Page 18 of 30
OP2.6 | Proptosis: Causes, Differentiation and Management — SDL Guide
Learning Objectives
- Enumerate the major causes of proptosis, classifying them by direction (axial vs eccentric), laterality (unilateral vs bilateral), and time course (acute vs chronic)
- Describe the differentiating clinical features of proptosis including Hertel measurement, direction of displacement, reducibility, pulsation, and lid signs
- Explain why intraconal lesions cause axial proptosis and extraconal lesions cause eccentric proptosis
- Distinguish pseudoproptosis from true proptosis on clinical examination
- Outline the investigations required and the management principles for proptosis, identifying sight-threatening emergencies requiring urgent intervention
INSTRUCTIONS
Proptosis — a forward protrusion of the eyeball — is one of the most diagnostically challenging presentations in ophthalmology. The same physical sign can result from a benign orbital fat prolapse, a slowly growing cavernous haemangioma, a rapidly invasive rhabdomyosarcoma in a child, or the familiar inflammation of thyroid eye disease. Making the correct diagnosis depends on applying a systematic framework: direction of displacement tells you which compartment harbours the lesion; laterality and time course narrow the differential; and specific examination findings guide urgent versus elective management. This module gives you that framework, grounded in orbital anatomy and illustrated with the clinical features that distinguish the major causes.
References
- Khurana AK. Comprehensive Ophthalmology, 7th ed. Chapter on Diseases of the Orbit (textbook)
- Parsons' Diseases of the Eye, 23rd ed. Chapter on Orbital Disease (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 45-year-old woman is brought to the ophthalmology outpatient clinic by her husband, who noticed over the past three months that her right eye appeared to be 'sticking out'. She reports mild discomfort on eye movement, some difficulty reading, and occasional redness. Her vision has not changed dramatically, but she finds bright light uncomfortable. On inspection, the right eye appears to protrude forward symmetrically — the cornea is visible below the upper lid even in primary gaze, and there is conjunctival congestion. The left eye looks normal. How do you confirm proptosis, and where do you begin your diagnostic search?
WHY THIS MATTERS
Proptosis is a clinical sign — not a diagnosis — and the underlying cause ranges from the common (thyroid eye disease) to the rare but life-threatening (orbital apex malignancy). A clinician who cannot systematically evaluate proptosis will miss a sight-threatening compressive optic neuropathy in a thyroid patient, delay the diagnosis of rhabdomyosarcoma in a child, or fail to recognise that an apparent proptosis is actually pseudoproptosis caused by contralateral enophthalmos. At the MBBS level, OP2.6 requires you to enumerate causes, describe differentiating features, and outline management — the diagnostic and therapeutic competencies that will make you effective in the outpatient clinic, the emergency department, and the referral chain.
RECALL
Before proceeding, revisit the following from Year-1 Anatomy:
1. Orbital anatomy: The orbit is a bony pyramid of approximately 30 mL volume, bounded by seven bones (frontal, zygomatic, maxilla, palatine, lacrimal, ethmoid, sphenoid). The orbital apex opens posteriorly through the optic canal (optic nerve, ophthalmic artery) and the superior orbital fissure (cranial nerves III, IV, V1, VI; superior ophthalmic vein). The orbit is a closed bony space — any increase in orbital volume directly raises intraorbital pressure.
2. Orbital septum: The orbital septum is a fibrous sheet extending from the periosteum of the orbital margins to the tarsal plates. It is the surgical and anatomical boundary between preseptal (periorbital) and postseptal (orbital) compartments. Infections and masses posterior to the septum are orbital and potentially sight-threatening; those anterior are preseptal and rarely threaten vision.
3. Extraocular muscle cone: The four rectus muscles and their intermuscular membranes form the muscle cone, dividing the orbit into an intraconal compartment (within the cone, containing the optic nerve and its associated structures) and an extraconal compartment (outside the cone). This distinction is the key to understanding the direction of proptosis that a lesion produces.
4. Thyroid eye disease: Briefly revisit from the preceding OP2.3 SDL — TED is autoimmune, involves glycosaminoglycan deposition in orbital fibroblasts and EOM belly enlargement, and is the commonest cause of proptosis in adults.
A Patient with a Bulging Eye: Recognising Proptosis
Proptosis (also called exophthalmos when it specifically refers to thyroid-related forward protrusion) is the abnormal forward displacement of the eyeball within the orbit. The displacement can be symmetric or asymmetric; the onset can be indolent over months or explosive over hours. Recognising proptosis begins with the simple clinical observation of the globe's position relative to the orbital rim and the fellow eye.
