Page 17 of 33
OP4.6 | Corneal Blindness — SDL Guide
Learning Objectives
- Define blindness using the WHO classification and the Indian national programme definition
- Enumerate the causes of corneal blindness including infective, nutritional, traumatic, and congenital categories
- Describe the WHO classification of xerophthalmia and the management of keratomalacia
- Describe the stages of trachomatous blindness and the SAFE strategy for its control
- Outline the national and international programmes for prevention and control of corneal blindness in India
INSTRUCTIONS
Corneal blindness is one of the most visible inequities in global health — the majority of the 4.9 million people bilaterally blind from corneal disease live in low-income countries, and most of these cases were preventable. India carries a disproportionate share of this burden, driven by preventable post-infective scarring, vitamin A deficiency, and trachoma. This module provides the public health and clinical framework needed to understand, prevent, and address corneal blindness at community and clinical levels.
References
- Khurana AK. Comprehensive Ophthalmology, 7th ed. Ch 5: Diseases of the Cornea; Ch 19: Preventive Ophthalmology (textbook)
- Parsons' Diseases of the Eye, 23rd ed. Ch 9: The Cornea; Ch 24: Preventive Ophthalmology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 4-year-old boy is brought to the district hospital by his mother. He has been unable to see at night for 2 months, and his eyes 'look dry.' On examination, both corneas are dull, hazy, and soft — the right cornea has a punched-out area of softening that protrudes forward (descemetocele). The left has early haziness. Examination of his skin reveals follicular hyperkeratosis. He is severely malnourished, with a mid-upper arm circumference of 9 cm. He had measles 6 weeks ago. If you do not act in the next 24 hours, he will likely lose both corneas to perforation. This is keratomalacia — a medical emergency.
WHY THIS MATTERS
Corneal blindness affects approximately 4.9 million people worldwide, with the vast majority in South and Southeast Asia and Sub-Saharan Africa. India accounts for approximately 20–25% of global corneal blindness. Most of this blindness is avoidable — either preventable (vaccination, vitamin A supplementation, trachoma control, trauma prevention) or treatable (keratoplasty). For a medical graduate planning to practise in India, understanding the causes, prevention strategies, and national programmes for corneal blindness is not optional — it is a core public health competency directly tested in the MBBS final examination.
RECALL
From SDL 3: fungal and bacterial keratitis leave post-infective leukoma — the commonest cause of corneal blindness in India's working-age adults. From SDL 4: corneal opacity is graded as nebula, macula, or leukoma — only leukoma causes significant VA reduction if central. From SDL 1: the cornea's principal refracting role means any central opacity substantially reduces corrected VA. From general paediatrics: vitamin A is a fat-soluble vitamin essential for rhodopsin (retinal rod photoreceptor pigment) synthesis and for maintenance of mucus-secreting epithelia — its deficiency affects both the eye (xerophthalmia) and systemic mucous membranes.
Definition and Global Burden of Corneal Blindness
The World Health Organization (WHO) defines blindness as presenting visual acuity less than 3/60 (also expressed as 0.05 on the decimal scale, or 20/400 on Snellen equivalent) in the better eye, or a visual field of less than 10 degrees around central fixation regardless of VA. The WHO further categorises vision impairment: mild (VA <6/12), moderate (VA <6/18), severe (VA <6/60), and profound/blindness (VA <3/60). For programme purposes in India, the National Programme for Control of Blindness and Visual Impairment (NPCBVI) uses a national definition: presenting VA less than 6/60 in the better eye — a more inclusive threshold that captures a larger proportion of functionally blind individuals for planning purposes.
Corneal blindness is specifically defined as bilateral corneal opacity causing VA below the blindness threshold. Globally, it is estimated that approximately 4.9 million people are bilaterally blind from corneal disease — making it the fourth commonest cause of global blindness after cataract, glaucoma, and age-related macular degeneration. However, in South Asia and Sub-Saharan Africa, corneal blindness ranks second only to cataract among causes of avoidable blindness.
In India, the NPCBVI national survey data indicate that cataract remains the leading cause of blindness (about 66% of cases), but corneal pathology contributes substantially to avoidable and monocular blindness. The population most affected is children (vitamin A deficiency, congenital anomalies), agricultural workers (infective keratitis from vegetative trauma), and the elderly (Fuchs' dystrophy, cataract-surgery complications). The disease burden is concentrated in rural, low-income populations with limited access to tertiary ophthalmological care and eye banking services.
