Page 12 of 33
OP4.4 | Corneal Opacity: Identification, Grading and Management — SDL Guide (Part 2)
Assessment and Investigation of Corneal Opacity
The pre-management assessment of corneal opacity is structured to answer three questions: How deep is the opacity? Is the endothelium healthy? Is the rest of the visual pathway intact (i.e., will a corneal graft restore vision)?
Slit-lamp biomicroscopy: The optical section of the slit-lamp accurately localises the opacity depth. A high-magnification narrow slit beam is focused on the cornea and moved slowly from anterior to posterior — the observer can see at which depth the scar begins and ends. Retroillumination and sclerotic scatter illuminate the overall extent.
Anterior segment OCT (AS-OCT): Provides a cross-sectional high-resolution scan of the cornea, enabling precise measurement of scar depth. This is essential before planning DALK (deep anterior lamellar keratoplasty) — if the scar extends to Descemet's membrane, DALK may not be possible and PK may be needed instead.
Specular microscopy: Assesses endothelial cell density and morphology. A cell count above 1,000–1,500 cells/mm² in the fellow eye (or the same eye if accessible) is reassuring for surgical planning. If the endothelium is too compromised, penetrating keratoplasty with healthy donor endothelium is required.
Visual acuity and pinhole test: VA measured before and after pinhole. A pinhole reduces the effect of refractive error by limiting light entry to the central optical axis — it will NOT improve VA caused by corneal opacity (organic cause). If VA improves substantially with pinhole, consider that refractive error (not scar alone) is contributing to the VA reduction — potentially treatable with spectacles/contact lenses without surgery.
Projection of light (PL) test: In a patient with very dense central leukoma, checking that the patient can perceive light and project it accurately in all four quadrants assesses rudimentary macular function. If projection is inaccurate or absent, there may be retinal or optic nerve disease that will limit the visual gain from keratoplasty.
B-scan ultrasonography: When the corneal opacity is too dense to see the fundus, B-scan assesses posterior segment integrity — vitreous, retina, choroid. Unexpected posterior pathology (retinal detachment, vitreous haemorrhage) would significantly change the surgical indication.
Management Modalities of Corneal Opacity
Management of corneal opacity is guided by the grade, depth, location, endothelial status, and patient factors (age, fellow eye, systemic health). The range of options extends from non-surgical optical rehabilitation to transplant surgery.
Provided image
Optical management: Spectacles or contact lenses address the refractive error and irregular astigmatism caused by corneal scarring. A hard (rigid gas-permeable) contact lens can neutralise irregular astigmatism by providing a smooth refractive surface — useful for nebulae and macula with irregular anterior surface.
Medical management: For superficial punctate keratitis and active surface disease causing haze, lubricants and treatment of the underlying cause may allow some spontaneous clearing. Topical steroids reduce active inflammatory haze (in appropriate conditions, after excluding infection).
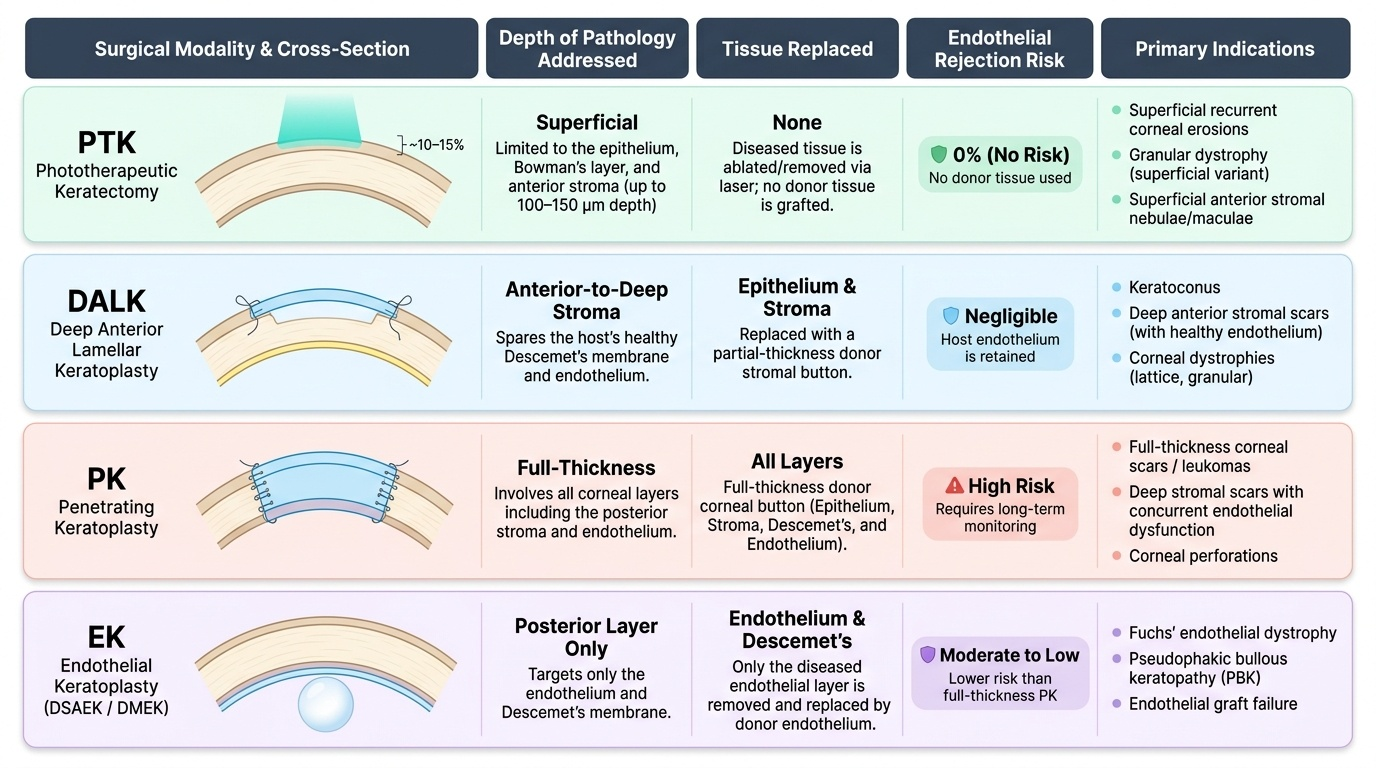
Phototherapeutic keratectomy (PTK): Excimer laser ablation of the anterior corneal surface — targets opacities in the epithelium, Bowman's layer, and anterior stroma (approximately up to 100–150 µm depth). PTK is effective for superficial recurrent corneal erosion syndromes, granular dystrophy, and anterior stromal nebulae/maculae. It cannot address mid or posterior stromal scars. The procedure is performed in a laser suite under topical anaesthesia.
