Page 21 of 27
OP3.7 | Topical Ocular Medication Instillation and Patient Counselling — SDL Guide (Part 2)
Special Considerations: Multiple Drops, Ointments, and Suspensions
Many ophthalmic conditions require more than one medication, and most treatment regimens in glaucoma involve two or three drops daily. Managing multiple eye medications correctly requires understanding the rules of sequencing and the differences between the various formulation types.
Provided image
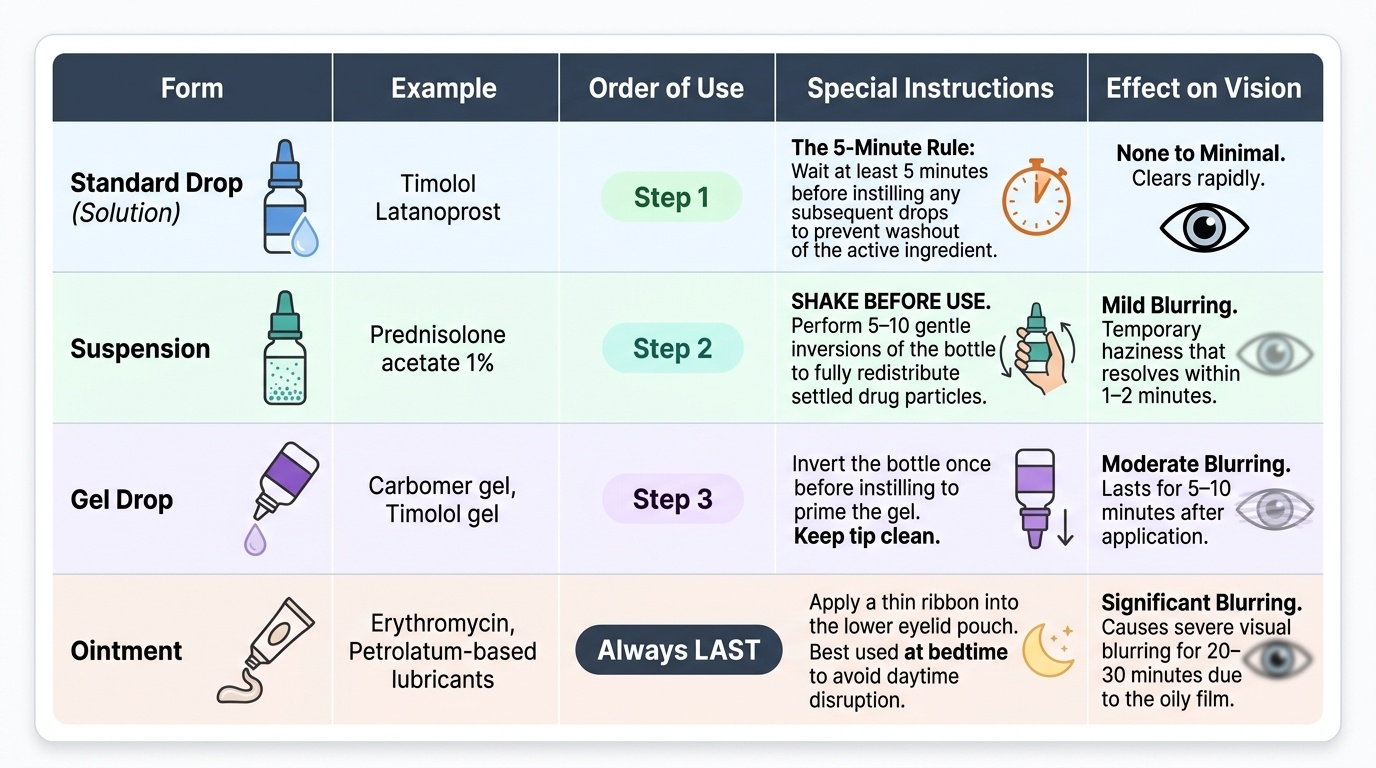
Multiple drops in the same session — the 5-minute rule:
When two or more different eye drops must be instilled at the same time of day, wait at least 5 minutes between each drop. The rationale is simple: the conjunctival sac holds only 7–10 μL; instilling a second drop immediately after the first simply washes out the first. After 5 minutes, the first drop has been absorbed through the corneal epithelium or drained, and the sac is ready for the next drug. The order of instillation should be least viscous first — the thicker the drop, the longer it stays in the sac and the more it delays the next drug.