The symptom complex that brings patients to the clinic reflects the mechanical and compressive consequences of a mass in a rigid bony compartment, because the orbit is a four-walled bony cone with only one opening — anteriorly through the orbital aperture — any increase in orbital volume pushes the globe forward. This is why proptosis is the cardinal sign of any space-occupying orbital lesion, whether inflammatory, vascular, neoplastic, or endocrine in origin:
- Exposure keratopathy: incomplete eyelid closure (lagophthalmos) exposes the inferior cornea, causing dry eye, foreign-body sensation, redness, and — if severe — corneal ulceration.
- Diplopia: orbital masses compress or restrict the extraocular muscles, producing gaze restriction and double vision.
- Visual blurring or loss: either from corneal involvement (exposure) or, more seriously, from compressive optic neuropathy at the orbital apex.
- Periorbital fullness and lid swelling: particularly with inflammatory or neoplastic lesions.
- Epiphora: lacrimal drainage obstruction by a medial or inferior mass.
- Pain: suggests inflammation (orbital cellulitis, myositis), acute angle-closure, or malignancy invading periosteum.
The clinical scenario above — a 45-year-old woman with three months of slowly progressive unilateral axial proptosis and ocular surface discomfort — is the textbook presentation of a benign intraconal orbital tumour or thyroid eye disease. The time course and direction of displacement are the first diagnostic filters. Before constructing a differential, the clinician must confirm that proptosis is real (not pseudoproptosis) and measure it precisely.
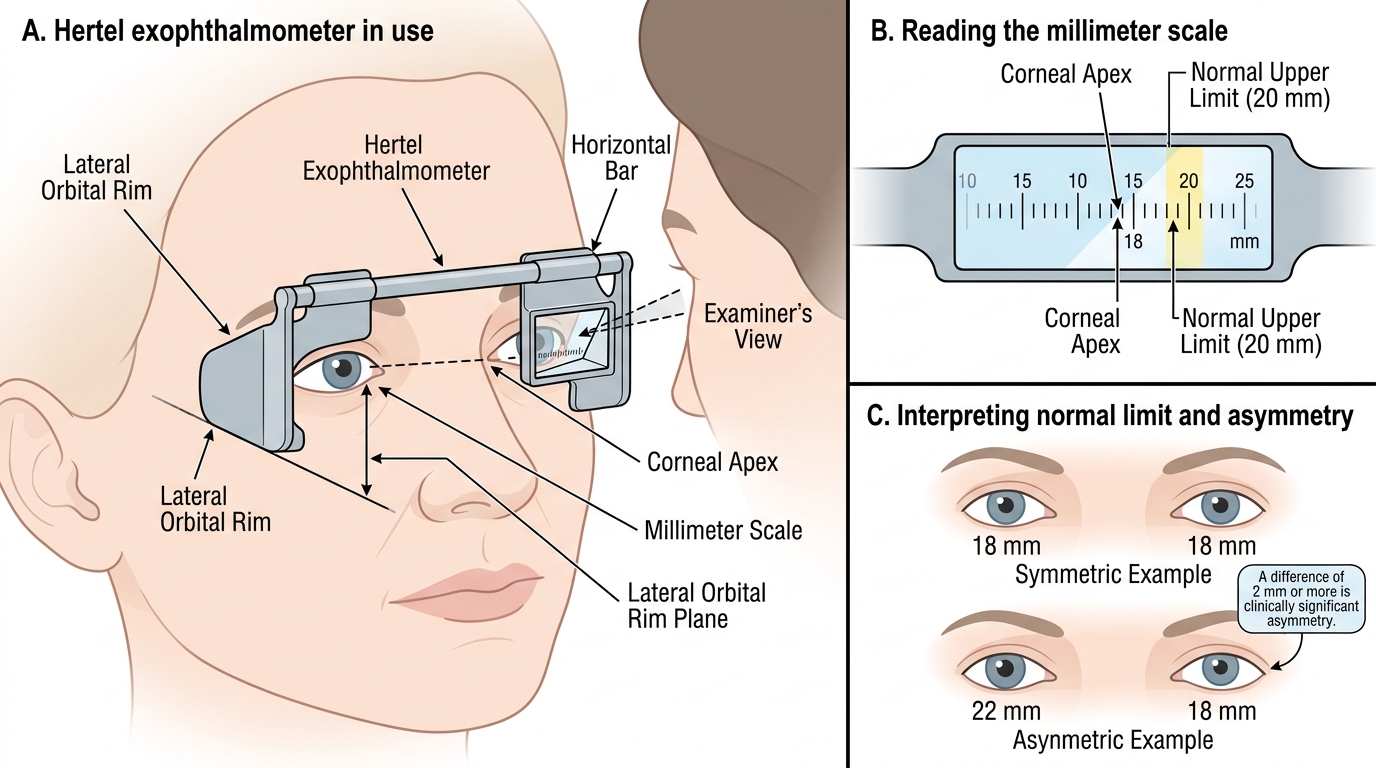
Hertel Exophthalmometry: Technique and Interpretation
Orbital Anatomy and Pathophysiology of Proptosis
Understanding why a given lesion produces the type of proptosis it does requires a clear mental model of the two orbital compartments defined by the extraocular muscle cone.
