Page 10 of 22
OP1.3 | Visual Acuity, Colour Vision, Pinhole, Menace and Blink Reflex Testing — SDL Guide (Part 2)
Procedure: Pinhole Test, Colour Vision and Reflex Testing
Pinhole Test — procedure:
After measuring unaided VA, hold the pinhole disc in front of the patient's eye (the other eye is occluded) and ask them to repeat the VA reading. The pinhole should be aligned with the visual axis (the patient holds it, or it is on a trial frame). If the patient cannot read through the pinhole (too dark, too uncomfortable), the examiner can try multiple pinhole positions until the patient finds the clearest reading. Document VA with pinhole as, e.g., 'RE VA 6/36 NC, 6/9 with PH (pinhole)'. If VA with pinhole is better than VA without, the improvement is likely due to refractive error — a refraction is indicated. If no improvement occurs, organic pathology of the retina, optic nerve, or media (dense cataract may not improve) should be suspected.
Colour Vision (Ishihara plates) — procedure:
- Test in good, natural (preferably daylight or colour-corrected) illumination — avoid fluorescent light alone, which may distort colour perception.
- Hold each plate at approximately 35 cm from the patient's eyes; allow no more than 3 seconds per plate (longer viewing allows patients with colour deficiency to use pattern recognition strategies).
- Ask the patient to identify the number (or path, for the tracing plates used in patients who cannot read numbers).
- Record the number of plates read correctly out of the total presented (typically 17 diagnostic plates from the standard 38-plate set).
- Interpretation: a normal subject reads 17/17 (or near-perfect). A patient with red-green deficiency reads significantly fewer — typically <13/17 on the standard scoring. The specific error pattern can distinguish protanopia (red blindness), deuteranopia (green blindness), and the anomalous forms (protanomaly, deuteranomaly).
Menace Reflex (Threat Reflex) — procedure:
The menace reflex tests the visual and motor integrity of the reflex arc: the examiner makes a rapid threatening gesture (advancing the hand or an object toward one eye), and a normal subject blinks reflexively. Afferent limb: CN II (optic nerve — the threat must be visually perceived). Efferent limb: CN VII (facial nerve — orbicularis oculi contraction, lid closure). To test one eye: cover the fellow eye and make the threatening gesture. Caution: ensure the gesture does not generate a corneal air-current (which would independently trigger the blink via the corneal/CN V reflex). Important normal variant: the menace reflex is absent in infants under approximately 3 months because the afferent visual pathway is not yet fully myelinated. Its absence in a 1-month-old is normal; its absence in a 6-month-old is not.
Blink Reflex (Corneal Reflex) — procedure:
The blink reflex (corneal reflex) tests corneal sensation and facial nerve motor function. The examiner approaches a wisp of cotton wool from the side (outside the patient's vision, to avoid triggering the menace reflex) and gently touches the cornea — not the conjunctiva, but the corneal epithelium. Normal response: bilateral blink (both eyes blink — the direct response ipsilaterally, and the consensual response contralaterally, because the efferent CN VII signals both orbicularis muscles). Afferent limb: CN V1 (ophthalmic division, nasociliary branch). Efferent limb: CN VII bilaterally. Absent corneal reflex on one side: consider CN V1 lesion (loss of afferent → neither direct nor consensual response on stimulation of that eye) vs CN VII lesion (loss of efferent → the direct response is absent, but the consensual response when stimulating the SAME eye remains — a subtle but important distinction).
SELF-CHECK
A patient's unaided distance VA is 6/36 in the right eye. After placing a pinhole in front of the right eye, VA improves to 6/9. Which of the following conclusions is MOST appropriate?
A. The patient has optic nerve disease causing the reduced VA
B. The patient has macular degeneration
C. The reduced VA is likely due to a refractive error and can be improved with appropriate spectacles
D. The patient has a corneal scar that is reducing VA
Reveal Answer
Answer: C. The reduced VA is likely due to a refractive error and can be improved with appropriate spectacles
Improvement in VA with the pinhole strongly suggests that the cause of reduced VA is a refractive error. The pinhole eliminates peripheral aberrant rays and allows only the central beam to reach the retina, effectively reducing the blur from uncorrected myopia, hypermetropia, or astigmatism. Optic nerve disease and macular degeneration affect the neural substrate and do not improve with the pinhole. A dense corneal scar scatters light and usually does NOT improve with pinhole (though mild/peripheral scars may show some improvement). This patient should have a formal refraction to determine the prescription.
