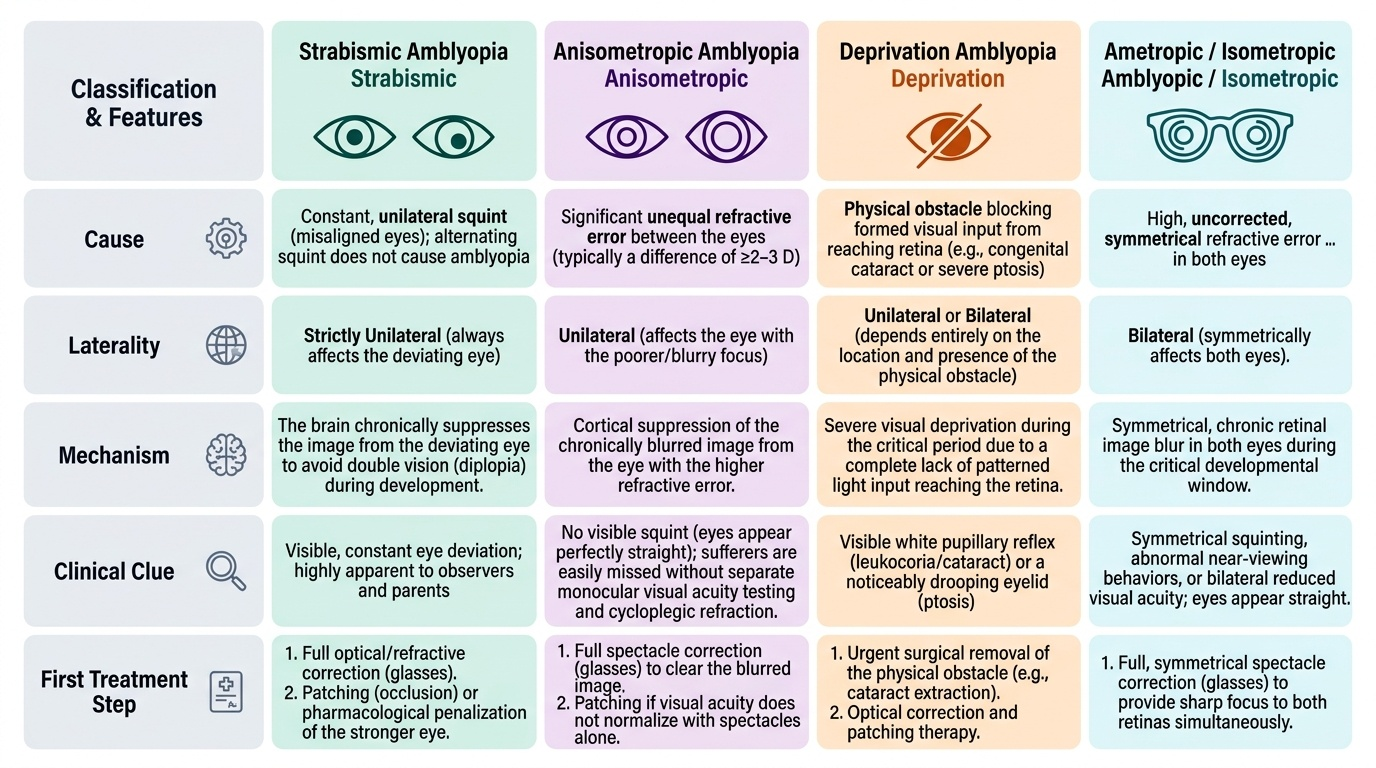
Provided image
1. Strabismic amblyopia is the most common form in clinical series (in high-income countries where refractive error is routinely corrected). It occurs when a constant (not intermittent) squint causes the brain to chronically suppress the image from the deviating eye to avoid diplopia (double vision). The suppression, sustained over years of the critical period, produces amblyopia in the deviated eye. Importantly: alternating squint (the patient alternates fixation between the two eyes) does NOT cause amblyopia — because each eye is used approximately equally. Only a constant unilateral squint causes strabismic amblyopia.
2. Anisometropic amblyopia occurs when a significant difference in refractive error between the two eyes (typically ≥2–3 D for spherical anisometropia) causes one eye to be chronically out of focus even when the other eye sees clearly through its natural/residual accommodation. The blurred eye is suppressed cortically over time. Crucially, anisometropic amblyopia may have no visible squint — the patient appears to have straight eyes — and may not be detected unless VA is tested in each eye separately AND cycloplegic refraction is performed. It is a common cause of missed amblyopia at school screening.
3. Deprivation amblyopia is the most severe form. It occurs when a physical obstacle prevents formed visual input from reaching the retina of one (or both) eye(s) during the critical period. Causes: congenital cataract, unilateral complete ptosis (covering the visual axis), corneal opacity, or a vitreous haemorrhage. Bilateral congenital cataracts causing visual deprivation from birth represent an ophthalmic emergency — surgery must be performed within weeks (ideally within the first 6–8 weeks of life) to prevent irreversible bilateral deprivation amblyopia. Unilateral congenital cataract requires surgery even earlier and intensive patching of the fellow eye afterwards, as the asymmetry strongly favours the fellow eye's cortical dominance.
4. Ametropic (isometropic) amblyopia refers to bilateral amblyopia from bilateral high uncorrected refractive error — most commonly bilateral high hypermetropia (>+5 D) or bilateral significant astigmatism. Both eyes receive a blurred image; neither eye gains cortical dominance over the other. The result is bilateral reduced VA, which may be less severe than unilateral amblyopia but can still be significant. Treatment is bilateral optical correction.
SELF-CHECK
A 5-year-old girl has VA of 6/6 in the right eye and 6/36 in the left eye. Cycloplegic refraction: RE +1.50 D, LE +5.00 D. The left eye does not improve with pinhole. Fundoscopy and anterior segment are normal bilaterally. There is no strabismus. What is the diagnosis?
A. Strabismic amblyopia
B. Anisometropic amblyopia
C. Deprivation amblyopia
D. Left optic nerve disease
Reveal Answer
Answer: B. Anisometropic amblyopia
This is anisometropic amblyopia. The key features are: significant anisometropia (LE +5.00 D vs RE +1.50 D = 3.50 D difference), reduced VA in the more ametropic eye, no improvement with pinhole (the VA loss is cortical, not refractive), no strabismus, and a structurally normal eye (no organic cause). The chronically defocused left eye has been suppressed cortically during the critical period. There is no structural cause, ruling out optic nerve disease. Strabismic amblyopia requires a constant squint. Deprivation amblyopia requires a media opacity or ptosis.