Page 6 of 22
OP1.2 | Refractive Errors: Classification and Correction — SDL Guide (Part 2)
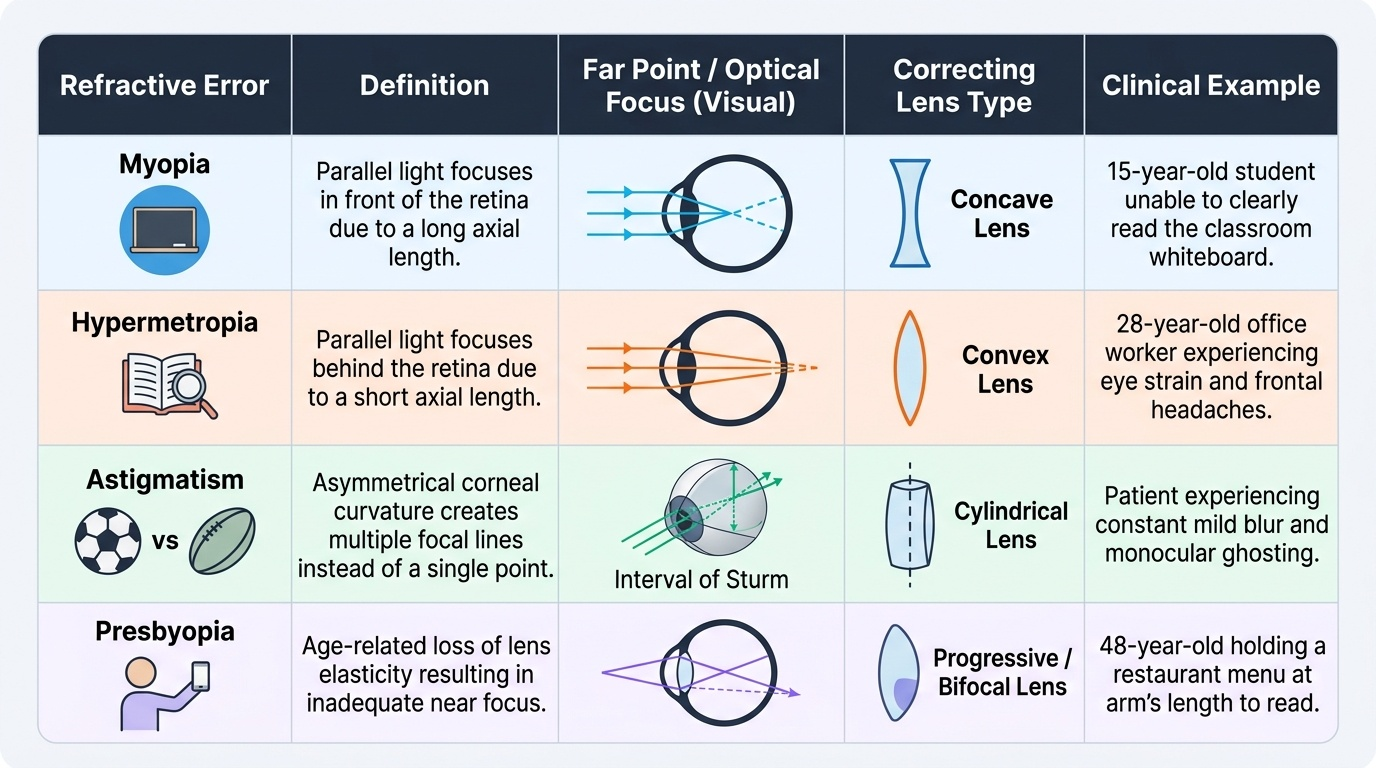
Astigmatism and Presbyopia
Astigmatism is the refractive condition in which the refracting power of the eye differs in different meridians — the eye cannot form a point focus; instead, parallel light is focused as two separate line foci separated by the interval of Sturm. The most common cause is an asymmetrically curved cornea (the cornea is steeper in one meridian than the perpendicular meridian, like a rugby ball rather than a football), though the crystalline lens also contributes (lenticular astigmatism). Unlike myopia and hypermetropia, which produce uniform blur at a given distance, astigmatism causes blurring and distortion at both distance and near simultaneously, because no single plane can bring both meridians to focus at the same point on the retina. Patients may describe monocular ghosting, shadow images around letters, or difficulty reading fine print even with distance spectacles. Astigmatism is extremely common and frequently coexists with myopia or hypermetropia. The clinical significance depends on its degree and type — a small regular astigmatism is easily corrected with a cylindrical spectacle lens, while irregular astigmatism (from corneal scarring or keratoconus) cannot be corrected with standard spectacle lenses and requires rigid contact lenses or surgery.
