Page 14 of 33
OP4.5 | Dry Eye Disease — SDL Guide
Learning Objectives
- Describe the three-layer structure of the normal tear film and the source of each layer
- Enumerate the causes of dry eye disease and classify them as aqueous-deficient or evaporative
- Describe the clinical features and symptoms of dry eye disease including paradoxical reflex tearing
- Describe and interpret the Schirmer's test and tear film break-up time (TBUT)
- Outline a stepwise management plan for dry eye disease matched to its mechanism
INSTRUCTIONS
Dry eye disease (DED) is among the most prevalent ocular conditions in clinical practice globally, affecting an estimated 10–30% of adults over 40 years. It is chronic, often underdiagnosed, and significantly reduces quality of life. Understanding the tear film — and the distinct mechanisms by which it fails — transforms management from prescribing generic lubricants to targeted therapy. This module builds the pathophysiological framework for DED and applies it to clinical decision-making.
References
- Khurana AK. Comprehensive Ophthalmology, 7th ed. Ch 5: Diseases of the Cornea (textbook)
- Parsons' Diseases of the Eye, 23rd ed. Ch 9: The Cornea (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 38-year-old IT professional presents with a 6-month history of burning, gritty, tired eyes — worse in air-conditioned offices and after prolonged screen use. 'The strange thing,' she says, 'is that my eyes water constantly too — I look like I'm always crying.' Her optometrist prescribed lubricant drops but they only help for an hour. On examination there is mild conjunctival injection, TBUT of 6 seconds, and fine punctate fluorescein staining across the inferior cornea. Her Schirmer's test result: 14 mm at 5 minutes. The 'watering' and the dryness coexist. Why?
WHY THIS MATTERS
Dry eye disease is one of the top three presentations to any general ophthalmologist. It is also one of the most underserved — patients are often told 'just use lubricants' without an attempt to identify the mechanism or underlying cause. Severe DED (as in Sjögren's syndrome, Steven-Johnson syndrome aftermath, or severe chemical burns) can lead to corneal scarring and blindness. Recognising DED, testing it appropriately, and managing it by mechanism rather than symptom is a clinical competency that will serve you throughout your career.
RECALL
From SDL 1: the corneal epithelium carries microplicae and microvilli on its surface cells — these stabilise the tear film and anchor the mucin layer. Goblet cells of the conjunctival epithelium secrete mucin that wets the otherwise hydrophobic corneal epithelial surface. The meibomian glands in the tarsal plate of the eyelids secrete lipid (meibum) that forms the outer tear film layer preventing evaporation. From SDL 3: neurotrophic keratitis causes reduced blink reflex and trophic failure — both of which worsen dry eye by reducing tear distribution and epithelial renewal.
Clinical Presentation of Dry Eye Disease
Dry eye disease (DED) presents with a characteristic cluster of symptoms that may seem contradictory to the patient: ocular burning, gritty or foreign-body sensation (like sand in the eye), redness, blurring of vision (worse with sustained visual tasks, clearing on blinking — because blinking redistributes the unstable tear film), and paradoxical reflex tearing (excessive watering). The paradoxical tearing is the explanation the hook patient needed: when the tear film becomes unstable and the corneal surface is inadequately lubricated, pain and irritation stimulate the lacrimal reflex via the trigeminal nerve — causing copious reflex tear secretion by the lacrimal gland. This lacrimal reflex secretion is aqueous-rich but not a replacement for the stable mucin-anchored tear film; it quickly evaporates and the cycle repeats. The result is a patient who feels both dry and teary simultaneously.
Symptoms characteristically worsen with: prolonged screen use (reduced blink rate from ~15–20/min normally to as low as 5–7/min during concentrated visual tasks), air-conditioned or dry environments (increased evaporative loss), early morning on waking (evaporative accumulation during sleep with reduced blink), contact lens wear, and wind or smoke exposure. They typically improve with: blinking, eye closure, humid environments, and preservative-free lubricant drops.
Ocular signs on examination include: reduced tear meniscus height (the normally visible crescent of tear fluid at the lower eyelid margin is diminished or absent), conjunctival injection, mucus filaments or debris in the tear film, and corneal punctate epithelial erosions (staining with fluorescein as fine dots in the interpalpebral zone — the area of cornea exposed between the upper and lower eyelids). In severe cases, corneal filaments (strands of mucus anchored to the epithelium) or corneal staining extending outside the interpalpebral zone indicate more advanced disease.
Tear Film Structure and Normal Physiology
A stable, healthy tear film is the prerequisite for a clear optical surface over the cornea. The tear film is a thin (~7–10 µm total thickness) trilaminar structure coating the corneal and conjunctival epithelium with each blink.
