Page 15 of 27
OP3.5 | Pterygium — SDL Guide (Part 2)
Differential Diagnosis: Pterygium vs Pseudopterygium and Other Lesions
Several conditions can be confused with pterygium on first inspection. The most important differential is pseudopterygium, because the management is different and the distinction requires a simple bedside test.
Provided image
Pseudopterygium:
A pseudopterygium (false pterygium) is an adhesion between the bulbar conjunctiva and the cornea that forms after a chemical burn, thermal injury, severe corneal ulceration, or trauma. Unlike a true pterygium, it does NOT originate from the limbal tissue — it is a secondary adhesion of conjunctival tissue to a damaged corneal surface. The key distinguishing test is the probe test: pass a lacrimal probe (or the end of a cotton bud) beneath the pseudopterygium at the limbus. In a true pterygium, the probe CANNOT pass through (the tissue is adherent to the cornea from the limbus forward); in a pseudopterygium, the probe CAN pass through at the limbus because there is a gap between the conjunctival adhesion and the underlying cornea at that point.
Other distinctions:
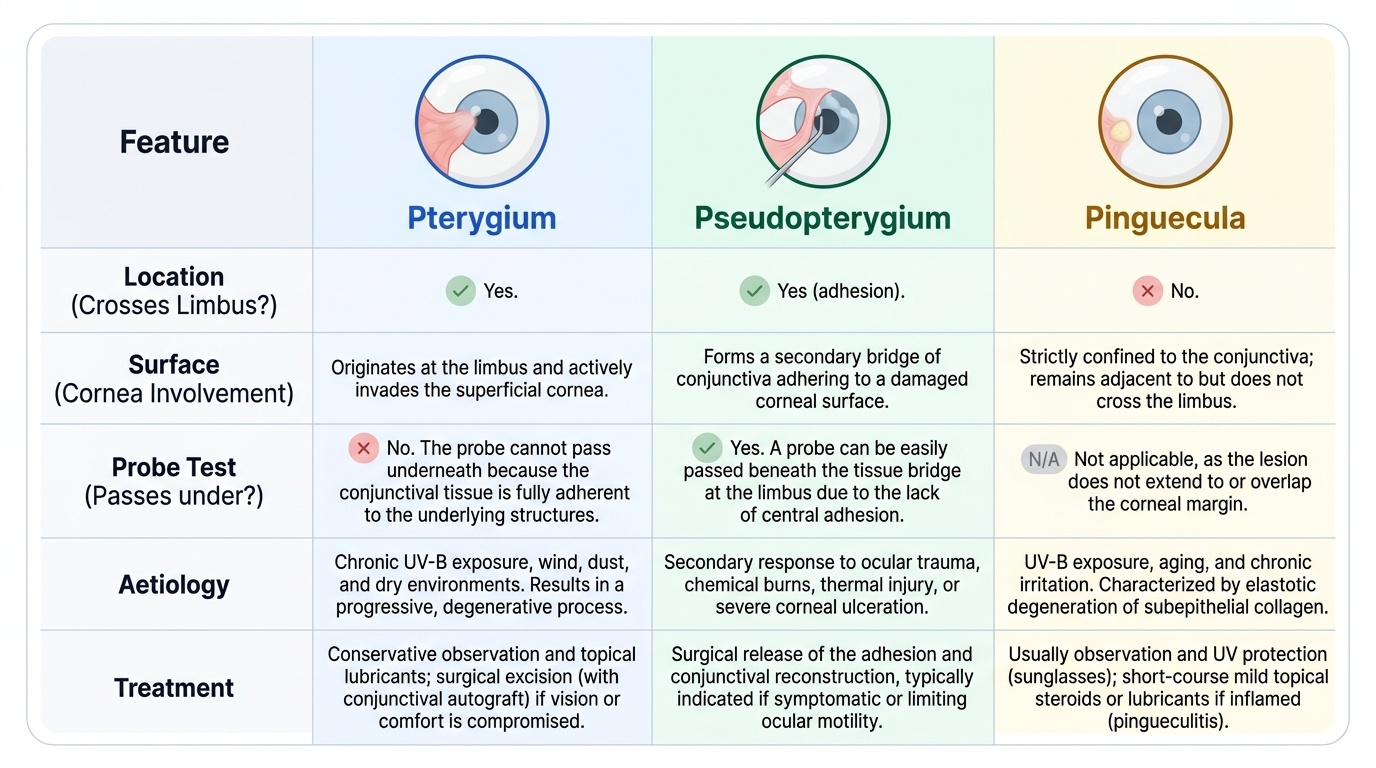
| Feature | Pterygium | Pseudopterygium | Pinguecula |
|---|---|---|---|
| Crosses limbus onto cornea | Yes | Yes (adhesion) | No |
| Probe passes at limbus | No | Yes | N/A |
| Aetiology | UV-B, chronic exposure | Chemical burn / trauma / ulcer | UV-B; degenerative |
| Treatment | Observation or surgery | Surgery (if symptomatic) | Observation (usually) |
Pinguecula:
A pinguecula is a yellowish-white deposit of degenerated conjunctival stroma in the interpalpebral zone (usually nasal, occasionally temporal), just inside the limbus. It does NOT cross the limbus onto the cornea — it remains confined to the conjunctiva. Histologically, it shows elastotic degeneration of the subepithelial collagen (Bowman's zones replaced by actinic elastosis). It is considered a precursor lesion or associated finding of pterygium. Most pingueculae are asymptomatic; when inflamed (pingueculitis), they cause redness and irritation treated with topical lubricants or short-course steroids.
Limbal dermoid:
A dermoid is a developmental choristoma (normal tissue in an abnormal location) at the limbus, usually white and smooth, containing hair follicles or sebaceous glands. It is present from birth and does not progress. It lacks the vascularity of pterygium.
Corneal pannus:
Superficial vascularisation of the cornea (extending from the limbus) in trachoma (superior pannus) or from other causes; it can be confused with a pterygium if the clinical history is not taken carefully.
