Page 9 of 32
OP10.3 | Headache and Refractive Error Referral Decisions — SDL Guide
Learning Objectives
- Explain the mechanism by which uncorrected hypermetropia and astigmatism cause headache
- Explain why myopia typically does not cause headache
- Describe the clinical features that suggest a refractive origin for headache
- Distinguish refractive headache from acute angle-closure glaucoma and convergence insufficiency
- Enumerate the red flag features of headache that mandate urgent non-ophthalmic referral
- State the indications for referral of a patient with headache and refractive error
INSTRUCTIONS
Headache is one of the most common complaints in clinical practice, and patients — and many doctors — readily attribute it to 'eye strain' from uncorrected refractive error. While this is sometimes correct, the ophthalmologist's role is to determine when the headache is truly of refractive origin, when it points to a sight-threatening ocular condition (acute angle-closure glaucoma), and when it signals a systemic or neurological problem requiring urgent referral. This module equips you with that decision-making framework.
References
- Khurana AK. Comprehensive Ophthalmology, 7th ed. New Age International, 2019. Ch. 2 (Refraction and Optics) and Ch. 10 (Glaucoma) (textbook)
- Parsons JH (revised by Ramanjit Sihota, Radhika Tandon). Diseases of the Eye, 23rd ed. Elsevier, 2022. Ch. 5 (Refraction) and Ch. 14 (Glaucoma) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 38-year-old schoolteacher presents to the general outpatient department with a two-month history of frontal headaches that begin after two to three hours of marking examination papers. The headache is relieved by rest and a pain reliever. She has never needed glasses. Her blood pressure is 126/82 mmHg. Her neurological examination is normal. The medical officer gives her an analgesic prescription and sends her away — but she returns three months later with the same complaint. Could a simple pair of reading glasses have resolved this entirely? And how do you know you are not missing something more serious?
WHY THIS MATTERS
As a general practitioner or district hospital doctor, you will encounter patients with headache attributed to 'eye strain' almost every week. The ability to distinguish a refractive headache — which is managed simply with spectacles — from acute angle-closure glaucoma (a sight-threatening emergency) or raised intracranial pressure (a life-threatening condition) is a fundamental clinical skill. The MBBS competency OP10.3 asks you to describe the role of refractive error correction in headache and enumerate the indications for referral — this SDL gives you the clinical logic for both.
RECALL
From your optics and physiology learning, recall that accommodation is the process by which the crystalline lens increases its curvature (via the ciliary muscle contracting and the zonular fibres relaxing) to bring near objects into focus. The eye's accommodative power is greatest in childhood and decreases with age as the lens stiffens — reaching clinical significance as presbyopia around age 40–45. Recall also that in a hypermetropic (long-sighted) eye, the eye is slightly shorter than normal and the light from a distant object is focused behind the retina — the ciliary muscle must contract (accommodate) even to see clearly in the distance. Contrast with a myopic (short-sighted) eye, where the eye is too long and distant objects focus in front of the retina — near objects, however, focus perfectly on the retina without any accommodative effort.
The Patient with Headache and Blurring: Clinical Presentation
The classic presentation of refractive headache is asthenopia — ocular fatigue, discomfort, and headache that develop after sustained near visual tasks such as reading, writing, working on a computer screen, or sewing. The headache is characteristically frontal or brow-ache in location, begins after a period of sustained near work (typically 1–3 hours), and is relieved by rest or by closing the eyes. In some patients, the headache builds progressively through the working day and is worst in the late afternoon or evening — consistent with accumulated accommodative fatigue. The patient may also report blurring of vision after prolonged near work, difficulty shifting focus from near to far ('after reading for an hour, the board looks blurry for a few minutes'), watering, and a tendency to screw up the eyes (squinting) when reading fine print.
A critical distinguishing feature in the history is the relationship to near work: a refractive headache is consistently triggered by near visual tasks and consistently relieved by rest. A headache that is present on waking in the morning (before any visual effort), that is positional (worse on bending forward), or that is associated with nausea and vomiting should immediately raise suspicion of a non-refractive cause.
Common presentations by refractive type:
- Hypermetropia: Frontal headache, worst after near work, may have normal distance VA (young patients compensate with accommodation) — the key is that distance VA may be 6/6 but the patient is working hard to achieve it.
- Astigmatism: Headache, brow-ache, and squinting (from trying to find the clearest focal plane); the symptom may occur even at distance.
