Page 26 of 33
OP4.9 | Corneal Foreign Body Identification and Simulated Removal — SDL Guide
Learning Objectives
- Identify a corneal foreign body and assess its depth and material using slit-lamp examination
- Perform a Seidel test to exclude corneal perforation
- Describe the instrument setup and technique for slit-lamp corneal foreign body removal
- Manage the rust ring from an iron or steel corneal foreign body
- Prescribe appropriate post-removal treatment and identify patients who require surgical referral
INSTRUCTIONS
Corneal foreign body (FB) removal is one of the most common minor ophthalmic procedures — performed at slit-lamps in emergency and outpatient departments across India daily. Done correctly, it is safe, quick, and provides immediate relief. Done incorrectly — too deeply, on a penetrating FB, or without excluding perforation — it can convert a minor injury into a medical emergency. This module teaches the skill using the OP-skills arc: indication and relevance, instrument principles, procedure technique, interpretation, and applied practice.
References
- Khurana AK. Comprehensive Ophthalmology, 7th ed. Ch 5: Diseases of the Cornea; Ch 16: Ocular Injuries (textbook)
- Parsons' Diseases of the Eye, 23rd ed. Ch 9: The Cornea; Ch 23: Injuries to the Eye (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 35-year-old mechanic presents at 5 PM to the emergency eye clinic with a painful, red, photophobic right eye. He was grinding metal without protective eyewear 6 hours ago. On examination, there is a small metallic-looking grey speck on the cornea at the 7 o'clock position, midway between the limbus and pupil. A brownish ring is visible around its edge — it has already begun to rust. He says, 'Doctor, just take it out quickly — I have to get back to work.' You have a slit-lamp, a topical anaesthetic, and a sterile 23-gauge needle. But first: is this truly a superficial FB, or has it penetrated into or through the cornea? Your decision on how to answer that question determines whether the next 10 minutes are routine or an emergency.
WHY THIS MATTERS
Corneal foreign body management is tested in final MBBS OSCE stations because it is a real-world skill that primary-care doctors, emergency physicians, and rural medical officers must be able to perform safely. The cost of getting it wrong — a perforated cornea from aggressive FB removal, or a fungal keratitis from a missed vegetative FB — is permanent vision loss. The cost of getting it right — a five-minute slit-lamp procedure with immediate pain relief — is immeasurably positive for the patient.
RECALL
From SDL 1: the corneal epithelium is 5–6 layers thick; the Bowman's layer is acellular and 8–14 µm thick; the stroma is ~90% of corneal thickness (~470–500 µm). A foreign body in the epithelium or Bowman's layer is superficial and safe to remove at slit-lamp; one in the mid-to-deep stroma requires caution; one that has penetrated through Descemet's is a surgical emergency. From SDL 3: vegetative (organic) foreign bodies carry Aspergillus and Fusarium spores — their removal does not eliminate the infection risk; monitor for fungal keratitis features (feathery margins, satellite lesions) for 2 weeks. From general principles: topical anaesthetics (proparacaine, benoxinate) are for PROCEDURAL use only — prescribing them for ongoing pain management is contraindicated because repeated instillation is toxic to the corneal epithelium.
Clinical Presentation and Initial Assessment of Corneal Foreign Body
Patients with corneal foreign bodies present with the classic triad of pain (foreign body sensation — worse on blinking because the eyelid moves over the sharp FB), lacrimation, and photophobia. In some cases — particularly when the FB entered the eye at high velocity (grinding, hammering metal) — the patient may be unaware of an FB and present only with eye pain. In children or in high-velocity injuries, the FB may have penetrated the cornea or the entire globe (intraocular FB) — a clinical scenario that must be excluded before ANY removal is attempted.
The initial assessment proceeds systematically:
Step 1 — History: Mechanism of injury (grinding/hammering metal → metal FB, high-velocity risk; gardening → vegetative FB, fungal risk; beach/dust → fine particulate, usually superficial). Use of protective eyewear. Time since injury. Whether the patient has used any eye drops (topical anaesthetic overuse? someone applied drops already?). Any prior eye disease or surgery.