Interpreting the Results: VA Notation, Pinhole Effect and Colour Defects
Systematic interpretation of visual acuity test results requires a consistent documentation framework and an understanding of what each level of VA implies clinically. The VA number is not merely a number — it carries specific implications for the patient's functional capacity, their eligibility for certain occupations and activities, their qualification for government blindness certification and surgical intervention under the NPCBVI, and the urgency of further investigation. A physician who can look at a VA result and immediately translate it into a clinical decision — whether to prescribe, refer, investigate, or reassure — is doing exactly what this skill training is designed to produce. The same interpretive discipline applies to the pinhole result (does it improve or not?), the colour vision test (how many plates correct, and does the pattern suggest congenital vs acquired defect?), and the reflex tests (is the afferent or efferent limb affected?). Interpretation, not just measurement, is the clinical skill. The following principles and documentation framework guide this interpretation:
Provided image
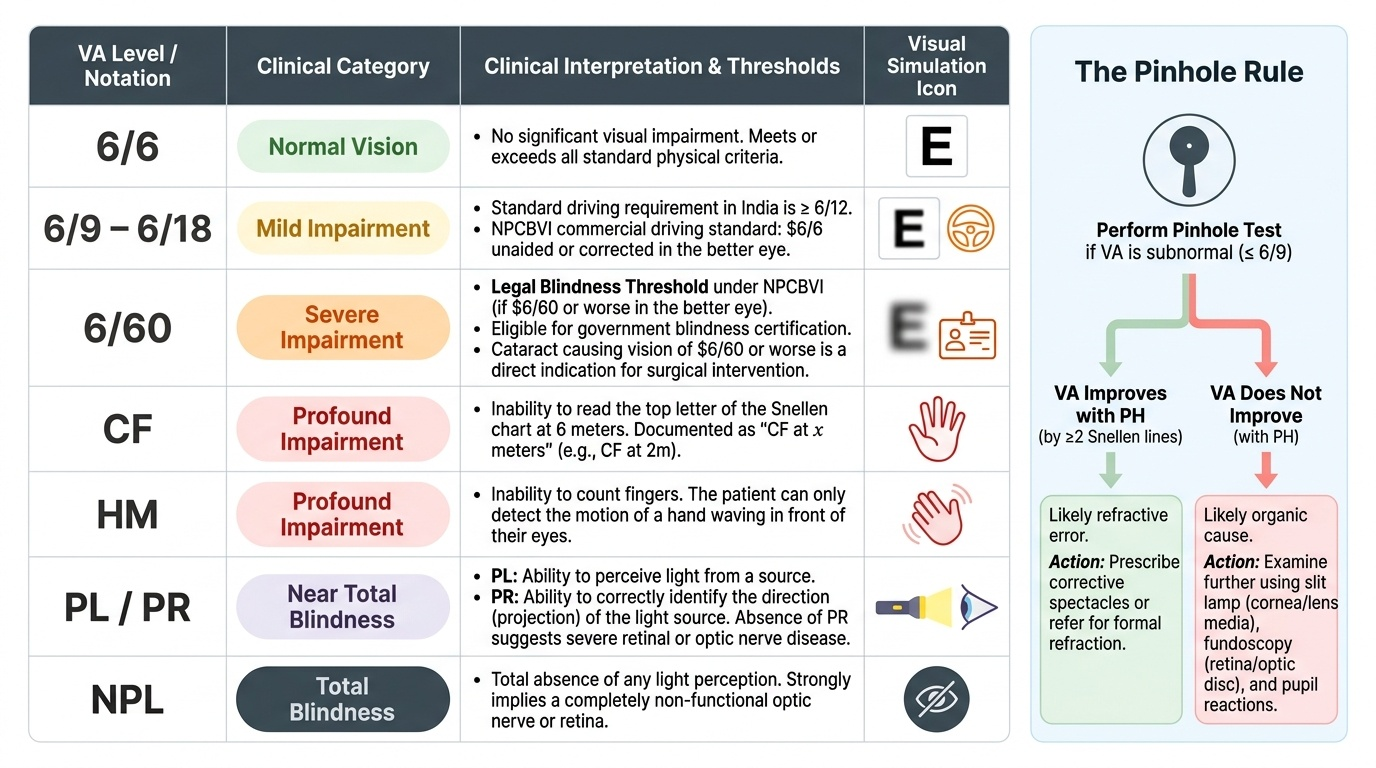
VA documentation hierarchy (from best to worst):
Key interpretation principles:
- VA 6/6: normal; no significant visual impairment.