Corneal tattooing: In blind, cosmetically disfiguring leucomatous eyes (where surgery is not an option or has failed), tattooing the white opacity with pigment (iron preparations or platinum chloride) improves cosmesis. It is a palliative procedure and does not restore vision.
Deep anterior lamellar keratoplasty (DALK): The surgeon removes the host epithelium and stroma down to (but not including) Descemet's membrane, preserving the host endothelium. Donor stroma is sutured in place. The advantage over PK is that the host endothelium is retained — eliminating endothelial rejection risk, and allowing the transplant to last longer. Indication: anterior stromal opacity (nebula/macula/leukoma) with healthy endothelium — keratoconus, anterior stromal scars from fungal/bacterial ulcers, corneal dystrophies (granular, lattice).
Penetrating keratoplasty (PK): Full-thickness replacement of the entire cornea, including Descemet's membrane and endothelium, with a full-thickness donor button. Required when the opacity involves the posterior stroma/Descemet's/endothelium (e.g., adherent leukoma with iris involvement, Fuchs' endothelial dystrophy with full stromal oedema, failed DALK). The risk of endothelial rejection (requiring lifelong immunosuppression with topical steroids) is higher than for DALK.
Endothelial keratoplasty (DSEK — Descemet's stripping endothelial keratoplasty; DMEK — Descemet's membrane endothelial keratoplasty): Replaces ONLY the endothelium and Descemet's membrane via a small incision, leaving the host stroma intact. Indicated for endothelial failure without significant stromal opacity — Fuchs' endothelial dystrophy, pseudophakic bullous keratopathy. Faster visual recovery and lower rejection rates than PK.
| Procedure | Tissue addressed | Depth | Endothelial rejection risk | Primary indication |
|---|---|---|---|---|
| PTK (excimer laser) | Epithelium/Bowman's/anterior stroma | ≤150 µm | None | Superficial nebulae/maculae, recurrent erosion |
| DALK | Epithelium + stroma (host endothelium preserved) | Full stroma to DM | Nil (own endothelium) | Anterior-mid stromal scars, keratoconus |
| PK (penetrating keratoplasty) | Full-thickness (all layers) | All layers | Yes (lifelong steroids needed) | Full-thickness opacity, adherent leukoma, Fuchs' + stroma |
| DSEK/DMEK | Descemet's + endothelium only | Posterior only | Lower than PK | Endothelial failure without stromal opacity |
CLINICAL PEARL
Before referring any patient with corneal opacity for keratoplasty, check the projection of light test: ask the patient to look straight ahead in a darkened room; shine a torch at the eye from four quadrants (temporal, nasal, superior, inferior) and ask 'which direction is the light coming from?' If they cannot accurately project light in all quadrants, there may be macular or optic nerve disease that will limit vision gain from corneal surgery. Offering keratoplasty to a patient with posterior segment disease is offering false hope and unnecessary risk. Always rule out the posterior segment — by B-scan if the cornea is too opaque for funduscopy.
SELF-CHECK
A 40-year-old woman has a dense central leukoma from old fungal keratitis. Specular microscopy of the same eye shows endothelial cell count of 1,800 cells/mm². AS-OCT confirms the scar extends through 80% of the stroma but appears to spare Descemet's membrane and the endothelium. Which keratoplasty technique is most appropriate?