Step 2 — Visual acuity (VA): Measure VA in both eyes BEFORE any procedure. If VA is significantly reduced (below 6/18) in an otherwise healthy eye, consider that the FB may be more extensive than anticipated (deep stromal, causing oedema) or that there is an intraocular component.
Step 3 — Torch and slit-lamp survey: Examine the lids, conjunctiva (for concomitant conjunctival FBs or lacerations), and the entire corneal surface. The FB appears as a grey-white, metallic, brownish, or translucent particle on the corneal surface. An iron/steel FB may already have a brownish rust ring within hours.
Step 4 — Seidel test (to exclude perforation): Apply a strip of fluorescein paper or a drop of 2% fluorescein to the area of the FB. In a dark room, examine under cobalt blue slit-lamp illumination. If aqueous is leaking through a corneal perforation, the fluorescein stream is diluted by the aqueous and appears as a brighter green rivulet streaming away from the FB site. A positive Seidel test = corneal perforation is present. Do NOT attempt FB removal at slit-lamp in this case — refer urgently for operative management.
Step 5 — Depth assessment: Using the slit-lamp with a narrow, bright optical section (the corneal illumination technique described in SDL 1): focus the beam on the FB and move it slowly from anterior to posterior to determine at what depth the FB is located — superficial (in or just below the epithelium), mid-stromal, or deep stromal. Only superficial FBs should be removed at slit-lamp.
Instrument and Equipment Principles for FB Removal
Safe corneal FB removal at the slit-lamp requires specific instruments and an understanding of how they interact with the corneal anatomy.
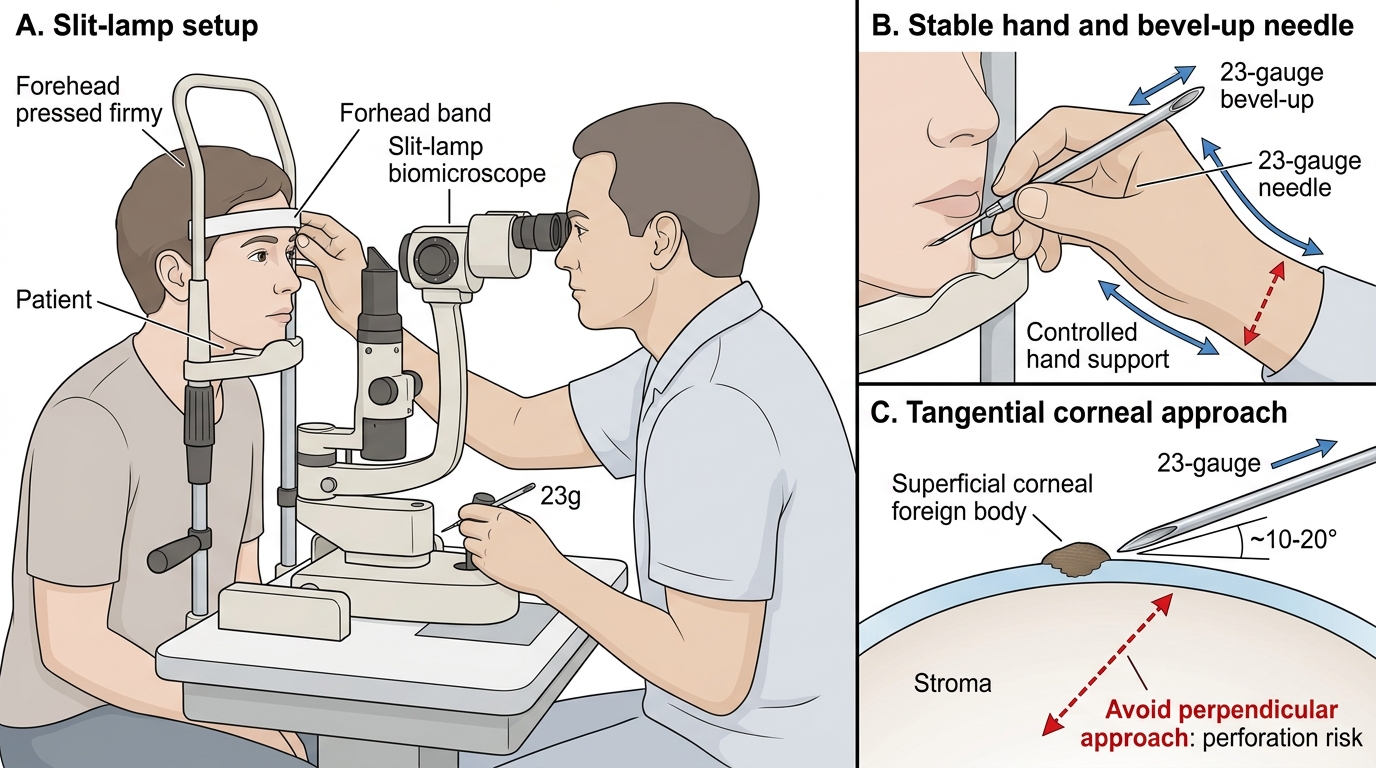
Slit-lamp: The instrument provides the magnification (typically ×16–×25) and focal illumination required to work precisely on the corneal surface. The patient is seated at the slit-lamp with the chin in the chin rest and the forehead against the forehead band. The examiner sits on the opposite side. Good patient cooperation is essential for a slit-lamp FB removal — a sudden movement of the head could push the needle deeper into the cornea. Some surgeons use an assistant to hold a topical anaesthetic-soaked cotton bud on the conjunctiva as a reminder to the patient not to move.
