Page 1 of 27
OP3.1 | Red Eye History Taking and Cause Framework — SDL Guide
Learning Objectives
- Demonstrate a systematic history-taking approach for a patient presenting with red eye
- Enumerate the causes of red eye by anatomical compartment
- Identify danger signs that distinguish sight-threatening conditions from benign causes
- Construct a differential diagnosis from the history pattern and make a referral decision
INSTRUCTIONS
Red eye is among the most common ophthalmic complaints in primary and secondary care. The history alone — the character of discharge, the presence or absence of pain, the effect on vision, and the pattern of redness — separates a benign self-limiting conjunctivitis from an acute angle-closure glaucoma or anterior uveitis that can cause permanent blindness within hours if missed. This module teaches the systematic history framework and cause classification that every MBBS graduate must apply before deciding whether a patient can be reassured or needs urgent specialist referral.
References
- AK Khurana — Comprehensive Ophthalmology, 7th ed., Ch. 6 (Diseases of Conjunctiva), Ch. 5 (Diseases of Cornea), Ch. 11 (Glaucoma) (textbook)
- Parsons' Diseases of the Eye, 23rd ed., Ch. 8 (Conjunctiva), Ch. 18 (Glaucoma) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 35-year-old schoolteacher walks into your clinic at 6 PM on a Friday with a red left eye. She reports the eye has been red since morning and 'feels scratchy.' There is no discharge, but she mentions her vision seems a little blurry. She has had one previous episode of something similar two years ago. She is otherwise fit and on no medications. You have five minutes before the pharmacy closes. Do you reassure her with lubricant drops and send her home — or do you refer her urgently? The answer turns entirely on what you ask her next and how you interpret the answers.
WHY THIS MATTERS
Red eye is one of the five most common presentations in outpatient ophthalmology globally, and a competency that every MBBS graduate will encounter in general practice, emergency medicine, and rural primary care long before any specialist arrives. Getting this history right is the difference between a patient who loses vision and one who is treated in time. The NMC CBME framework (OP3.1) designates this as a skill competency at the SH level — you are expected to demonstrate the technique in a simulated environment, not merely describe it. This module builds the mental framework and the scripted approach that you will practise in your skills laboratory sessions.
RECALL
Before we build the red eye framework, retrieve what you already know. The conjunctiva is a thin transparent mucous membrane lining the inner eyelids (palpebral) and covering the visible white sclera (bulbar) to the limbus — it is the most exposed ocular tissue. The cornea is the clear anterior dome; it is densely innervated (hence exquisite sensitivity) and is the main refracting surface. The uveal tract (iris, ciliary body, choroid) is the vascular middle coat — inflammation here is called uveitis and it is painful because the iris muscles go into spasm. The anterior chamber angle contains the trabecular meshwork through which aqueous humour drains — when this angle acutely closes, intraocular pressure spikes dangerously. These four structures are the main generators of a red eye, and knowing which one is inflamed tells you immediately how serious the situation is.
Why Red Eye Is Never 'Just Conjunctivitis'
Red eye — hyperaemia of the conjunctival and episcleral vessels — is the final common response of the anterior segment to a wide range of insults, ranging from trivial to vision-threatening. The clinical trap that catches juniors is anchoring on the most common cause (simple conjunctivitis) without actively ruling out the dangerous ones. The four conditions you must never miss in a red-eye consultation are acute angle-closure glaucoma (AACG), microbial keratitis (infective corneal ulcer), anterior uveitis (iritis), and scleritis — all of which share the surface appearance of 'red eye' but carry a real risk of permanent visual loss if treated with a simple antibiotic drop and sent home. Conversely, simple bacterial or viral conjunctivitis is not sight-threatening: the redness is real, the patient is uncomfortable, but the vision is preserved and there is no photophobia.
The epidemiological stakes are worth stating explicitly. Acute angle-closure glaucoma is the leading preventable cause of irreversible blindness from a red eye presentation; in South Asia, the prevalence of angle-closure disease is significantly higher than in Western populations because of the anatomically shallower anterior chambers prevalent in this region. Anterior uveitis can be the first presentation of systemic autoimmune disease (ankylosing spondylitis, juvenile idiopathic arthritis, sarcoidosis) and recurrent episodes cause posterior synechiae (iris–lens adhesions) that cloud the pupil and damage the lens. Microbial keratitis — bacterial, fungal, or Acanthamoeba — can destroy a cornea within 48 hours if treated as 'just conjunctivitis' with a weak antibiotic. The framework taught in this module operationalises a 'rule out dangerous causes first' discipline that you will use in every red-eye consultation for the rest of your career.
Key principle: The absence of any one danger sign (pain, photophobia, reduced visual acuity, ciliary flush, corneal opacity) makes a sight-threatening cause extremely unlikely. The presence of even one should prompt an urgent referral to an ophthalmologist.
Anatomy of the Red Eye: What Structures Can Inflame?