- Presbyopia: Near headache and blurring in a patient aged 40+ who holds reading material at arm's length; cannot read fine print at the normal 33 cm working distance.
Refractive Errors and Their Headache Mechanisms
The mechanism by which refractive errors cause headache is primarily through sustained ciliary muscle effort (accommodation) and associated brow-ache from contraction of the frontalis and corrugator muscles during squinting.
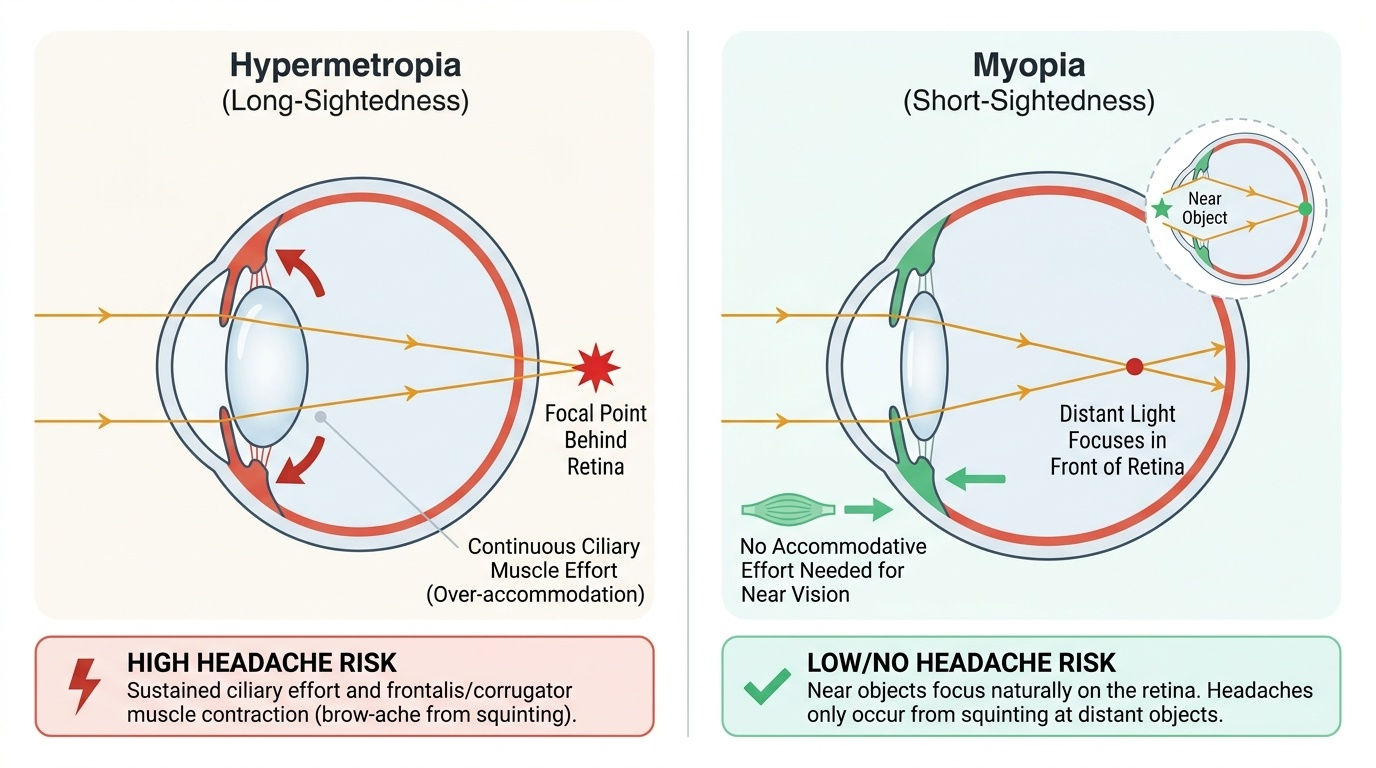
Provided image
Hypermetropia (long-sightedness): In a hypermetropic eye, the anteroposterior diameter of the globe is shorter than normal, causing parallel rays of light from a distant object to converge behind the retina rather than on it. To see even at distance, the ciliary muscle must contract to thicken the lens — this is continuous, involuntary accommodation. For near tasks, the accommodation required is even greater (distance accommodation + near accommodation). In young patients with good accommodative amplitude, this extra effort may be sustainable but causes frontal headache from prolonged ciliary and frontalis muscle tension. As the patient ages and the accommodative amplitude diminishes, the distance VA begins to drop and the headache intensifies. Uncorrected hypermetropia of even +1.00 to +2.00 DS can cause significant asthenopia in students or workers requiring sustained near work.