Suspensions — shake before use:
Some eye drops are suspensions, not true solutions — the active drug particles are suspended in an aqueous vehicle. Examples: prednisolone acetate 1% (topical steroid), some antibiotic suspensions. Suspensions settle if left undisturbed; instilling an unmixed suspension delivers only the vehicle with minimal drug. The instruction 'SHAKE BEFORE USE' on the label must be followed literally — 5–10 gentle inversions of the bottle.
Eye ointments — always LAST, usually at bedtime:
Ointments are semi-solid preparations (petrolatum or lanolin base) containing the active drug. They stay in the conjunctival sac much longer than drops (half-life in sac approximately 1–2 hours vs minutes for drops) and are useful for conditions requiring prolonged contact (nocturnal antibiotic coverage, dry eye, viral conjunctivitis with aciclovir). However, ointments cause significant visual blurring for 20–30 minutes after application (due to light scattering by the oily film over the cornea). For this reason, when ointment and drops are prescribed together: instil all drops first (in the correct order, 5 minutes apart), then apply ointment last — at the end of the session. Patients who work or drive should be specifically advised to apply ointment at bedtime.
Preservative-free drops:
Most bottled eye drops contain a preservative — most commonly benzalkonium chloride (BAC) — to prevent microbial contamination of the bottle after opening. BAC is mildly toxic to the corneal epithelium and goblet cells, particularly with frequent use (more than 4× daily or combined multiple preserved drops). Patients requiring drops more frequently than 4× daily (e.g., lubricants for severe dry eye, frequent steroid courses), patients with pre-existing ocular surface disease, and patients using multiple preserved drops simultaneously should be prescribed preservative-free formulations (single-use unit-dose vials or multidose BAC-free bottles).
Self-instillation aids:
For patients with arthritis, tremor, or reduced dexterity, autodrops and drop guides hold the bottle and guide it over the eye, making correct positioning easier.
SELF-CHECK
A patient with primary open-angle glaucoma is prescribed latanoprost eye drops (once nightly) and brimonidine eye drops (twice daily). At the evening dose, he needs to instil both drops. The correct order and timing is:
A. Instil both drops simultaneously into the same eye at the same time
B. Instil brimonidine first, wait at least 5 minutes, then instil latanoprost
C. Instil latanoprost first, then brimonidine immediately after without waiting
D. Mix both drops in the cap and instil the mixture
Reveal Answer
Answer: B. Instil brimonidine first, wait at least 5 minutes, then instil latanoprost
When two eye drops are prescribed at the same time, they must be instilled at least 5 minutes apart to prevent the second drop from washing out the first. Brimonidine (an alpha-2 agonist) is typically instilled first because it is a standard solution; latanoprost (a prostaglandin analogue) is instilled second after the waiting period. The order (brimonidine before latanoprost vs latanoprost before brimonidine) is less critical than the 5-minute gap — but a consistent order should be established with the patient for compliance. Simultaneous instillation or mixing in the cap are both wrong and result in subtherapeutic drug levels.
CLINICAL PEARL
The simplest counselling analogy for nasolacrimal occlusion: tell the patient 'press the corner of your eye like you are holding in a tear for one minute.' Most patients immediately understand and replicate the technique correctly when the instruction is phrased this way. Abstract anatomical explanations ('occlude the punctum to prevent nasolacrimal drainage') are comprehensible to healthcare professionals but are rarely understood by patients at first hearing.
Patient Counselling and Medication Compliance
The final step of the OP3.7 competency is patient counselling — the transfer of the technical knowledge you have acquired into clear, actionable instructions that a patient will remember, understand, and follow at home. Studies consistently show that up to 50% of glaucoma patients are non-compliant with their drops within 12 months of prescription. Poor technique and inadequate counselling are among the most modifiable causes of treatment failure.