Understanding why different red eyes look different requires a brief revisit of the anterior segment anatomy as a framework for classification. The conjunctiva covers the visible sclera right up to the limbus (the junction between cornea and sclera) and lines the inside of the eyelids. Inflammation of the conjunctiva (conjunctivitis) produces redness that is most prominent in the fornices and peripheral bulbar conjunctiva — the vessels are large, bright red, and they blanch when you press on the globe, a feature called conjunctival injection. In contrast, inflammation arising from the cornea or uvea produces a different pattern: ciliary flush (also called circumcorneal injection or perilimbal flush), which is a violet-red ring of fine vessels immediately around the corneal margin that does NOT blanch on pressure. This one sign — ciliary flush versus conjunctival injection — is the single most important clinical sign in the red-eye examination.
The structures that generate red eye can be classified by anatomical compartment to build a structured differential:
- Conjunctival causes: conjunctivitis (bacterial, viral, allergic, trachoma), subconjunctival haemorrhage, pterygium, pingueculum.
- Corneal causes: keratitis (bacterial, viral HSV, fungal, Acanthamoeba), corneal abrasion, corneal foreign body, exposure keratopathy.
- Uveal causes: anterior uveitis (iritis), iridocyclitis, Fuchs' heterochromic cyclitis.
- Scleral/episcleral causes: scleritis (deep, painful, nodular or diffuse — can threaten scleral integrity), episcleritis (superficial, self-limiting, less painful).
- Adnexal/drainage causes: acute angle-closure glaucoma (raised IOP from angle closure), blepharitis, hordeolum (stye), chalazion, dacryocystitis (inflamed lacrimal sac).
Normal intraocular pressure (IOP) is 10–21 mmHg (Goldmann applanation). In acute angle-closure glaucoma, IOP may rise to 50–70 mmHg, causing corneal oedema (halos around lights), extreme pain, and nausea — a clinical picture that is sometimes misdiagnosed as acute abdomen because the vomiting dominates.
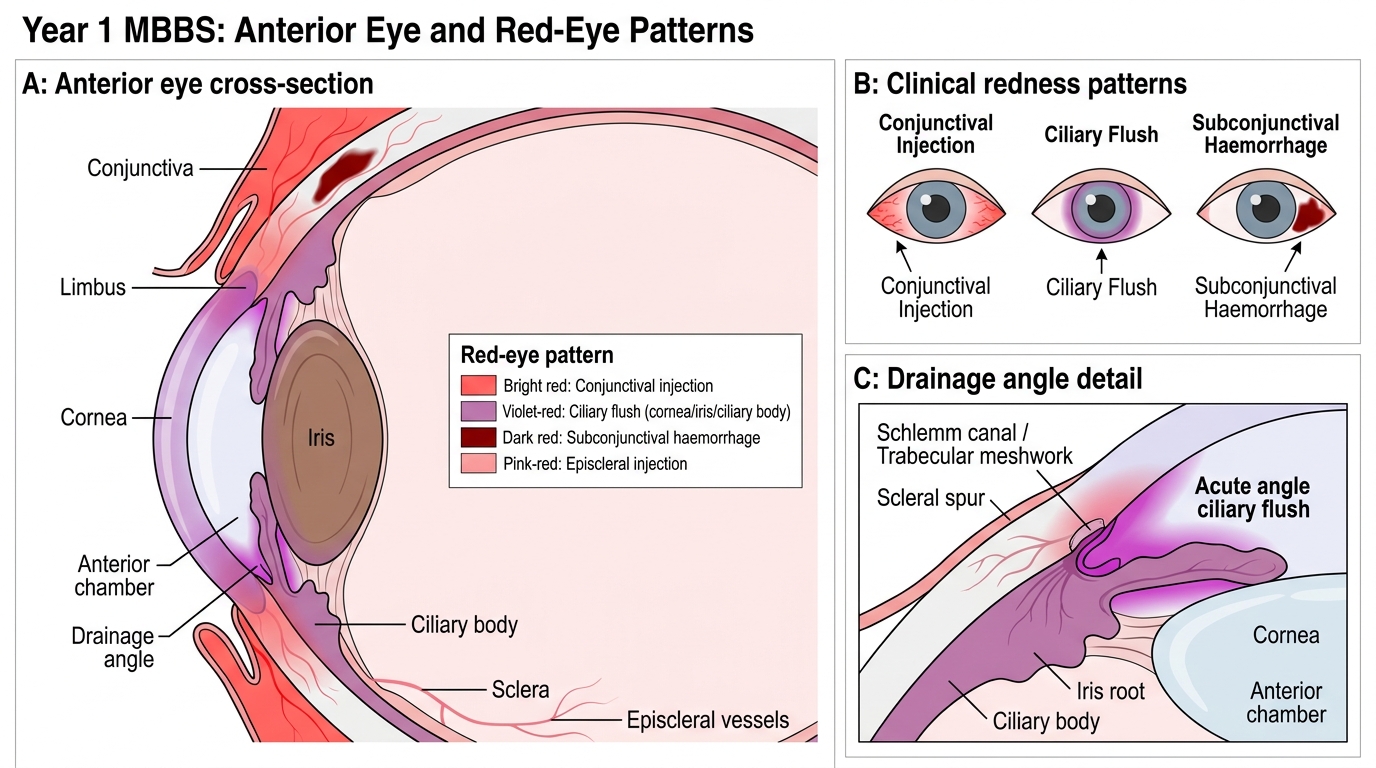
Anterior Eye Structures and Red-Eye Patterns
SELF-CHECK
A patient with a red eye has violet-red redness that is most prominent immediately around the corneal margin and does NOT blanch when you press on the globe. This pattern is called:
A. Conjunctival injection
B. Ciliary flush (circumcorneal injection)
C. Subconjunctival haemorrhage
D. Episcleral injection
Reveal Answer
Answer: B. Ciliary flush (circumcorneal injection)
Ciliary flush (circumcorneal or perilimbal injection) is fine vessel engorgement arising from the deep episcleral plexus around the limbus, driven by corneal or uveal inflammation. It does not blanch on pressure. Conjunctival injection is more prominent peripherally, is bright red, and blanches easily. Ciliary flush signals a potentially sight-threatening cause (keratitis, uveitis, acute angle-closure) and must not be dismissed as simple conjunctivitis.