The three layers, from outermost to innermost, are:
Lipid layer (~0.1 µm thick): secreted by the meibomian glands (modified sebaceous glands within the tarsal plates of both upper and lower eyelids, with approximately 25–30 glands per eyelid). The lipid (meibum) is spread across the tear film surface during blinking. Its primary function is to retard evaporation of the underlying aqueous layer. Without an adequate lipid layer, the aqueous evaporates rapidly — this is the mechanism of evaporative dry eye (EDE). The quality of meibum (whether it is liquid and freely expressed, or inspissated and obstructed) is therefore critical.
Aqueous layer (~7 µm thick, the bulk of the tear film): secreted primarily by the main lacrimal gland (located in the superolateral orbit) and supplemented by the accessory lacrimal glands of Krause (in the fornices) and Wolfring (at the upper lid margin). The aqueous layer carries dissolved proteins (lysozyme, lactoferrin, IgA — antimicrobial defence), growth factors (EGF supporting epithelial renewal), electrolytes, and oxygen for the avascular cornea. Failure or insufficiency of aqueous secretion is aqueous-deficient dry eye (ADDE).
Mucin layer (~1 µm thick, gel-like): secreted by goblet cells scattered throughout the conjunctival epithelium and by the stratified squamous surface cells of the cornea and conjunctiva (membrane-associated mucins MUC1, MUC4, MUC16). Mucins are hydrophilic glycoproteins that transform the normally hydrophobic epithelial surface into a wettable surface, allowing the aqueous layer to spread uniformly. Without adequate mucin, the aqueous beads up and distributes unevenly — causing localised drying. Goblet cell loss (from chemical burns, Stevens-Johnson syndrome, trachoma, vitamin A deficiency) causes a severe mucin-deficiency dry eye that is refractory to aqueous supplementation alone.
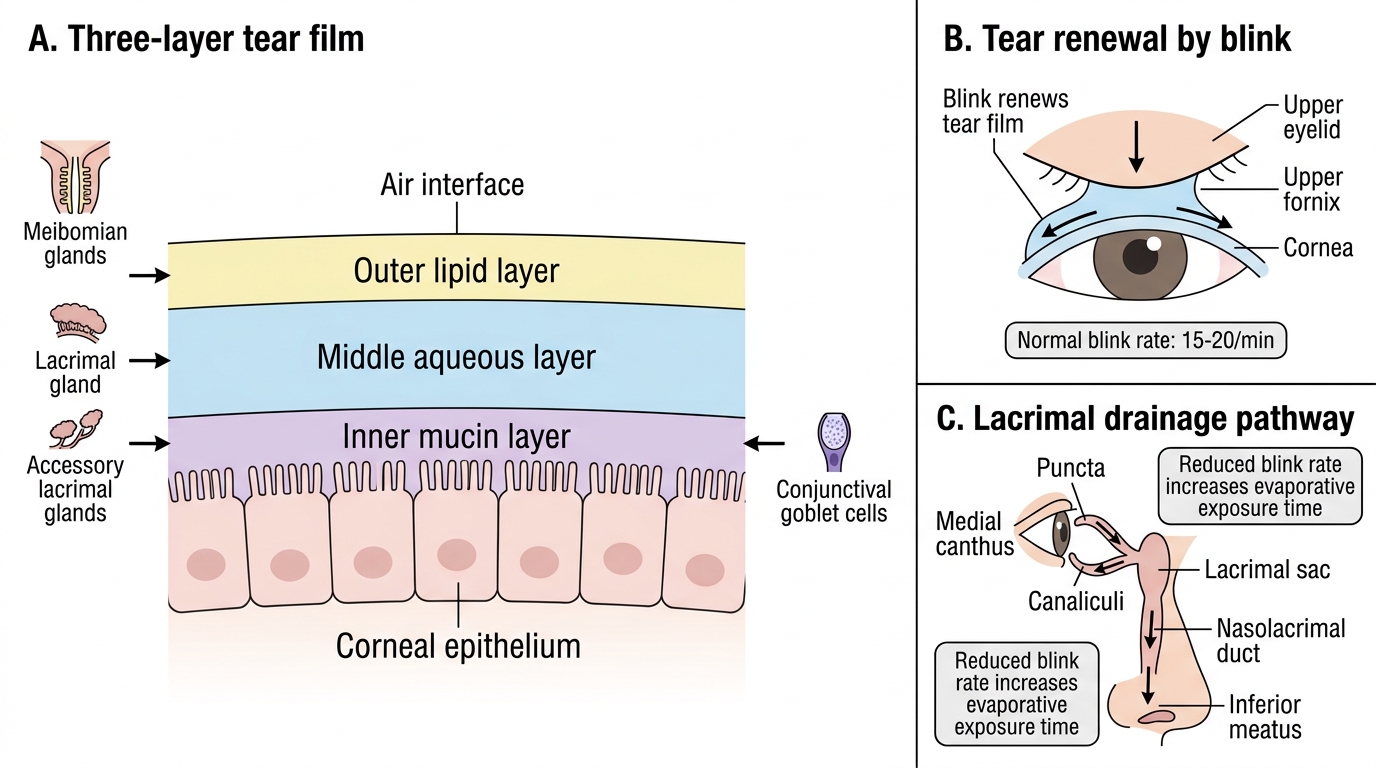
Three-Layer Tear Film: Sources, Renewal, and Drainage
The tear film is renewed with each blink — the upper eyelid sweeps new tear fluid from the upper fornix across the cornea, expelling old tears into the lacrimal drainage system (puncta → canaliculi → nasolacrimal duct → inferior meatus of the nose — hence tears cause nasal discharge). The blink rate (normally 15–20 per minute) is therefore a component of tear distribution; reduced blink rate increases evaporative exposure time.