CLINICAL PEARL
The probe test is fast, cheap, and definitive for pterygium vs pseudopterygium — and it changes management. A pseudopterygium from a chemical burn requires different surgical planning (often limbal stem cell transplantation rather than simple excision) and has different recurrence risks. Always perform the probe test when the aetiology is not clear from the history. Ask: 'Did anything splash in your eye or burn your eye in the past?' — the affirmative history plus a positive probe test seals the diagnosis of pseudopterygium.
Management: When to Treat and How
Pterygium management follows a conservative-to-surgical escalation based on the degree of corneal involvement, visual impact, symptoms, and rate of progression. Not all pterygium needs surgery — the surgery itself carries a risk of recurrence (sometimes worse than the original growth) and should not be performed for purely cosmetic reasons in stable, visually uninvolved pterygium. This conservative-first principle is important to internalise because patients with a visible 'growth on the eye' often request early surgery for cosmetic and psychological reasons, and the clinician's role is to provide accurate risk-benefit counselling: for a stable pterygium more than 3 mm from the pupil with normal VA, the recurrence risk from surgery (which can be higher than 50% with older techniques) outweighs the benefit of early excision. Conversely, a pterygium that is approaching the visual axis, growing on serial measurements, or causing visually significant induced astigmatism that is not correctable with spectacles requires surgical referral — and the correct surgical technique (conjunctival autograft) must be specified to achieve a recurrence rate below 10%.
Indications for surgery:
- Pterygium approaching within 2–3 mm of the pupillary margin (visual axis threatened).
- Documented progressive growth on serial measurements.
- Visually significant induced astigmatism or reduced VA attributable to the pterygium.
- Restricted extraocular movement.
- Recurrent significant inflammation and redness causing patient distress despite conservative management.
- Patient is symptomatic and requests removal (cosmetically, with informed consent regarding recurrence risk).
Conservative (non-surgical) management:
- UV-protective sunglasses and hats — the most important preventive measure and reduces progression in established pterygium.
- Artificial tear drops — to reduce dryness, foreign body sensation, and inflammation.