Topical anaesthesia: Proparacaine 0.5% (also called proxymethacaine) or benoxinate (oxybuprocaine) 0.4% eye drops are instilled into the conjunctival sac 1–2 minutes before the procedure. One or two drops are sufficient. The patient may still feel pressure but not sharp pain. Critical safety rule: topical anaesthetics are for PROCEDURAL use only — they must NEVER be prescribed for the patient to take home and use for ongoing pain management. Repeated self-application masks the normal pain warning signals (pain indicates healing is incomplete, or infection is developing) and is directly toxic to corneal epithelial cells, causing neurotrophic-like keratopathy.
Removal instruments:
- 23–26 gauge hypodermic needle (sterile, single-use): The standard instrument for slit-lamp FB removal. The bevel (the angled cutting edge of the needle tip) is positioned facing upward (bevel-up). The needle is held in the dominant hand, approaching the cornea at a tangential angle (~15–30 degrees) parallel to the corneal surface — this minimises the risk of inadvertent deep penetration if the patient moves or the surgeon's hand slips. The FB is engaged with the tip of the needle and lifted or flicked off the surface.
- Corneal FB spud: A spatula-shaped instrument specifically designed for FB removal; provides more control for very flat, adherent particles.
- Alger brush (rust ring burr): A low-speed motorised burr attachment for slit-lamp use, specifically designed to debride rust rings from iron FBs. Applied gently to the rust-stained area to mechanically remove the iron oxide deposits.
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
Slit-Lamp Corneal Foreign Body Removal Setup
SELF-CHECK
During corneal foreign body removal at the slit-lamp, a patient asks to take home the topical anaesthetic drops you used for the procedure to manage the pain that evening. What is the correct response and reasoning?