Astigmatism: The cornea (or less commonly the lens) has different curvatures in different meridians, producing two focal planes rather than one. The brain attempts to find the sharpest image by constantly adjusting accommodation between the two focal planes — an exhausting and impossible task. This sustained accommodative effort and associated frowning (to narrow the effective pupil aperture and improve depth of focus) causes frontal headache and brow-ache, even with relatively small degrees of uncorrected astigmatism (as little as 0.75 to 1.00 DC).
Myopia (short-sightedness): In a myopic eye, the globe is longer than normal and parallel rays from distant objects focus in front of the retina. For near objects (which diverge slightly), the rays converge further back and may focus on — or close to — the retina, requiring minimal or no accommodation. This is why myopia DOES NOT typically cause headache: near vision is naturally clear with no accommodative effort. A myope's headache is from squinting at distant objects, not from accommodation. Correcting myopia with minus lenses restores distance clarity without influencing near accommodation.
Presbyopia: After age 40–45, the crystalline lens progressively stiffens (nuclear sclerosis), reducing its ability to change shape for near focus. The amplitude of accommodation falls below the level needed for comfortable near work. The patient holds reading material further away, struggles with fine print, and develops near headache and fatigue. Reading glasses (convex lenses — add) provide the missing accommodative power.
Clinical Assessment of the Patient with Refractive Headache
A structured approach to the patient with headache of possible refractive origin begins with a careful history and proceeds to targeted examination. The assessment has three goals: confirm that the headache pattern is consistent with a refractive cause; measure visual acuity and refractive error; and exclude dangerous alternatives. The clinical assessment of refractive headache is fundamentally a process of pattern recognition combined with active exclusion of serious diagnoses. The most important habit to develop is resisting the temptation to attribute every headache to eye strain without performing the basic visual assessment — visual acuity, near vision, and the pinhole test take less than five minutes and together provide the evidence base for or against a refractive diagnosis. Equally important is recognising when the headache pattern does NOT fit a refractive cause: headache present on waking (before any visual effort), headache with nausea and vomiting, or headache associated with a red eye or visual disturbance require a fundamentally different diagnostic approach. A clinician who skips the systematic history and examination and prescribes spectacles for every patient with frontal headache will miss acute angle-closure glaucoma, raised intracranial pressure, and giant cell arteritis — all of which can present with periorbital pain.
History — the four key questions:
1. Is the headache consistently triggered by sustained near work and relieved by rest? (Refractive pattern: YES)
2. Is it present on waking? (Raised ICP or hypertension: YES; refractive: NO)
3. Are there associated symptoms — nausea, vomiting, red eye, haloes around lights? (Acute glaucoma: YES)
4. Is the patient 40+ years and struggling to read? (Presbyopia: YES)
Visual acuity (each eye separately, with current correction if any): Use the Snellen chart at 6 m for distance VA. Note: a hypermetropic patient may have 6/6 distance VA (compensated by accommodation) but still have refractive headache. Near VA is assessed at 33 cm using a Jaeger card or N-notation card.
Pinhole test: Placing a pinhole occluder in front of the eye reduces the effect of uncorrected refractive error on visual acuity. If VA improves with a pinhole, a significant refractive error is present. If VA does NOT improve with a pinhole, the blur has an organic (non-refractive) cause — macular disease, optic nerve pathology, amblyopia.
Refraction: Non-cycloplegic refraction (subjective refraction by the optometrist) is the starting point. In children and young adults where significant latent hypermetropia may be masked by accommodation, cycloplegic refraction (with cyclopentolate 1% or atropine 1%) is essential to reveal the true refractive error. A significant hypermetropia revealed only under cycloplegia — the latent component — can be the entire explanation for the headache.
Binocular vision assessment: Near point of convergence (NPC) — measured by bringing a fixation target from arm's length toward the nose until the patient reports doubling or one eye is seen to deviate. Normal NPC ≤10 cm. A receded NPC (>10 cm) indicates convergence insufficiency, an important cause of near-related headache not corrected by spectacles alone.