The intraconal compartment lies within the muscle cone formed by the four rectus muscles and their intermuscular septa. Its contents are the optic nerve, central retinal artery and vein, ciliary nerves, and the orbital fat immediately surrounding the nerve. A lesion that arises in the intraconal space expands in all directions equally, pushing the globe straight forward along the orbital axis — producing axial proptosis with no displacement up, down, or to either side. The classic intraconal lesions are cavernous haemangioma (commonest benign adult intraconal tumour), optic nerve glioma, and optic nerve sheath meningioma.
The extraconal compartment lies outside the muscle cone, between the cone and the bony orbital walls. It is subdivided by position: superior, inferior, medial, and lateral. A lesion in the extraconal space cannot expand posteriorly (blocked by the apex) or laterally (bone), so it pushes the globe in the direction away from the lesion — producing eccentric proptosis. A lesion in the superior orbit displaces the globe downward and forward; a lacrimal gland tumour (superolateral) displaces the globe inferomedially; a medial subperiosteal abscess displaces the globe laterally. Classic extraconal lesions include lacrimal gland tumours, dermoid cysts (at the frontozygomatic or frontolacrimal suture lines), rhabdomyosarcoma (commonest childhood primary orbital malignancy), and subperiosteal abscess (complication of sinusitis).
Why the orbit's rigidity matters: unlike the skull, where tumour growth can be accommodated by CSF shifts, the orbit is rigid and cannot expand. Any increase in orbital volume — even 3–4 mL — raises intraorbital pressure significantly, compressing venous outflow, the optic nerve sheath, and ultimately the nerve itself. This is the mechanism of compressive optic neuropathy, the most sight-threatening complication of proptosis. Colour vision deteriorates before visual acuity because the parvocellular fibres subserving colour are more sensitive to compression than the achromatic channels — hence colour testing at every visit is the key safety check.
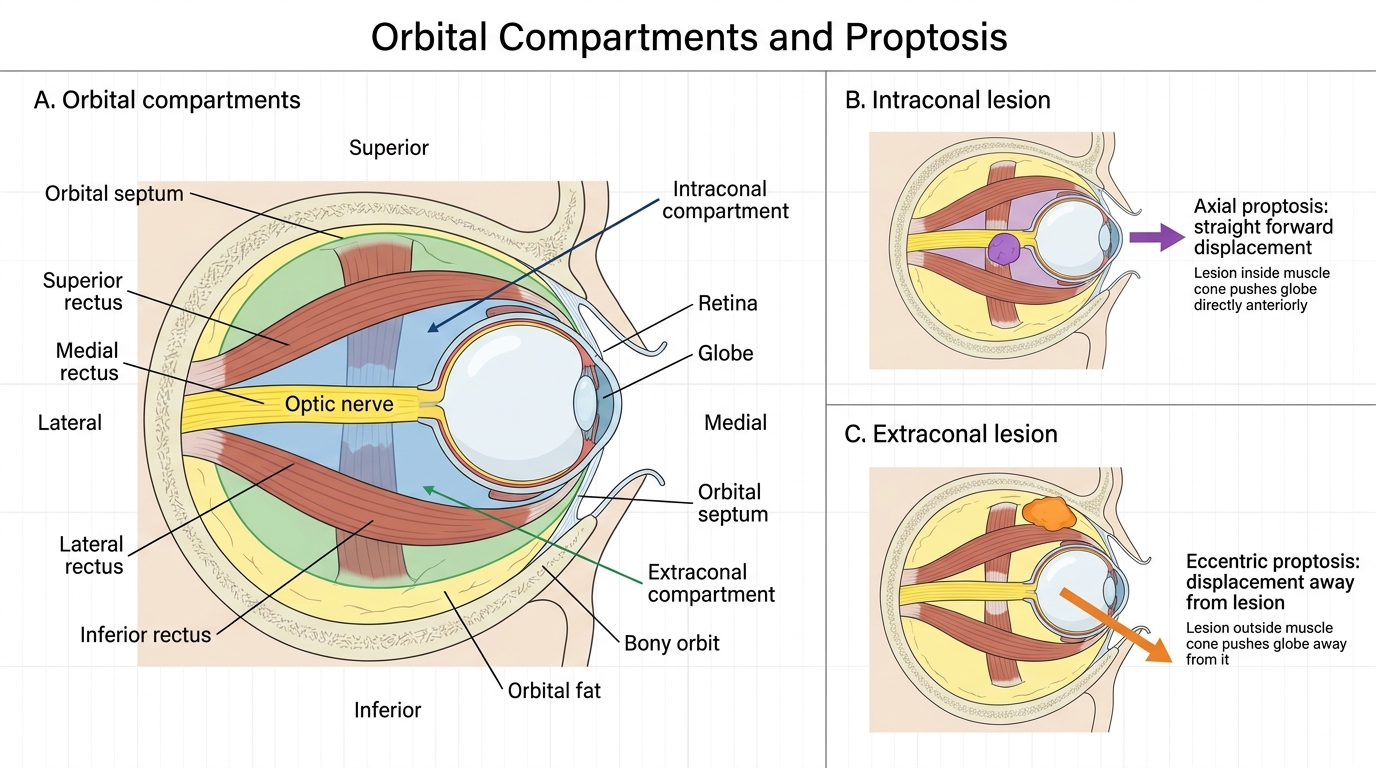
Orbital Compartments and Direction of Proptosis
Classification of Proptosis: Direction, Laterality and Time Course
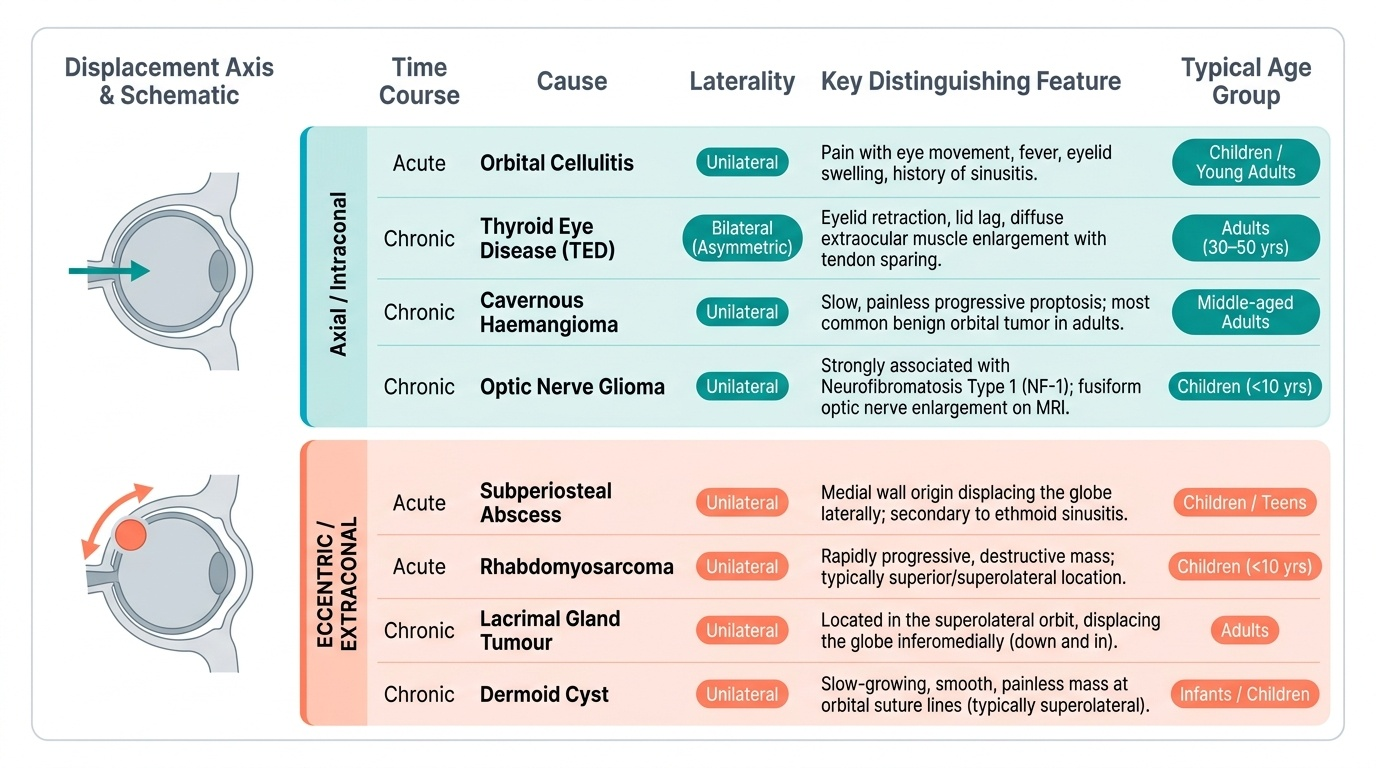
Applying a systematic classification to proptosis is more than a revision exercise — it is a diagnostic algorithm that experienced ophthalmologists run mentally at the bedside. The orbit is a compact bony structure housing the globe, extraocular muscles, optic nerve, lacrimal gland, and orbital fat, all tethered by fibrous septa. A lesion displacing the globe in any direction communicates its tissue of origin through that direction: an intraconal lesion pushes straight forward, a lacrimal gland tumour pushes inferomedially, an ethmoid sinus mucocele pushes laterally, and a subperiosteal abscess displaces the globe away from the infected sinus wall. Mastering the three-axis framework below allows instant generation of the correct differential.