- VA 6/9–6/18: mild impairment; driving standard requires ≥6/12 in India (NPCBVI for commercial vehicle: 6/6 unaided or corrected in better eye).
- VA 6/60 in the better eye: legal blindness threshold under the NPCBVI — eligible for blindness certification. Cataract causing 6/60 or worse is an indication for surgical intervention under NPCBVI.
- VA <6/60: document as CF at x metres, HM, PL (with projection = PR), or NPL. 'NPL' indicates total absence of light perception and suggests the optic nerve or retina is non-functional.
The pinhole interpretation rule:
- VA improves with PH (≥2 lines Snellen improvement): likely refractive cause → prescribe spectacles or refer for formal refraction.
- VA does not improve with PH: likely organic cause — examine further (slit lamp for corneal/lens media, fundoscopy for retina/disc, pupil reactions for optic nerve).
- Special case: dense cataract may reduce VA but not show pinhole improvement (too much scatter) — the media examination (red reflex, slit lamp) clinches this.
Colour vision interpretation:
- Ishihara 17/17 (or 16/17): normal colour vision.
- <13/17: significant red-green colour deficiency — red-green colour confusion hazards (military, aviation, transport, fire services). Acquired colour defects (e.g. from optic neuritis, glaucoma) tend to cause red-green desaturation (assessed by red cap desaturation test) rather than the plate-reading pattern of congenital deficiency.
Menace and blink reflex interpretation:
- Menace reflex absent in a child >4–6 months: suggests visual field loss, optic nerve damage, or a dense media opacity (the threat is not visually perceived); OR CN VII palsy (threat perceived but lids cannot close).
- Corneal reflex absent direct but consensual present when stimulating the SAME eye: suggests CN VII lesion (efferent absent, afferent intact). Absent both direct and consensual when stimulating one eye: CN V1 lesion (afferent gone — brain receives no signal regardless of which eye is the efferent).
CLINICAL PEARL
The 'good refraction, bad vision' trap — recognise clinically significant amblyopia: A child presents with VA 6/60 in one eye that does NOT improve with pinhole OR with spectacles, even when the spectacle prescription is perfect. The eye appears structurally normal on examination. This is amblyopia (lazy eye) — the neural connections for fine spatial vision were not established during the critical period because the eye was not used normally in early childhood (see OP1.5). The key clinical teaching point is: reduced VA that does not improve with optimal optical correction AND with no apparent structural cause = amblyopia until proven otherwise. The difference between amblyopia and organic disease may require detailed retinal and optic nerve examination to establish, but the pattern recognition — young patient, one eye, no structural correlate — is the first clinical flag.
Applied Practice: Clinical Decision-Making from VA Assessment
The clinical value of these tests lies in the decisions they drive. The following worked examples integrate the tests into clinical reasoning. These are the kind of cases you will encounter in PHC posting and in ophthalmology OPD.
Scenario A — Ravi, the truck driver (from the hook):
Ravi's unaided VA: RE 6/18, LE 6/9. With pinhole: RE 6/9, LE 6/6. Near VA: N6 in both eyes without spectacles. Colour vision: 17/17 Ishihara in both eyes. Menace and blink reflexes: present bilaterally.
Interpretation: Both eyes show significant VA improvement with the pinhole → the cause is refractive. The right eye has greater refractive error. Near VA is normal → the predominant error is likely myopia or astigmatism (not presbyopia, which would affect near first). Colour vision normal. Reflexes normal.
Decision: Refer for formal refraction and spectacle correction. If VA reaches 6/6 with the refraction, Ravi can continue driving with spectacles. No urgent referral required.