Provided image
Regular astigmatism (most common, correctable with cylindrical lenses): the two principal meridians (steepest and flattest) are perpendicular to each other.
- With-the-rule (WTR) astigmatism: the vertical meridian is steeper than the horizontal — corrected with a minus cylinder at 180° (or equivalently, a plus cylinder at 90°). This is more common in young individuals.
- Against-the-rule (ATR) astigmatism: the horizontal meridian is steeper — corrected with a minus cylinder at 90°. More common with advancing age.
- Oblique astigmatism: principal meridians lie at oblique angles (not at 90° or 180°).
Irregular astigmatism: no consistent difference between meridians; caused by corneal scarring, keratoconus (progressive corneal ectasia causing cone-shaped protrusion, corrected with rigid contact lenses), or trauma. Cannot be corrected fully with spectacles — requires rigid gas-permeable contact lenses or surgery.
Presbyopia is the age-related, physiological loss of the amplitude of accommodation, typically becoming symptomatic around age 40 years. It is NOT a disease but an inevitable physiological change. The mechanism is primarily loss of elasticity of the crystalline lens (the lens nucleus becomes progressively sclerotic and rigid), though changes in the ciliary muscle and zonules also contribute. The lens can no longer deform adequately for near vision despite full ciliary muscle contraction.
Clinically: the patient (typically over 40) holds reading material at arm's length, requires brighter light for reading, and experiences difficulty in dim light. Near vision is progressively blurred while distance vision remains (in an otherwise emmetropic person) clear.
The required near addition (reading add) progresses with age: approximately +1.00 D at age 40, increasing to approximately +2.50–3.00 D by age 60. Correction options include: reading spectacles (plus lenses), bifocals (two optical zones — distance on top, near at bottom), trifocals, and progressive (varifocal) lenses.
SELF-CHECK
A 48-year-old school teacher with previously normal distance vision presents with gradual difficulty in reading and near work over the past 5 years. She needs to hold her phone at arm's length to read. Her distance VA is 6/6. What is the PRIMARY mechanism of her condition?
A. Increased axial length of the eyeball
B. Loss of elasticity of the crystalline lens
C. Weakness of the ciliary muscle
D. Corneal flattening reducing refracting power
Reveal Answer
Answer: B. Loss of elasticity of the crystalline lens
Presbyopia is caused primarily by progressive hardening (sclerosis) of the crystalline lens, which loses its elasticity and cannot deform (become more convex) adequately during ciliary muscle contraction. This reduces the amplitude of accommodation. While changes in the ciliary muscle and zonules also contribute, lens hardening is the primary and most well-established mechanism. Increased axial length causes myopia; ciliary muscle weakness alone is not the dominant mechanism in presbyopia; corneal flattening is not the cause.
Correcting Refractive Errors: Spectacles, Contact Lenses and Optical Principles
Determining the type and degree of a refractive error — refraction — is the central examination skill in clinical optics. The goal of refraction is to identify the precise lens power that, when placed in front of the eye, brings the patient's vision to its best corrected level. This process has both objective components (which do not require patient cooperation or verbal responses) and subjective components (which depend on patient feedback). In clinical practice these two approaches are almost always combined: objective refraction establishes a starting point, and subjective refraction refines it to a prescription. Understanding both methods is essential because neither alone is sufficient — an objective measurement without subjective refinement may leave the patient slightly over- or under-corrected, while subjective refraction without an objective starting point is time-consuming and prone to error in children or patients who cannot cooperate. Two main approaches are used:
Objective refraction (does not require patient responses):
- Retinoscopy (skiascopy): the classic, examiner-performed objective method. A streak of light is projected into the eye and the movement of the reflex in the pupil — 'with' or 'against' the motion of the retinoscope — guides the addition of trial lenses until the neutral point (working distance corrected) is reached. Essential for children, uncooperative patients, and pre-verbal infants.