Causes of Corneal Blindness: An Aetiological Classification
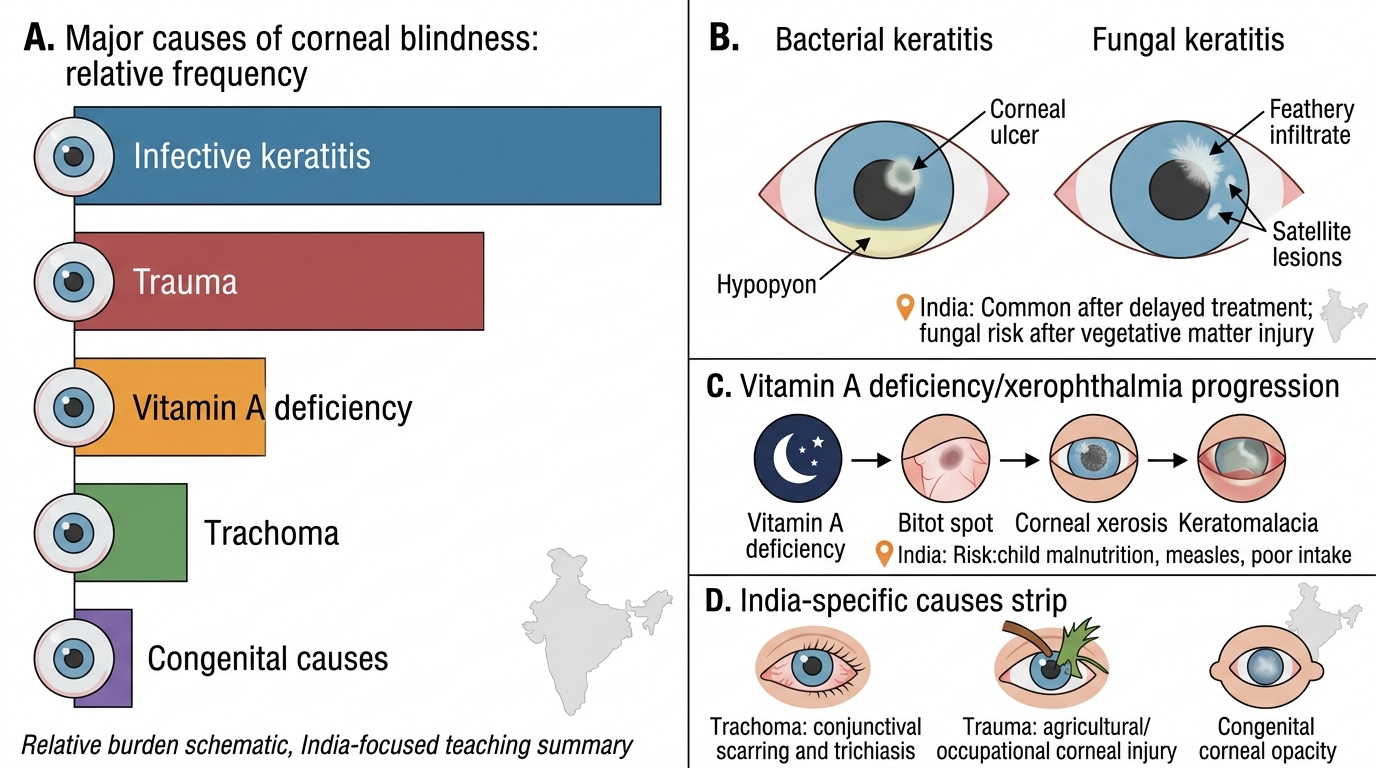
Corneal blindness arises from a variety of causes that can be grouped aetiologically into five categories. Understanding each category guides both clinical management and preventive strategy.
Infective causes form the largest category in India and low-income countries. Microbial keratitis — bacterial (Pseudomonas, Streptococcus pneumoniae) and fungal (Aspergillus, Fusarium) — leaves post-infective corneal leukoma after resolution. India's agricultural population has an exceptionally high burden of fungal keratitis from vegetative trauma, and inadequate or delayed treatment results in dense central leukoma. Trachoma (Chlamydia trachomatis) is the leading infectious cause of preventable blindness globally, though dramatically reduced in India since the SAFE strategy campaigns. In trachoma-endemic regions of north-west India and sub-Saharan Africa, recurrent infection leads to cicatricial lid disease, trichiasis, and ultimately corneal scarring.
Nutritional causes: Vitamin A deficiency is the leading cause of preventable corneal blindness in children under 5 worldwide. Severe deficiency causes xerophthalmia, progressing to keratomalacia — corneal softening and melting that can destroy both corneas within days. India's National Vitamin A Supplementation Programme has dramatically reduced the incidence of keratomalacia, but pockets of high prevalence persist in nutritionally vulnerable communities.