Provided image
A systematic three-axis classification of proptosis is the most practical clinical framework. Applying these three axes in sequence — direction of displacement, laterality, and time course — rapidly narrows the differential from dozens of causes to three or four.
Axis 1: Direction of displacement
- Axial (straight forward): intraconal lesion. The globe protrudes along the orbital axis with no lateral or vertical displacement. Major causes: cavernous haemangioma, optic nerve glioma, optic nerve sheath meningioma, thyroid eye disease (which causes diffuse EOM enlargement and predominantly axial proptosis), orbital lymphoma (can be intraconal or diffuse).
- Eccentric (downward, medial, or lateral displacement): extraconal lesion. Direction of displacement indicates the compartment opposite the lesion. Major causes: lacrimal gland tumour (superolateral → inferomedial displacement), dermoid cyst (superolateral at suture lines), rhabdomyosarcoma (variable, typically superior or superolateral), subperiosteal abscess (medial wall → lateral displacement), mucocele of sinuses (medial/superior → lateral/inferior displacement).
Axis 2: Laterality
- Unilateral: the great majority of orbital tumours, infections, inflammatory pseudotumour, mucocele, and vascular lesions are unilateral.
- Bilateral: thyroid eye disease is the commonest cause of bilateral proptosis in adults — this is a high-yield fact. Other bilateral causes include systemic lymphoma, bilateral metastases, and bilateral cavernous sinus lesions.
Axis 3: Time course
- Acute (<48 hours): orbital haemorrhage (post-trauma or spontaneous), cavernous sinus thrombosis, orbital cellulitis with abscess, acute orbital haemorrhage from vascular malformation.
- Subacute (days to weeks): orbital cellulitis, rhabdomyosarcoma in children (notorious for rapid growth), inflammatory orbital pseudotumour.
- Chronic (months to years): cavernous haemangioma, meningioma, lacrimal gland pleomorphic adenoma, thyroid eye disease, benign lymphoma.
Pseudoproptosis is the apparent forward displacement of the globe without true increase in proptosis on Hertel measurement. Recognising it avoids unnecessary investigation. Causes:
- Contralateral enophthalmos (the sunken eye on the left makes the normal right look proptosed)
- Ipsilateral lid retraction (TED: lid retraction exposes the sclera above the limbus, mimicking proptosis)
- High axial myopia (enlarged globe elongated posteriorly, physically displaced forward in the orbit)
- Buphthalmos (enlarged globe in congenital glaucoma)
SELF-CHECK
A 5-year-old boy presents with rapidly progressive proptosis of 2 weeks duration, downward and forward displacement of the left globe, and periorbital bruising. He is systemically well. What is the most likely diagnosis?
A. Orbital cellulitis
B. Rhabdomyosarcoma
C. Capillary haemangioma
D. Optic nerve glioma
Reveal Answer
Answer: B. Rhabdomyosarcoma
Rhabdomyosarcoma is the commonest primary orbital malignancy in children. The classic presentation is a child under 10 years with rapidly progressive eccentric proptosis (extraconal, typically superior orbit → inferomedial displacement) over days to weeks. It can mimic inflammation. Urgent biopsy and paediatric oncology referral are required. Capillary haemangioma grows in infancy but is typically soft, compressible, and superficial. Optic nerve glioma causes axial proptosis (intraconal). Orbital cellulitis causes acute proptosis with fever, chemosis, and EOM restriction.