Page 12 of 22
OP1.4 | Refractive Surgery: Principles and Indications — SDL Guide
Learning Objectives
- Explain the optical principle by which corneal laser surgery corrects refractive errors
- Describe the procedure and indications for LASIK, PRK and SMILE
- Describe the rationale and indications for phakic IOL and refractive lens exchange (RLE)
- Enumerate the pre-operative assessment criteria and absolute contraindications for refractive surgery
- Identify the common complications of laser refractive surgery and their management principles
INSTRUCTIONS
Refractive surgery has transformed the management of myopia, hypermetropia, and astigmatism, offering millions of patients spectacle-independence. As a physician, you will routinely encounter patients who have undergone or are considering refractive surgery — and who ask questions about risks, suitability, and outcomes. Understanding the principles and indications helps you counsel patients, identify unsuitable candidates (preventing the catastrophic complication of post-LASIK ectasia), and co-manage post-surgical patients appropriately.
References
- Khurana AK. Comprehensive Ophthalmology, 7th ed. New Age International, 2019. Ch 4, Refractive Surgery. (textbook)
- Parsons J, Duke-Elder S. Diseases of the Eye, 22nd ed. Elsevier, 2011. Ch 6, Surgical Correction of Refractive Errors. (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Capt. Arjun Singh, a 26-year-old trainee commercial pilot, has a refraction of −5.00 D in both eyes and has worn contact lenses since age 16. He is informed by the aviation medical board that he cannot wear soft contact lenses during flight operations due to hypoxia risk at altitude, and that spectacles are not permitted in the cockpit of his aircraft type. He asks his ophthalmologist: 'Can I have laser surgery so I can fly without glasses or contacts?' His ophthalmologist orders a detailed corneal topography, pachymetry (corneal thickness measurement), and a cycloplegic refraction — and only after reviewing these will she decide whether Captain Singh is a surgical candidate. What is she looking for, and what procedure would she recommend?
WHY THIS MATTERS
Refractive surgery is now one of the most commonly performed elective surgical procedures globally. With over 40 million LASIK procedures performed since its FDA approval in 1999, it has an extraordinary safety record when patients are selected appropriately. However, the consequences of operating on an unsuitable candidate — particularly a patient with subclinical keratoconus — can be devastating: progressive post-operative ectasia (corneal bulging and thinning) leading to severe, uncorrectable visual loss. As a doctor, you are the first counsellor: understanding the principles, indications, and contraindications allows you to screen patients appropriately and provide evidence-based counselling. You will also encounter patients with post-LASIK complications who present to general clinics — knowing the surgical history is essential for their subsequent ophthalmic management (for example, post-LASIK patients have altered corneal thickness and curvature, affecting IOP measurement and cataract surgical calculations).