A. Prescribe one bottle of proparacaine 0.5% for home use; the pain will last only one day so toxicity is not a concern
B. Topical anaesthetics must not be prescribed for home use; they are toxic to the corneal epithelium with repeated use, mask warning pain signals, and delay healing. Prescribe antibiotic drops and oral analgesics instead
C. Prescribe benoxinate 0.4% for a single dose at bedtime only; one further dose is safe
D. Topical anaesthetics are safe for 48-hour home use after minor procedures
Reveal Answer
Answer: B. Topical anaesthetics must not be prescribed for home use; they are toxic to the corneal epithelium with repeated use, mask warning pain signals, and delay healing. Prescribe antibiotic drops and oral analgesics instead
Topical anaesthetics — proparacaine, benoxinate — are contraindicated for home use. Repeated instillation is directly toxic to corneal epithelial cells, causing a neurotrophic-like keratopathy that can result in severe, non-healing corneal ulceration. Additionally, anaesthetising the cornea masks the pain that serves as a warning sign of infection or incomplete healing. The correct post-removal analgesia is oral analgesics (paracetamol, NSAID), topical antibiotic drops to prevent infection, and cycloplegics for ciliary spasm pain.
Procedure and Technique for Corneal FB Removal
The procedure for slit-lamp corneal FB removal follows a consistent sequence that maximises safety and minimises the risk of iatrogenic injury. This description assumes a superficial metallic FB — the most common scenario.
Preparation: Instil topical anaesthetic (proparacaine 0.5% × 2 drops) into the conjunctival sac. Wait 1–2 minutes for full effect. Explain the procedure to the patient: 'I am going to use a thin needle to lift the metal particle off your eye. You may feel pressure but not pain. It is very important that you keep your head still — tell me if you need to move or cough, and I will take the needle away first. Please fix your gaze on the fixation light.'
Slit-lamp setup: High magnification (×16–×25), narrow bright slit beam focused on the FB. Good co-axial illumination.
FB removal:
1. Approach the cornea with the sterile 23-gauge needle bevel facing upward at a tangential angle (approximately 15–30 degrees to the corneal surface — nearly parallel, not perpendicular).
2. Engage the leading edge of the FB with the needle tip.
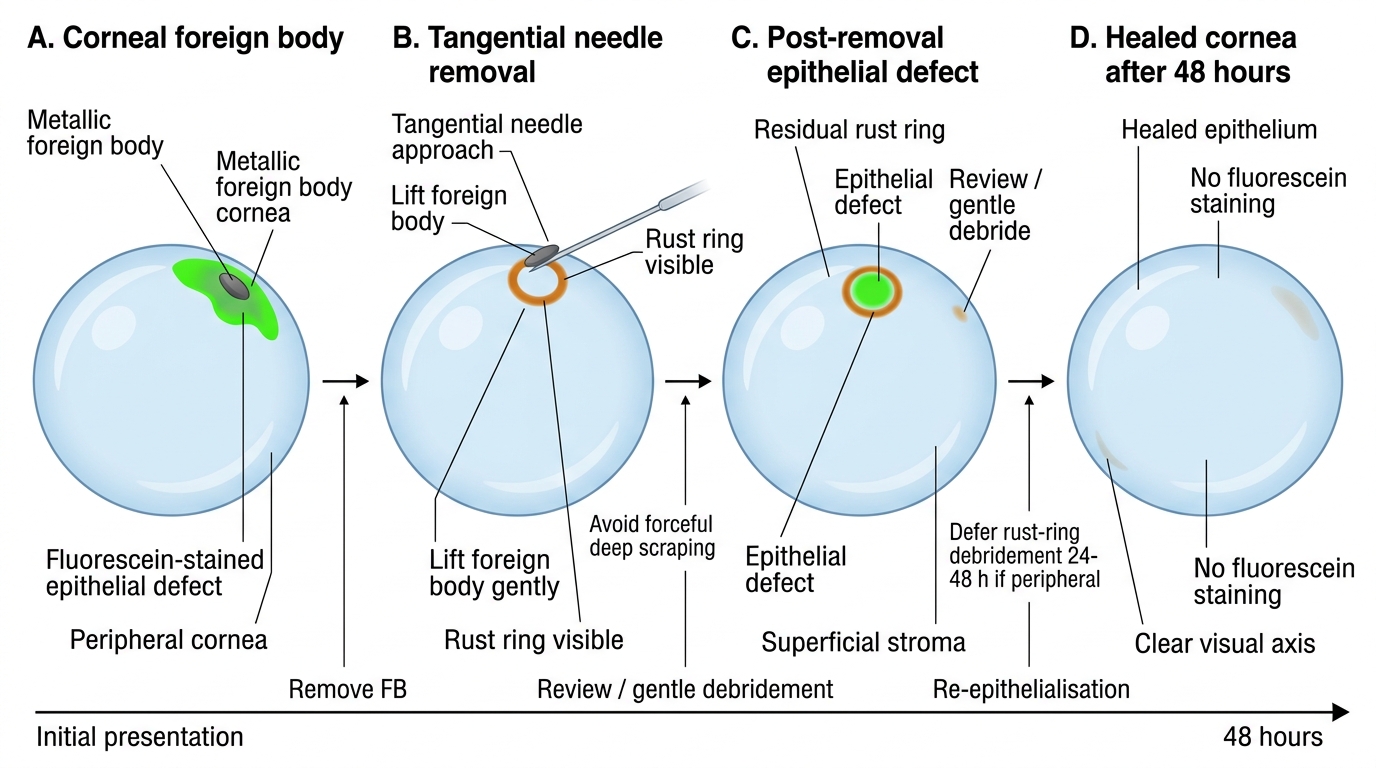
3. Use a gentle scooping or flicking motion to dislodge the FB from the stroma. The goal is to lift it toward the slit-lamp side (anteriorly) and off the surface.