SELF-CHECK
A 55-year-old woman has a 2-year history of severe dry eyes, dry mouth, and joint pains. Serological tests show positive anti-Ro (SSA) antibodies. Her Schirmer I test shows 2 mm wetting at 5 minutes bilaterally. Which mechanism of dry eye is most likely and what autoimmune diagnosis fits the clinical picture?
A. Evaporative dry eye due to meibomian gland dysfunction; no systemic disease
B. Aqueous-deficient dry eye due to primary Sjögren's syndrome (autoimmune destruction of lacrimal glands + salivary glands with anti-Ro/SSA antibodies)
C. Mucin-deficient dry eye due to conjunctival goblet cell loss from trachoma
D. Aqueous-deficient dry eye due to reduced blink rate from prolonged screen use
Reveal Answer
Answer: B. Aqueous-deficient dry eye due to primary Sjögren's syndrome (autoimmune destruction of lacrimal glands + salivary glands with anti-Ro/SSA antibodies)
The triad of dry eyes (keratoconjunctivitis sicca), dry mouth (xerostomia), and joint pains, combined with positive anti-Ro/SSA antibodies and Schirmer I wetting of only 2 mm (severely reduced, normal ≥10 mm), is diagnostic of primary Sjögren's syndrome — an autoimmune condition causing lymphocytic destruction of lacrimal and salivary glands. This is aqueous-deficient dry eye. Meibomian gland dysfunction causes evaporative dry eye, not the severe Schirmer's reduction seen here. Screen-related blink reduction would not cause anti-Ro positivity or Schirmer <5 mm.
Classification and Causes of Dry Eye Disease
The 2017 TFOS DEWS II (Dry Eye Workshop II) definition characterises DED as a multifactorial disease of the ocular surface characterised by a loss of homeostasis of the tear film — encompassing both symptoms and signs of tear film instability and hyperosmolarity, with inflammation and neurosensory abnormalities. The mechanistic classification divides DED into two non-exclusive categories.
Aqueous-deficient dry eye (ADDE) results from insufficient secretion of the aqueous tear film component by the lacrimal glands. Two main categories:
Sjögren's syndrome-associated ADDE: Primary Sjögren's syndrome = autoimmune lymphocytic infiltration and destruction of both lacrimal and salivary glands — presenting as keratoconjunctivitis sicca (KCS: dry eye) + xerostomia (dry mouth). Anti-Ro/SSA and anti-La/SSB antibodies are diagnostic. Secondary Sjögren's = the same glandular features occurring in the context of another autoimmune disease: rheumatoid arthritis (most common), SLE, scleroderma, primary biliary cholangitis.
Non-Sjögren's ADDE: Age-related lacrimal gland involution (physiological decline in aqueous output with age), lacrimal gland scarring from trachoma, Stevens-Johnson syndrome, chemical burns (alkali burns destroy goblet cells AND can scar lacrimal ductules), radiation, medication-induced (antihistamines, tricyclic antidepressants, beta-blockers, isotretinoin, oral contraceptives — all reduce aqueous secretion through diverse mechanisms).
Evaporative dry eye (EDE) occurs despite normal aqueous production — the tear film evaporates too rapidly due to lipid layer deficiency or prolonged exposure. Meibomian gland dysfunction (MGD) is the commonest cause of DED overall — inspissation or obstruction of meibomian glands reduces the quality and quantity of meibum, the lipid evaporation barrier. Other EDE causes: blepharitis (chronic lid margin inflammation → abnormal meibum quality), reduced blink rate (computer use, Parkinson's disease, neurotrophic states), lagophthalmos (incomplete lid closure from facial nerve palsy or proptosis — exposure keratopathy), contact lens wear (lens acts as a wick evaporating the tear film), and low-humidity environments.
In clinical practice, mixed-mechanism DED is extremely common — many patients have both reduced aqueous production and rapid evaporation. Sjögren's patients often develop secondary MGD from chronic lid margin inflammation.