RECALL
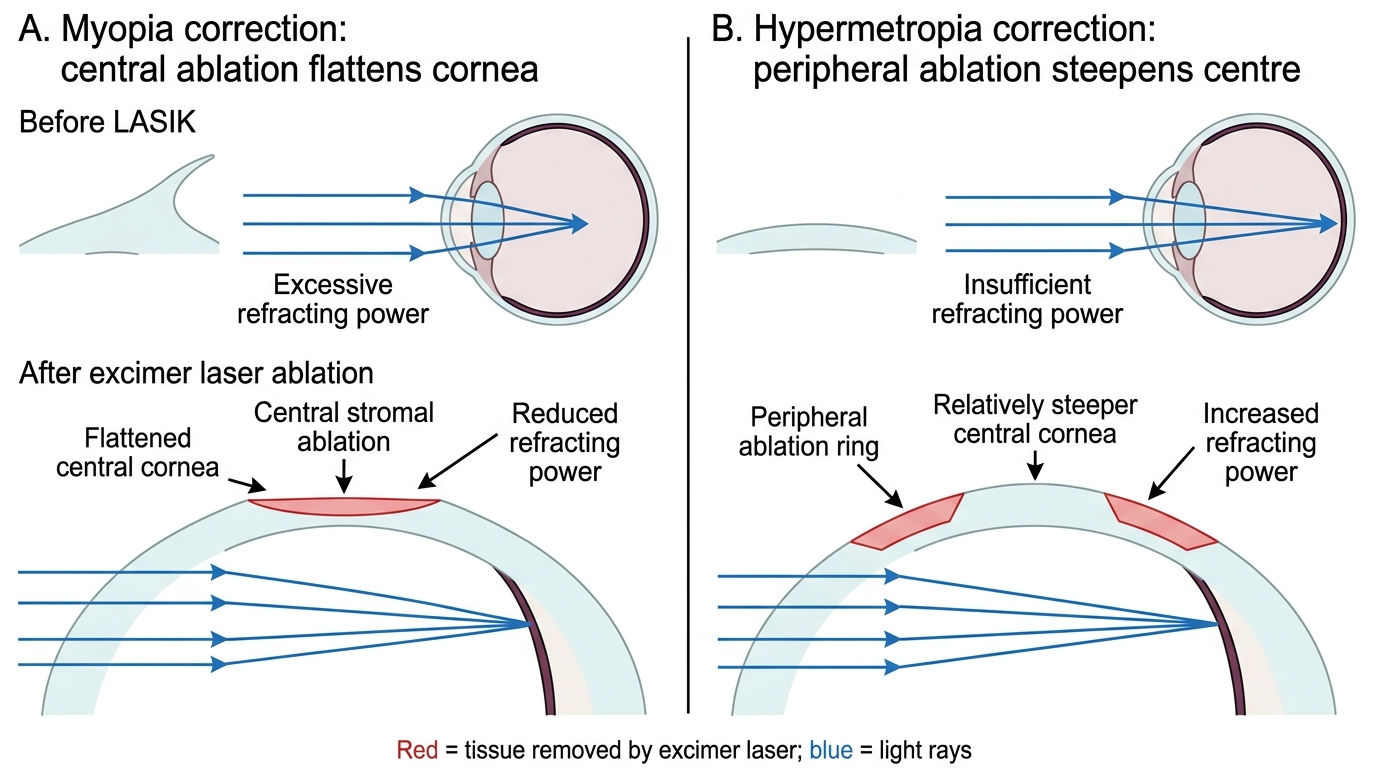
From OP1.1, recall: the cornea contributes approximately 43 D of the total ~60 D refracting power. Changing corneal curvature changes refracting power — steeper cornea = greater plus power, flatter cornea = less plus power. From OP1.2: myopia (excess power, focal point anterior to retina) is corrected by reducing refracting power — i.e. flattening the cornea. Hypermetropia (insufficient power) is corrected by increasing refracting power — steepening the cornea. Astigmatism (unequal meridional power) is corrected by selectively reshaping to equalise meridians. These physical principles are the basis of all corneal refractive surgery.
Clinical Indication and Relevance: Who Seeks Refractive Surgery and Why
Refractive surgery presents to the clinician in two ways: as a planned elective procedure sought by a patient who wishes to be free of spectacles or contact lenses, and as a past surgical history that now complicates subsequent ophthalmic management. Both presentations require the physician to understand the principles, indications, and potential consequences of the surgery.
The patient seeking refractive surgery is almost always motivated by a desire to reduce dependence on optical correction — a quality-of-life goal that is entirely legitimate and, in well-selected patients, reliably achieved. Common presenting stories include the young professional who finds spectacles impractical in an active occupation or sport; the contact lens wearer with recurrent lens-related infections or discomfort who wants a permanent solution; the military or aviation candidate whose service requires unaided visual acuity that they currently cannot meet; and the patient with high myopia whose thick spectacle lenses produce magnification and cosmetic distortion that contact lenses alone do not fully resolve.
The physician's role in this initial encounter is not to perform the surgery — but to counsel accurately about candidacy, to understand the pre-operative workup that distinguishes suitable from unsuitable patients, and to recognise the absolute contraindications that must be screened before any surgical evaluation. The single most important of these — and the one responsible for the most devastating surgical outcomes — is the presence of keratoconus or subclinical keratoconus, a corneal ectatic disease that is invisible to clinical inspection but detectable on corneal topography and tomography. Knowing this — and knowing that any physician who refers a patient for refractive surgery should enquire about topographic screening — is the clinical knowledge this module is designed to provide.