Traumatic causes: Mechanical trauma (penetrating eye injuries, corneal foreign bodies, blast injuries) and chemical burns (alkali burns — particularly lime, ammonia — are more devastating than acid burns because of ongoing saponification of the corneal stroma). Occupational eye injuries are preventable with appropriate protective eyewear.
Iatrogenic causes: Surgical complications — post-keratoplasty graft failure, post-cataract surgery pseudophakic bullous keratopathy, post-refractive surgery ectasia.
Congenital/developmental causes: Peters' anomaly, sclerocornea, and other anterior segment dysgeneses (described in SDL 2).
Major Causes of Corneal Blindness in India
Vitamin A Deficiency and Xerophthalmia
Vitamin A deficiency (VAD) causes a progressive spectrum of ocular disease collectively called xerophthalmia (from the Greek: dry eye disease). Vitamin A (retinol) is a fat-soluble vitamin that serves two distinct functions in the eye: first, as a precursor of retinal (11-cis-retinal), the chromophore of rhodopsin in retinal rod photoreceptors — its absence impairs night vision; second, as an essential regulator of epithelial differentiation throughout the body, including the conjunctival goblet cells that produce the mucin layer of the tear film. When vitamin A is deficient, the conjunctival epithelium undergoes squamous metaplasia — goblet cells are lost, the surface becomes keratinised and non-wettable, and the tear film becomes unstable. Progressive deficiency extends this process to the corneal epithelium, and ultimately to catastrophic stromal melting (keratomalacia). Understanding the mechanism explains why the disease stages progress in the order they do: night blindness comes first because rods are more sensitive to retinol deficiency than cone photoreceptors; conjunctival changes come next because the conjunctival epithelium is large and highly vitamin-A-dependent; corneal changes are a late and catastrophic manifestation once the systemic deficiency is severe. The WHO classification — used worldwide and commonly tested in examinations — stages the disease by its clinical manifestations from earliest (night blindness) to most severe (keratomalacia with corneal scarring), with each stage assigned a two-character code.
Provided image
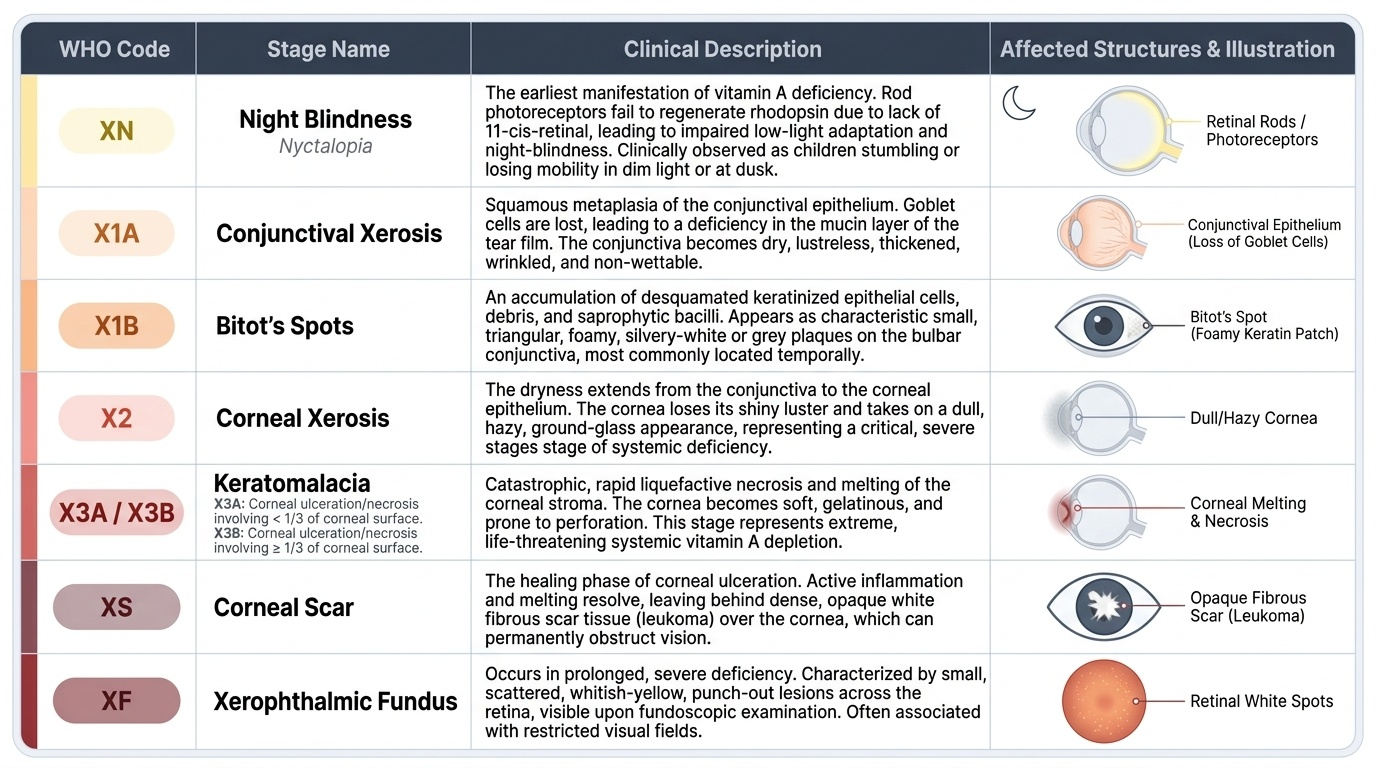
The WHO xerophthalmia classification proceeds as follows:
- XN — Night blindness (Nyctalopia): The earliest manifestation. Retinal rod photoreceptors require retinal (a vitamin A metabolite) for rhodopsin regeneration — deficiency impairs low-light vision. Children stumble in dim light or at dusk.
