Page 7 of 30
OP2.2 | Lid and Lacrimal Procedures: Bell Phenomenon, Ptosis Evaluation, Massage and Epilation — SDL Guide (Part 3)
Interpretation of Findings and Clinical Decision-Making
The four procedures in this SDL generate objective measurements that directly guide management. This section builds interpretive fluency — the ability to look at a number and know what it means clinically.
Provided image
Bell's phenomenon grading and surgical risk: A positive Bell's (globe rotates well upward on closure) means that even if the lid is slightly under-corrected (not fully raised to the desired position) or slightly over-corrected (raised too much leaving a small gap on closure), the cornea will be largely protected by the reflex. A negative Bell's phenomenon means every millimetre of over-correction translates directly to exposed cornea. For this reason, in a patient with a negative Bell's, the surgeon targets an intentionally under-corrected result in ptosis surgery and counsels the patient that they will need eye drops for the rest of their life. This interpretation changes the surgical goal completely.
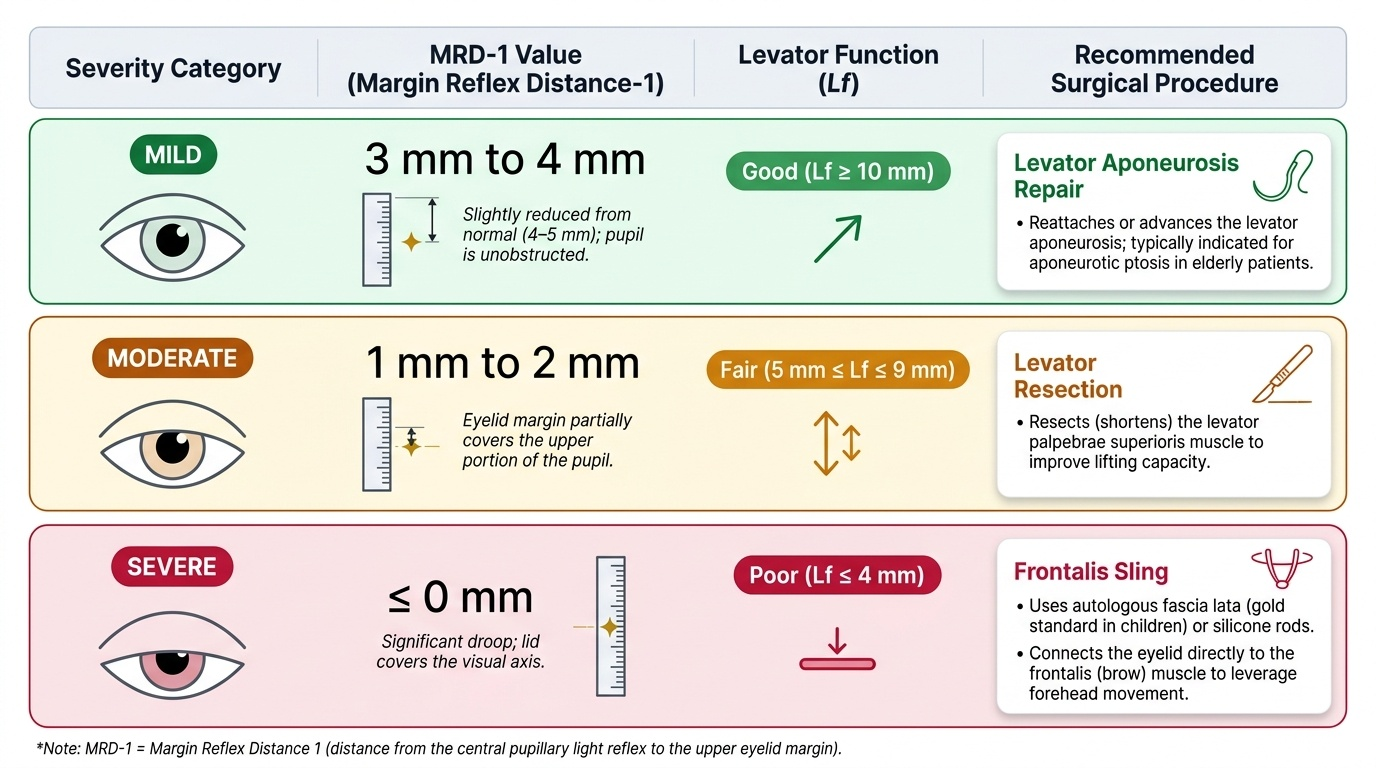
MRD-1 and levator function cross-reference: The two measurements together define both the severity of ptosis and the likely surgical approach. Consider:
A common clinical scenario: elderly patient, gradual upper lid drooping bilaterally, good levator function (14 mm), absent crease, normal MRD-1 only slightly reduced (3 mm) — this is aponeurotic ptosis; levator aponeurosis repair is the operation. Another: child with lifelong ptosis, poor levator function (2 mm), absent crease, MRD-1 of 0 — congenital myogenic ptosis; frontalis sling using autologous fascia lata (the gold standard in children) or silicone rod. These two scenarios require completely different surgery.