The Optical Principle: How Laser Surgery Reshapes the Cornea
All corneal refractive procedures exploit a single unifying principle: modifying the anterior curvature of the cornea to adjust its refracting power, thereby changing the focal point of the eye. This is possible because the cornea is responsible for approximately 43 D of the eye's total ~60 D refracting power — even a small geometric change in corneal curvature produces a clinically significant refractive change.
The key instrument in laser corneal surgery is the excimer laser (argon fluoride, wavelength 193 nm — ultraviolet). The 193 nm wavelength is precisely absorbed by the peptide bonds of corneal stromal collagen without generating heat — this is photoablation (also called 'cold' laser ablation). Each laser pulse removes approximately 0.25 micrometres of corneal tissue. A computer-controlled scanning laser ablates tissue in a spatially controlled pattern to reshape the corneal surface:
- To correct myopia: tissue is removed centrally (central ablation), flattening the corneal curvature and reducing the central refracting power. The ablation zone is larger centrally than peripherally.
- To correct hypermetropia: tissue is removed in a ring pattern peripherally (annular ablation), causing relative steepening of the central cornea and increasing central refracting power.
- To correct astigmatism: a cylindrical ablation pattern selectively removes tissue in the steeper meridian to equalise the two principal meridians.
The total depth of ablation is proportional to the degree of refractive error — higher corrections require deeper ablation and therefore more corneal tissue removal. This is why a minimum residual stromal bed (RSB) of ≥250 micrometres must be maintained after ablation to prevent post-operative corneal ectasia (biomechanical failure leading to progressive corneal bulging).
Excimer Laser Corneal Reshaping in Myopia and Hypermetropia
SELF-CHECK
In LASIK for the correction of myopia, tissue is removed from which part of the cornea, and what is the refractive effect?
A. Tissue is removed peripherally, steepening the cornea and increasing refracting power
B. Tissue is removed centrally, flattening the cornea and decreasing refracting power
C. Tissue is removed from the lens, reducing the total refracting power of the eye
D. Tissue is removed peripherally, flattening the cornea and decreasing refracting power
Reveal Answer
Answer: B. Tissue is removed centrally, flattening the cornea and decreasing refracting power
In myopia, the eye has excess refracting power (focal point anterior to retina). LASIK for myopia corrects this by FLATTENING the central cornea — excimer laser ablation removes tissue from the central corneal stroma, reducing the central curvature and therefore the central refracting power, moving the focal point back to the retina. Peripheral ablation steepens the centre relatively (used for hypermetropia). LASIK does not involve the lens.