Scenario B — Gita, 55-year-old diabetic:
Gita's unaided VA: RE 6/60, LE 6/12. With pinhole: RE 6/60 (no improvement), LE 6/9 (modest improvement). Colour vision: RE unable to complete plates (only 8/17 correct), LE 15/17. Fundoscopy reveals dot-blot haemorrhages and hard exudates in the right macula.
Interpretation: Right eye VA does not improve with pinhole → organic cause. Left eye has some refractive component. Colour vision in the right eye is reduced — acquired colour defect consistent with macular disease. Fundoscopy reveals diabetic maculopathy.
Decision: Urgent ophthalmology referral for right eye (diabetic maculopathy with visual impairment). Left eye needs refraction and follow-up. The refractive component in the left eye may mask early maculopathy — fundoscopy of the left eye is essential.
Scenario C — Newborn assessment:
At the neonatal check, you elicit the blink reflex using a bright light (photo-blink reflex) in each eye separately. The menace reflex is NOT tested (normal to be absent until 3–4 months). You check for the red reflex (see OP3.x) and assess for gross visual tracking. Absence of the photo-blink or red reflex in a neonate warrants urgent ophthalmology referral to exclude retinoblastoma, dense cataract, or corneal opacity.
SELF-CHECK
A 4-month-old infant has an absent menace reflex in the right eye. The blink reflex (corneal reflex) is present in both eyes. Which of the following is the MOST appropriate next step?
A. Reassure — the menace reflex is normally absent until 3 months and is still developing at 4 months
B. Diagnose right CN VII palsy — the absent blink confirms efferent pathway damage
C. Refer for further evaluation of the right visual pathway — absent menace at 4 months warrants investigation
D. Test Ishihara plates to assess for colour vision deficiency
Reveal Answer
Answer: C. Refer for further evaluation of the right visual pathway — absent menace at 4 months warrants investigation
The menace reflex (threat reflex) normally develops by 3–4 months of age as the visual pathway myelinates. At 4 months, absence of the menace reflex on one side is at the developmental boundary and warrants careful evaluation. Crucially, the blink (corneal) reflex IS present — this tests CN V1 (afferent) and CN VII (efferent) — confirming the efferent facial nerve is intact. Therefore, the absent menace is NOT due to CN VII palsy. The most likely explanation is a defect in the right afferent visual pathway (CN II, retina) or a dense media opacity. Referral for further evaluation including red reflex, fundoscopy, and formal visual assessment is appropriate. Ishihara plates are not usable in a 4-month-old infant.
Self-Assessment: Applying VA and Reflex Testing Skills
The following self-assessment scenarios test your ability to integrate all the skills in this module into a clinical decision. Attempt each scenario before consulting your notes.
Scenario A: You are posted at a PHC. A 60-year-old farmer presents with gradual blur in both eyes for 3 years. Unaided VA: RE 6/60, LE 6/36. With pinhole: RE 6/18, LE 6/12. Colour vision: RE 12/17 Ishihara (errors on red-green plates), LE 16/17. Menace and blink reflexes: present bilaterally. (a) What does the pinhole improvement tell you about the primary cause? (b) Is the colour vision finding more consistent with congenital red-green deficiency or acquired colour defect? (c) What is the most likely underlying diagnosis for this bilateral VA loss in a 60-year-old? (d) What referral pathway exists under NPCBVI?
Scenario B: A 2-month-old infant is brought to a child health clinic. The mother is worried because the infant 'doesn't seem to see.' You test the menace reflex — absent bilaterally. The photo-blink reflex (bright light) is present bilaterally. The red reflex is present and symmetric bilaterally. (a) Is the absent menace reflex a cause for concern at 2 months? Explain the developmental basis. (b) Which component of the visual assessment is most reassuring, and why? (c) What would make this infant's assessment urgent?
Scenario C: A patient's right eye unaided VA is 6/24. With pinhole, it improves to 6/6. Colour vision in the right eye is 16/17 Ishihara. The right corneal reflex is absent (right eye — no direct response), but touching the right cornea produces a blink in the left eye (consensual response present). (a) Does the VA finding suggest organic or refractive pathology? (b) Which cranial nerve is likely damaged to explain the absent direct corneal reflex with preserved consensual response? Explain the neurological basis.
Review your answers against the material in this module. Gaps indicate sections to revisit before your OSPE assessment.