A structured counselling session for a patient starting a new eye drop should cover seven points:
1. What the drop is for and why it must be taken every day:
Explain the condition (e.g., glaucoma = raised IOP damaging the optic nerve) and that the drop controls IOP but does NOT cure the condition — missing doses allows IOP to rise and the nerve to be damaged silently. Compliance is non-negotiable.
2. How to instil the drop (demonstrate and ask the patient to demonstrate back):
Walk through the technique (head back, lower lid pocket, one drop, close gently, NLO for 1–2 minutes). Then ask the patient to repeat the technique on the other eye with water or saline as a dummy run. Teach-back is the most effective compliance technique — patients who demonstrate the technique back have significantly higher adherence rates.
3. Nasolacrimal occlusion — especially for systemic-risk drops:
For timolol, betaxolol, brimonidine, and topical steroids: explicitly explain why NLO matters. For timolol in a patient with asthma: 'This drop can pass through your nose and into your lungs if not occluded — please press the corner of your eye for one full minute every time you use it.'
4. Timing and frequency:
Prostaglandin analogues (latanoprost, bimatoprost, travoprost) are once-nightly because of their peak IOP-lowering effect at night and because some cause hyperaemia that is less disruptive during sleep. This timing is not negotiable for this drug class. Other drops (timolol twice daily, ciprofloxacin 4× daily) should be spaced evenly through the waking day — give specific times (e.g., 8 AM and 8 PM for twice-daily drops).
5. Storage:
Most eye drops should be stored at room temperature away from direct sunlight. Latanoprost (and other prostaglandin analogues) should be stored in the refrigerator before opening (2–8°C); once opened, they can be kept at room temperature for up to 6 weeks. Patients should check the storage instructions on the label.
6. Bottle hygiene and shelf life after opening:
Most multi-dose eye drop bottles should be discarded 28 days after first opening, regardless of how much liquid remains. This is because the preservative cannot indefinitely protect the contents from microbial growth. Do NOT keep bottles longer than this. Do NOT share eye drops with family members — even if they have a 'similar condition' — as this transmits ocular pathogens between individuals.
7. What to report:
Report any of the following: significant worsening of redness or pain; decreased vision; new systemic symptoms after starting a topical medication (shortness of breath with timolol → stop and seek medical review; weight gain with steroids → medical review).
Self-Assessment
Before your supervised clinical session for OP3.7, verify that you can perform the following without consulting notes: The questions below span both the technical (procedure steps, sequencing rules) and the clinical reasoning (pharmacokinetic basis of NLO, systemic risks of specific drugs, storage and shelf-life rules) components of the OP3.7 competency. For the counselling OSCE element, you will be asked to advise a simulated patient — typically a newly diagnosed glaucoma patient starting timolol — and the assessor will specifically check whether you cover the asthma/breathing risk, the NLO technique with its rationale, the timing and frequency, and the 28-day bottle-discard rule. Preparing a structured 3-minute counselling script and rehearsing it aloud against a timer is the most effective preparation for this station. The teach-back check — asking the patient to demonstrate the NLO technique back to you — is both a clinical best-practice and an assessor-visible indicator of a high-quality consultation.
- Demonstrate the complete drop instillation sequence (7 steps from hand washing to NLO) on a fellow student or simulation model.
- Explain nasolacrimal occlusion in one sentence understandable by a patient with no medical background.
- State the two most important clinical consequences of poor NLO technique — specifically the systemic drug that causes bronchospasm in asthmatic patients.
- State the 5-minute rule for multiple drops and explain its pharmacokinetic basis.
- State the order of administration when both drops and ointment are prescribed at the same time.
- Name the instruction that must be followed when the label says 'SHAKE BEFORE USE' and identify what type of formulation this indicates.
- State the standard shelf life of a multi-dose eye drop bottle after opening.
For your assessment, you will be asked to counsel a simulated patient (usually an actor playing a newly diagnosed glaucoma patient) on their new timolol eye drops. The assessor will specifically check whether you cover: the asthma/breathing risk, NLO technique, once-daily vs twice-daily timing, and storage. Prepare a 3-minute counselling script and rehearse it aloud at least once.