4. If the FB does not lift with gentle attempts, do not increase force. A FB that requires excessive force to remove is either deeper than estimated, or has been there long enough to have epithelialised over it (the epithelium has grown over the FB — sometimes requiring a small epithelial flap to be raised before the FB can be engaged).
5. Remove only superficial material. If the FB is deep (visible posterior stroma on optical section), stop and refer.
Rust ring management: If an iron/steel FB leaves a rust ring after removal, the rust ring may be addressed at the same sitting or deferred. The ideal approach is to wait 24–48 hours — allowing the rust to soften (oxidation continues) and the surrounding tissue to soften slightly. At the follow-up visit, the rust ring is removed with an Alger brush (gentle motorised burr) or sequential needle debridement. A partial removal (removing the superficial rust, leaving a very deep rust ring) is acceptable at the first sitting — residual deep rust rings re-soften and can be approached in a second session. A small residual rust ring that is not on the visual axis is not a visual emergency.
Post-removal assessment: Apply fluorescein to visualise the epithelial defect size (a green staining area where the epithelium was removed with the FB). The defect should be smaller than or equal to the size of the FB. A very large staining area suggests that the FB was mobile and scraped the surface widely. Repeat the Seidel test if perforation is uncertain.
Corneal Foreign Body Removal and Rust Ring Management
SELF-CHECK
An iron FB has been removed from the cornea at the slit-lamp. A rust ring remains in the superficial stroma at the same site. The rust ring is 1 mm in diameter and not centrally located. What is the best approach to the rust ring?
A. Remove the rust ring completely at the same sitting using increasing force with the needle
B. Refer immediately for operative removal of the rust ring — slit-lamp removal is contraindicated
C. Leave it — rust rings are harmless and do not require treatment
D. Defer rust ring removal 24-48 hours; return the patient for gentle Alger brush or needle debridement when the ring has softened
Reveal Answer
Answer: D. Defer rust ring removal 24-48 hours; return the patient for gentle Alger brush or needle debridement when the ring has softened
Rust rings are best removed after 24-48 hours when the oxidised iron has softened, making debridement with an Alger brush (motorised burr) or sequential needle passes easier and less traumatic to the surrounding stroma. Attempting forceful removal at the first sitting risks deeper stromal injury. A peripheral rust ring is not a visual emergency. Complete removal at the first sitting is not necessary — a partial removal of the superficial rust followed by full removal at the next visit is acceptable and safer.