Corneal Laser Procedures: LASIK, PRK and SMILE
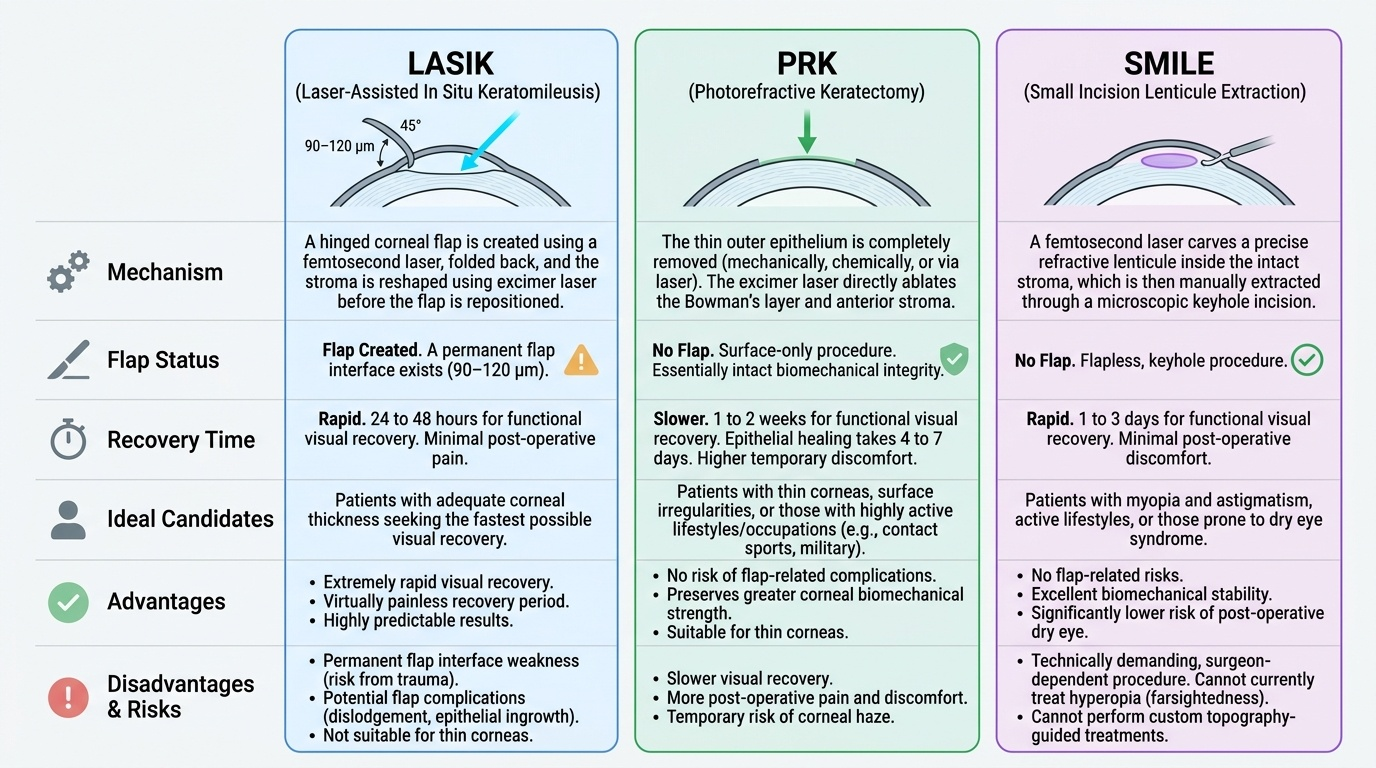
Three corneal laser procedures dominate current refractive surgery practice. They differ primarily in how the corneal surface is managed before excimer laser ablation — each choice represents a trade-off between visual recovery speed, biomechanical impact, and complication profile.
Provided image
LASIK (Laser-Assisted In Situ Keratomileusis) is the most widely performed refractive procedure worldwide. A thin hinged corneal flap (90–120 µm thick) is first created using either a microkeratome (mechanical oscillating blade) or, more commonly in modern practice, a femtosecond laser (which creates a more precise, predictable flap with lower flap complication rates). The flap is folded back, the excimer laser ablates the stromal bed beneath, and the flap is repositioned (it adheres by suction — no sutures required). Advantages: rapid visual recovery (24–48 hours), minimal pain, excellent predictability. Disadvantages: flap complications (dislodgement, striae, epithelial ingrowth), flap interface is a permanent weakness — contact sports or trauma risk, thin corneas may not have sufficient stroma for a safe RSB.
PRK (Photorefractive Keratectomy) predates LASIK and involves surface ablation — the epithelium is removed mechanically (a 'hockey stick' instrument), chemically (20% ethanol), or by laser (transepithelial PRK, TransPRK) before excimer laser ablation of Bowman's layer and anterior stroma. There is no flap; the epithelium regenerates over 4–7 days. Advantages: no flap risk, greater biomechanical strength retained (RSB threshold is met more easily because no flap depth is subtracted), suitable for patients with thinner corneas, active occupations/contact sports. Disadvantages: slower visual recovery (1–2 weeks), more post-operative pain (nerve endings exposed), slightly higher haze risk (mitigated by intraoperative mitomycin C 0.02%).
SMILE (Small Incision Lenticule Extraction) uses a single femtosecond laser to create an intrastromal lenticule (a disc of corneal stroma of the appropriate refractive shape) and a small 2–4 mm access incision. The surgeon manually dissects and removes the lenticule through the small incision — no flap, no excimer laser. Advantages: flapless (greater biomechanical integrity), minimal surface disruption, less dry eye (fewer corneal nerves cut), no excimer laser. Disadvantages: technically more demanding, less versatile (approved for myopia and myopic astigmatism; limited data for hypermetropia), cannot easily re-treat if under-correction occurs.