A. DMEK (Descemet's membrane endothelial keratoplasty) because the endothelium is healthy
B. DALK (deep anterior lamellar keratoplasty) — removes stroma down to Descemet's, preserving the healthy endothelium
C. Penetrating keratoplasty (PK) because the scar is dense and deep
D. PTK (phototherapeutic keratectomy) because the scar is <150 µm deep
Reveal Answer
Answer: B. DALK (deep anterior lamellar keratoplasty) — removes stroma down to Descemet's, preserving the healthy endothelium
The scar involves 80% of stromal thickness but spares Descemet's membrane and the endothelium. Endothelial cell count is healthy (1,800 cells/mm²). DALK is the procedure of choice: it removes the scarred stroma while preserving the host's own healthy endothelium. This avoids endothelial rejection risk entirely. PK would be overkill — replacing healthy endothelium unnecessarily adds rejection risk. DMEK only replaces the endothelium, which is not the problem here. PTK only ablates up to ~150 µm and would not reach an 80%-depth scar.
Clinical Decision-Making: Selecting Management for Corneal Opacity
The management decision for corneal opacity follows a logical decision tree based on four parameters: depth of opacity, grade (nebula/macula/leukoma), location relative to visual axis, and endothelial health. Rather than memorising a list of modalities independently, the experienced clinician integrates these parameters in a structured sequence to arrive at the most appropriate intervention — or to determine that no intervention is currently warranted. The decision is not purely technical; it must account for the patient's age (amblyopia risk in children under 8 makes early intervention more urgent), fellow-eye status (if the fellow eye is normal, the functional deficit from a unilateral opacity is different from bilateral disease), and access to specialised care (DALK and endothelial keratoplasty require tertiary centres with experienced surgeons and eye-bank infrastructure, whereas optical rehabilitation with contact lenses can be initiated at a district hospital). Understanding the decision algorithm — not just the names of procedures — is what enables a clinician in any setting to make the right initial management choice and the right referral decision.
Step 1 — Is it affecting vision? Peripheral opacities may require no active intervention — reassure and advise annual review. Central or paracentral opacities on the visual axis are the surgical candidates.
Step 2 — What is the depth? Use slit-lamp optical section and AS-OCT:
- Anterior stroma only (≤150 µm) → PTK is an option if the patient has spectacle-uncorrectable vision and the opacity is superficial
- Mid to posterior stroma, Descemet's and endothelium spared, endothelium healthy → DALK
- Full-thickness stroma with Descemet's/endothelium involved, or adherent leukoma → PK
- Endothelium failed without significant stromal opacity → DSEK/DMEK
Step 3 — Is the endothelium healthy? Specular microscopy result:
- Count adequate (>1,000 cells/mm²), Descemet's spared → DALK preferred over PK
- Count very low or endothelium structurally damaged → PK (donor endothelium included)
Step 4 — Is the posterior segment normal? Confirm by projection test and B-scan. If posterior segment is diseased, defer or decline keratoplasty until posterior disease is addressed.
Step 5 — Consider age and amblyopia: In children <8 years, central corneal opacity threatens amblyopia — urgent optical rehabilitation and consideration of early keratoplasty even with the additional surgical challenges in a child. Amblyopia treatment (patching of the fellow eye) is essential concurrently.
Step 6 — Patient factors: General anaesthesia fitness, compliance for post-operative medication (topical steroids, cyclosporine), follow-up reliability, socioeconomic access to eye bank tissue.
Self-Assessment: Grading and Managing Corneal Opacity
Work through these decision scenarios:
Scenario 1: A 60-year-old man has bilateral corneal haziness. Slit-lamp shows diffuse greyish bilateral stromal oedema worse in the morning (worse on waking, improving through the day — because the closed eye at night cannot evaporate excess tear film, so the normal 'evaporative deturgescence' of night-time causes more oedema to accumulate). Specular microscopy: 410 cells/mm² bilaterally. Slit-lamp shows no focal opacity — diffuse haze. Diagnosis: Fuchs' endothelial dystrophy with decompensation. Management: hypertonic saline (5% NaCl) drops for mild cases; DSEK or DMEK for definitive treatment (replacing diseased endothelium).
Scenario 2: A 5-year-old child has a faint central corneal nebula following a resolved HSV keratitis episode. Her corrected VA is 6/36 in that eye. The slit-lamp shows the nebula is anterior — in the Bowman's/anterior stroma zone. Discuss management. Answer: The nebula is causing amblyopia in a visually critical period (< 8 years). Options: (1) PTK if the nebula is treatable by excimer laser ablation (anterior, small, measurable); (2) contact lens to neutralise the irregular astigmatism; (3) simultaneous amblyopia treatment (patching the fellow eye). Keratoplasty is a last resort in a child due to graft risks and compliance challenges.
Scenario 3: Grade the following opacities using the three-grade system and select the management: (a) faint corneal haze only visible on oblique illumination, 6/9 vision, peripheral — nebula, peripheral, likely no intervention; (b) white spot 3 mm, central, iris visible through it — macula, central, optical contact lens initially; if vision <6/18 and anterior stroma, consider PTK; (c) dense white opacity, no iris visible, prior penetrating trauma with corneal-iris adhesion — leukoma adherens, complex PK.