- Auto-refractometry: automated, computerised objective refraction. Fast but requires patient cooperation and can overestimate myopia in young patients due to accommodative fluctuation (must be followed by subjective refinement).
- Cycloplegic refraction: the use of cycloplegic drops (cyclopentolate 1%, or atropine 1% for children under 5) before refraction to paralyse accommodation and reveal the true total refractive state — essential in children (to detect latent hypermetropia) and in strabismus assessment.
Subjective refraction: trial-frame refraction or a phoropter, using patient responses to 'better or worse' comparisons. The gold standard for adult prescription.
Optical correction principles:
- Myopia: minus (concave) spherical lens — diverges incoming light so the focal point moves posteriorly to the retina
- Hypermetropia: plus (convex) spherical lens — converges light so the focal point moves anteriorly to the retina
- Astigmatism: cylindrical lens (axis must be aligned with the flat meridian for minus cylinder convention)
- Presbyopia: plus add lens — bifocal, trifocal, or progressive
Contact lenses: available in soft (hydrogel / silicone-hydrogel) and rigid gas-permeable (RGP) designs. RGP lenses neutralise irregular corneal astigmatism by creating a smooth tear-film interface. Contact lens wearers have an elevated risk of Acanthamoeba keratitis (ring infiltrate, severe pain disproportionate to signs) and bacterial keratitis — hygiene counselling is essential.
Myopia control (paediatric): strategies to slow progressive myopia include low-dose atropine 0.01% eye drops (ATOM2 trial, Singapore — slows progression with minimal side effects), orthokeratology (overnight rigid contact lenses that reshape the cornea temporarily), and increased outdoor time (proven protective in epidemiological studies).
Differential Diagnosis and When to Investigate Further
Not all visual blurring is due to refractive error, and the clinician must always ask: 'Does this improve with a pinhole?' If it does NOT, an organic cause must be sought. This distinction is the single most important clinical decision in the assessment of a patient with blurred vision: patients with a purely refractive cause improve substantially with the pinhole (which restricts light to the central optical axis and bypasses peripheral aberration), whereas patients with retinal, optic nerve, or corneal structural disease do not improve — the substrate for a sharp image is damaged regardless of the optical correction provided. Making this call correctly determines whether a patient goes home with a spectacle prescription or is urgently referred for fundoscopy, visual field testing, or neuroimaging. The following red-flag features — each of which mandates ophthalmological assessment beyond simple refraction — must be actively screened for in every patient presenting with visual blurring:
- Recent onset (days to weeks) of visual deterioration in a previously corrected patient — suggests a new organic problem (vitreous haemorrhage, retinal detachment, optic neuritis, wet AMD)
- Associated symptoms: pain, photophobia, floaters, flashes, field loss — all point away from simple refractive error
- Asymmetric refractive error (anisometropia) in a child — significant anisometropia (>2–3 D difference between the two eyes) is a major risk factor for amblyopia and must prompt urgent treatment (see OP1.5)
- Progressive myopia in adults (>25 years) — pathological myopia or nuclear cataract (index myopia) should be considered
- High hypermetropia in children — risk of accommodative esotropia and amblyopia; cycloplegic refraction and occlusion therapy may be required
Organic causes that mimic refractive blur: posterior subcapsular cataract (causes disproportionate glare and near blur), macular disease (metamorphopsia, central scotoma — an Amsler grid test is useful), optic nerve disease (colour desaturation, afferent pupil defect), corneal disease (irregular astigmatism from keratoconus or scarring).