The Systematic History Template
A structured history for red eye is not a random list of questions — it is a hypothesis-testing algorithm. You are systematically narrowing your differential from 'red eye (all causes)' to 'most likely one or two causes' using only what the patient tells you, before you even look at the eye. The structure below adapts the SOCRATES pain assessment framework to ophthalmic presentations and adds the ophthalmic-specific questions that the generic history omits. In the red-eye consultation, history-taking does most of the diagnostic work: a systematic enquiry about the character of discharge, the presence and severity of pain, the effect on vision, and any associated systemic symptoms will reliably separate benign conjunctivitis from the sight-threatening diagnoses before the slit-lamp is even activated. This matters because focused examination is only meaningful when the examiner already knows what they are looking for. A student who jumps straight to examining the eye without a history framework will see 'redness' and anchor on conjunctivitis; a student who follows the template below will already know whether to look for ciliary flush, a peaked pupil, or corneal opacity.
1. Onset and laterality:
- When did the redness begin? Sudden onset (minutes to hours) with severe pain suggests acute angle-closure glaucoma or trauma; gradual onset (hours to days) with mild symptoms favours conjunctivitis.
- Is it one eye or both? Bilateral simultaneous onset is typical of viral or allergic conjunctivitis; unilateral onset is more suspicious for keratitis, uveitis, or acute angle-closure.
2. Character of discharge:
- Watery/serous discharge → viral conjunctivitis or allergic conjunctivitis.
- Mucopurulent (yellow-green, thick, causes lid sticking) → bacterial conjunctivitis.
- No discharge → keratitis, uveitis, acute angle-closure, or subconjunctival haemorrhage.
- Ropy, stringy mucous → vernal/allergic conjunctivitis.
3. Pain and photophobia:
- Gritty, sandy discomfort without true pain → conjunctivitis, foreign body.
- Deep aching or throbbing pain → anterior uveitis, scleritis.
- Severe, lancinating pain + nausea/vomiting + seeing halos around lights → acute angle-closure glaucoma (emergency).
- Photophobia (pain on exposure to light) → uveitis (iris spasm) or keratitis (corneal nerve irritation). Its presence should immediately raise your suspicion for a dangerous cause.
4. Visual acuity change:
- Any reduction in vision is a danger sign. Ask: 'Can you see clearly? Has your vision changed at all?' Conjunctivitis typically does NOT reduce vision (mild blurring from discharge clears with blinking). Keratitis, uveitis, and acute angle-closure all reduce vision.
5. Trauma, contact lenses, foreign body:
- Recent trauma → corneal abrasion, laceration, subconjunctival haemorrhage, intraocular foreign body.
- Contact lens wear → strongly raises suspicion for Acanthamoeba keratitis (which presents with pain disproportionate to clinical signs) and Pseudomonas bacterial keratitis.
- Working with metal/wood/vegetative matter → metallic/inorganic/fungal corneal foreign body risk.
6. Systemic and previous history:
- Recent upper respiratory infection in contacts → adenoviral conjunctivitis (epidemic keratoconjunctivitis).
- History of ankylosing spondylitis, inflammatory bowel disease, psoriasis → strongly associated with anterior uveitis.
- Diabetes, immunosuppression → risk of atypical or severe infections.
- Previous episodes of red eye: recurrent unilateral red eye is characteristic of recurrent anterior uveitis or herpes simplex keratitis.
- Atopy, hay fever, eczema → allergic/vernal conjunctivitis.