CNLDO resolution criteria: After Crigler's massage, resolution is confirmed when the epiphora stops and there is no mucopurulent discharge. On syringing, the fluorescein dye disappearance test (FDDT) demonstrates patent drainage — fluorescein instilled in the conjunctival sac disappears normally within 5 minutes when the duct is open. Failure of resolution by 12 months is the indication for probing.
Epilation response: After epilation, corneal epithelial erosions from the lashes heal within 24–48 hours if no other pathology is present. If healing is slow or the patient returns with new trichiatic lashes within 2 weeks, consider whether the underlying lid disease (trachoma, entropion) needs surgical correction rather than repeated epilation.
SELF-CHECK
A child with congenital ptosis of the right eye has an MRD-1 of 0 mm (the lid margin is at the level of the corneal reflex, occluding the visual axis), and levator function of 2 mm on standardised testing. Bell's phenomenon is positive. What is the correct surgical plan?
A. Levator aponeurosis re-attachment under local anaesthesia
B. Frontalis suspension sling (autologous fascia lata or silicone rod)
C. Fasanella-Servat procedure (superior tarsal resection)
D. Observation and patching to treat amblyopia only, no surgery yet
Reveal Answer
Answer: B. Frontalis suspension sling (autologous fascia lata or silicone rod)
Poor levator function (<4 mm — here 2 mm) with a visual-axis-threatening ptosis (MRD-1 = 0) and positive Bell's phenomenon indicates severe congenital myogenic ptosis where the levator muscle is functionally absent or fibrotic. The only viable operation is frontalis suspension — the upper lid is suspended from the frontalis muscle using a sling of autologous fascia lata (from the thigh) or silicone rod, using the brow elevation as the lid-opening mechanism. Aponeurosis repair and Fasanella-Servat both require good levator function (≥12 mm and fair LF respectively). Observation alone with amblyopia therapy would delay surgery and risk permanent visual loss.
Applied Practice: Putting It Together in the Clinic
In clinical practice, these four procedures are often performed in sequence during a single consultation. A worked example brings together the reasoning chain. Consider a 9-month-old infant brought for assessment of persistent right epiphora and mucopurulent discharge since birth. Your assessment proceeds as: (1) CNLDO suspected — confirm by pressing over the lacrimal sac and observing regurgitation of pus through the puncta (lacrimal regurgitation test). (2) Check that the lacrimal drainage anatomy is normal (no dacryocele, no fistula). (3) Teach the mother Crigler's massage — correct finger placement, downward direction, 4–6 times daily. (4) Prescribe topical antibiotic drops for the conjunctival discharge. (5) Book for review at 12 months — if not resolved, plan GA probing.