- X1A — Conjunctival xerosis: The conjunctival epithelium loses its goblet cells and becomes keratinised and non-wettable — appearing dry, dull, and granular ('like dry sand'). The conjunctiva loses the normal smooth, glistening appearance.
- X1B — Bitot's spots: Foamy, triangular, whitish deposits on the bulbar conjunctiva (typically temporal, sometimes nasal) — composed of keratinised epithelial debris and gas-forming bacteria (usually Corynebacterium xerosis). These are conjunctival, NOT corneal. They are pathognomonic of vitamin A deficiency in children, though isolated Bitot's spots in adults may be residual and not indicate active deficiency.
- X2 — Corneal xerosis: The corneal epithelium becomes non-wettable and hazy. At this stage, corneal involvement begins and blindness risk escalates.
- X3A — Corneal ulceration/keratomalacia involving less than one-third of the cornea: Corneal stromal melting (keratomalacia — from kerat-/cornea + -malacia/softening) begins. This is a medical EMERGENCY. The cornea may perforate within hours to days.
- X3B — Corneal ulceration/keratomalacia involving one-third or more of the cornea: More extensive corneal melting. Perforation risk is very high. Bilateral involvement in a severely malnourished child can result in bilateral blindness within 24–48 hours.
- XS — Corneal scarring (scar): Healed keratomalacia leaves a dense corneal leukoma.
- XF — Xerophthalmic fundus: A late manifestation — white, speckled depigmentation of the peripheral retina from rod photoreceptor degeneration.
Treatment of keratomalacia (WHO protocol): Vitamin A is given immediately — 200,000 IU (retinol equivalent) orally on day 1, repeated on day 2, and again at 2 weeks. For children under 1 year of age or weighing less than 8 kg, the dose is 100,000 IU. Intramuscular vitamin A palmitate is used if vomiting precludes oral administration. This vitamin A 'push' should be given before hospital investigation results — the clinical diagnosis is sufficient to initiate treatment. Concurrent nutritional support, treatment of precipitating infections (measles is the most common trigger that unmasks VAD), and topical antibiotic drops to prevent secondary corneal infection are given. Surgical management of the resultant scar (keratoplasty) is deferred until the nutritional status is restored and the eye is quiet.
Key prevention: India's National Vitamin A Supplementation Programme provides bi-annual high-dose vitamin A supplementation (100,000–200,000 IU) to children aged 6 months to 5 years through the Integrated Child Development Services (ICDS) network.
SELF-CHECK
A 3-year-old girl presents with night blindness and foamy whitish triangular deposits on the temporal conjunctiva of both eyes. Her corneas are clear. Which WHO xerophthalmia stage does she have, and which structures are involved?
A. X2 (corneal xerosis) — the cornea is involved with haziness beginning
B. X1B (Bitot's spots) — conjunctival lesions; the cornea is not yet involved
C. X3A (keratomalacia <1/3 cornea) — beginning corneal ulceration
D. XS (corneal scar) — healed scarring stage
Reveal Answer
Answer: B. X1B (Bitot's spots) — conjunctival lesions; the cornea is not yet involved
Bitot's spots (X1B) are foamy whitish deposits on the bulbar conjunctiva (temporal > nasal) — they are conjunctival lesions, not corneal. Clear corneas confirm that corneal involvement (X2 onwards) has not yet occurred. The night blindness indicates XN changes are also present, but the defining staging sign is the Bitot's spots. This patient needs urgent vitamin A supplementation to prevent progression to corneal xerosis (X2) and keratomalacia.