- Topical lubricants — supportive for mild symptoms.
- Short-course topical steroids for acute pingueculitis/pterygium flares.
- Advising the patient against rubbing and minimising prolonged sun exposure.
Surgical options:
The recurrence rate varies dramatically with technique:
- Bare sclera technique: The pterygium is excised and the sclera is left bare. Simple and fast, but has an unacceptably high recurrence rate of 50–80% — often with more aggressive regrowth ('recurrent pterygium' can be worse than the original). This technique is now largely abandoned.
- Conjunctival autograft (CAG): The pterygium is excised and the bare scleral defect is covered with a free graft of the patient's own bulbar conjunctiva (usually taken from the superior bulbar conjunctiva). The graft provides a new epithelial barrier, inhibiting regrowth. Recurrence rate: <10%. This is the current standard surgical technique.
- Amniotic membrane graft: The defect is covered with human amniotic membrane; used when there is insufficient autologous conjunctiva (e.g. recurrent pterygium, large defects). Recurrence rate intermediate between bare sclera and autograft.
- Adjuvant mitomycin C (MMC): Mitomycin C is an alkylating antimetabolite that inhibits fibroblast proliferation. Applied topically (0.02–0.04%) intraoperatively (for 2–5 minutes) or postoperatively to the surgical bed, it further reduces recurrence risk. Its main complication is scleral thinning/melting (particularly with high concentrations or prolonged application) — a serious sight-threatening complication; hence it must be used with precise timing and concentration, not indefinitely.
- Beta irradiation: Strontium-90 applicator applied postoperatively to reduce fibroblast activity; used in some centres as an adjuvant; risk of scleral necrosis with excessive dose.
SELF-CHECK
A 45-year-old farmer with a 5-year history of pterygium undergoes surgical excision. The surgeon uses the 'bare sclera technique.' What is the expected recurrence rate with this technique?
A. Less than 10%
B. 50–80%
C. Less than 5%
D. 20–30%
Reveal Answer
Answer: B. 50–80%
The bare sclera technique — in which the pterygium is excised and the underlying sclera is left uncovered — has an unacceptably high recurrence rate of 50–80%. The high recurrence has led to its abandonment in favour of conjunctival autograft (CAG), which has a recurrence rate of <10% by providing a new epithelial barrier over the excised area. This is a commonly tested comparison in examinations and the principal argument for performing CAG as the standard surgical approach.
Self-Assessment
Review your mastery of the OP3.5 competency. You should be able to describe pterygium's aetiology (UV-B exposure, limbal stem cell failure), its three anatomical components (head/neck/body), and the pathognomonic Stocker's line; explain why pterygium-induced astigmatism does not improve with pinhole; perform the probe test mentally to distinguish pterygium from pseudopterygium; state the recurrence rates for bare sclera (50–80%) versus conjunctival autograft (<10%); and identify the main indications for surgery (proximity to visual axis, progressive growth, VA reduction, restricted EOM). Before attempting the self-test questions below, check that you can articulate the mechanistic reasoning behind each fact: why does pinhole NOT improve VA in pterygium-induced astigmatism (because the astigmatism is corneal distortion, not a refractive error that the pinhole can eliminate)? Why does the bare sclera technique have a 50–80% recurrence rate (because leaving the sclera uncovered allows conjunctival fibroblasts to rapidly migrate back onto the corneal surface)? Understanding the 'why' behind each testable fact ensures durable knowledge under examination pressure.
Revision questions:
1. A patient has a conjunctival growth that crosses the limbus onto the cornea, but the probe passes under the growth at the limbus. Is this a true pterygium or pseudopterygium? What is the likely aetiology?
2. Why does pterygium-induced visual blurring not improve with pinhole testing?
3. What is mitomycin C's role in pterygium surgery and what is its main serious complication?
4. Name the iron deposit at the leading edge of the pterygium head. What else would you put in the differential for a similar iron deposit at the corneal base (Fleischer ring) and at the horizontal corneal meridian in ageing (Hudson-Stähli line)?