A second scenario: a 7-year-old girl presents with left upper lid droop noted by her teacher. Assessment sequence: (1) Measure visual acuity both eyes — is amblyopia already present? (2) Bell's phenomenon — positive bilaterally. (3) MRD-1 right = 4 mm, left = 1 mm (severe ptosis). (4) Levator function right = 15 mm (normal), left = 3 mm (poor). (5) Upper lid crease left = absent. (6) Assessment: congenital myogenic ptosis, poor levator function, amblyogenic MRD-1. (7) Urgent surgery: frontalis sling. (8) Post-operatively: occlusion therapy for any residual amblyopia.
A third scenario encountered in any general clinic: a 50-year-old farmer with trachoma-related bilateral trichiasis. Assessment: examine the lid margin and cornea at the slit-lamp — multiple inturned lashes touching the inferior cornea bilaterally, punctate corneal erosions. Perform epilation of the offending lashes. Document the number of lashes epilated per lid. Arrange surgery (posterior lamellar correction for the underlying cicatricial entropion) to prevent recurrence. Book the next epilation in 4–6 weeks.
In all three scenarios, the procedure generates the information that drives the management decision — this is what distinguishes a procedure with purpose from a routine task.
CLINICAL PEARL
The single most important pearl for Bell's phenomenon: always test Bell's phenomenon before any ptosis surgery. If the reflex is negative and the surgeon proceeds to raise the lid without accounting for this, the patient wakes up with the cornea fully exposed every night. Post-operative corneal ulceration in a patient with a negative Bell's phenomenon after ptosis surgery is a preventable tragedy. The pre-operative discussion with the patient must explicitly cover the expected gap on closure, the need for lifelong lubricants, and the intentionally under-corrected target MRD-1. For lacrimal massage: the most common error parents make is pressing on the nasal bone rather than the lacrimal sac fossa — always demonstrate the correct finger position during the clinic visit, not just describe it verbally.
Self-Assessment
Self-assessment for this module requires integration across the four clinical skills covered: Bell phenomenon testing, ptosis evaluation with MRD-1 and levator function measurement, lacrimal sac massage technique in infants, and epilation of aberrant lashes. In clinical OSCEs and viva examinations, examiners expect precise numerical values — MRD-1 cutoffs, levator function grades, success rates of conservative management — because these numbers directly determine operative versus non-operative decisions. The clinical importance of Bell phenomenon cannot be overstated: an absent Bell phenomenon in a patient with facial palsy or planned ptosis surgery represents a corneal protection risk that must be proactively managed. Similarly, knowing when to refer for ptosis surgery in a child (detecting amblyopia threshold) versus an adult (cosmetic or functional threshold) reflects competency-level reasoning. Review the following self-assessment questions to consolidate your learning from this module. These mirror the type of questions asked in ophthalmology clinical examinations and the NMC professional assessment.
- What is the normal range for MRD-1, and how does it change with each degree of ptosis severity (mild/moderate/severe)?
- What is the significance of a levator function of 3 mm in a child with ptosis — which operation is indicated?
- A 55-year-old woman has right-sided lagophthalmos from Bell's palsy. Her Bell's phenomenon is absent. What are the risks and how do you manage them?
- At what age is CNLDO massage most appropriate, and what is the success rate of probing at 12 months?
- What are the two techniques for permanent eyelash ablation and what are their risks?
Expected answers: (1) MRD-1 normal = 4–5 mm; mild ptosis = 3 mm (1 mm below normal); moderate = 2 mm; severe = 1 mm or less. (2) LF 3 mm = poor levator function → frontalis suspension. (3) Absent Bell's + lagophthalmos = fully exposed cornea with closure; aggressive lubricants, protective moisture chamber spectacles, eye taping at night; gold weight implant to upper lid for permanent palsy; extremely low threshold for corneal ulcer treatment. (4) Massage from birth to 12 months; probing success ~90% at 12 months. (5) Electrolysis (needle radiofrequency, risk of follicular damage if misplaced) and cryotherapy (liquid nitrogen or nitrous oxide probe; risk of lid margin depigmentation and notching in dark-skinned patients).