Page 23 of 33
OP4.{8,10} | Eye Donation, Eye Banking and Deceased Eye Preservation Counselling — SDL Guide
Learning Objectives
- Describe the importance of eye donation and eye banking in addressing corneal blindness
- Enumerate the protocols involved in eye donation and eye banking from consent through to distribution
- Describe the corneal preservation media (McCarey-Kaufman medium, Optisol-GS, organ culture) and their storage parameters
- Enumerate the eligibility criteria and contraindications to eye donation
- Counsel patients and their family in a simulated environment about eye donation, addressing common myths and explaining how to preserve the eye of the deceased until enucleation
INSTRUCTIONS
Every year, thousands of people in India who are blind from corneal disease could have their sight restored by keratoplasty — if only there were enough donor corneas. There are not. The gap between corneal need and supply is driven partly by ignorance, partly by myth, and partly by the failure of doctors to counsel families at the moment when donation is possible. This module teaches you the clinical and communication skills to change that outcome — a competency explicitly examined in the MBBS final and one that will affect real patients throughout your career.
References
- Khurana AK. Comprehensive Ophthalmology, 7th ed. Ch 5: Diseases of the Cornea; Appendix: Eye Donation (textbook)
- Parsons' Diseases of the Eye, 23rd ed. Ch 9: The Cornea (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 52-year-old man has just been declared brain-dead in the ICU of your hospital following a road traffic accident. His 28-year-old son — the only family member present — is distraught. The eye bank coordinator approaches you: 'Doctor, can you help us talk to the family? He's a potential donor — his corneas could give sight to two people waiting for keratoplasty.' You have 10 minutes before the family leaves for the night. You know that if you don't approach the family tonight, the donation window will close within hours. You must counsel — not pressure, not manipulate — in the most difficult moment of this family's life.
WHY THIS MATTERS
India requires approximately 150,000–200,000 corneal grafts per year. Its eye banks procure approximately 30,000–40,000 corneas annually — a supply gap of over 100,000. This means that for every person who receives a keratoplasty in India, three or four people who need one do not get one. The limiting factor is not surgical skill, not surgical facilities, not government will — it is voluntary eye donation. Every doctor who learns to counsel compassionately and accurately in the hours after a patient's death can directly change this statistic. This is perhaps the highest-impact public health action an ophthalmologist can take.
RECALL
From SDL 6: eye donation and eye banking are central to the treatment strategy for corneal blindness in India. From SDL 7: keratoplasty requires donor corneal tissue — the quality of the graft (endothelial cell count, preservation time) directly affects surgical outcomes. From microbiology: certain infectious diseases (HIV, hepatitis B/C, rabies, prion diseases such as CJD) can potentially be transmitted via corneal tissue — hence they are absolute contraindications to donation. Recall that CJD/prion proteins are not eliminated by standard sterilisation — hence the absolute exclusion.
Clinical Indication and Relevance of Eye Donation
Eye donation — the voluntary gift of the eyes (or specifically the corneas and other ocular tissues) of a deceased individual for the purpose of corneal transplantation, research, or training — is the only source of donor tissue for keratoplasty. Unlike blood transfusion or organ transplantation, eye donation involves corneas harvested from deceased donors; living individuals do not donate their corneas (a point of critical importance in public education and counselling, addressed below).
The clinical indication for eye donation is the need for corneal transplantation. As established in SDL 6 and SDL 7, keratoplasty restores vision in corneal blindness from post-infective leukoma, keratoconus, Fuchs' endothelial dystrophy, bullous keratopathy, and congenital anomalies. None of these patients can receive surgery without a donor cornea. The eye bank is the intermediary infrastructure that collects, evaluates, preserves, and distributes this tissue.
The scale of the problem in India is stark: an estimated 2 million people are waiting for keratoplasty in India. The supply of donor corneas falls far short of this demand. The gap has multiple causes: low public awareness of eye donation, myths and religious misconceptions, failure of hospital staff to approach donor families, cultural fear of post-mortem procedures, and inadequate hospital-based eye bank programs. Among these, the failure of doctors to initiate donation conversations is the most modifiable factor — and the most directly teachable clinical skill in this module.
India's eye donation landscape: the Eye Bank Association of India (EBAI) is the apex body; registered eye banks (approximately 750+) operate under the Transplantation of Human Organs Act (THOA) 1994 (amended 2011). The National Eye Donation Fortnight (August 25 – September 8) is an annual awareness campaign.
The Eye Banking Process: Consent, Retrieval and Evaluation
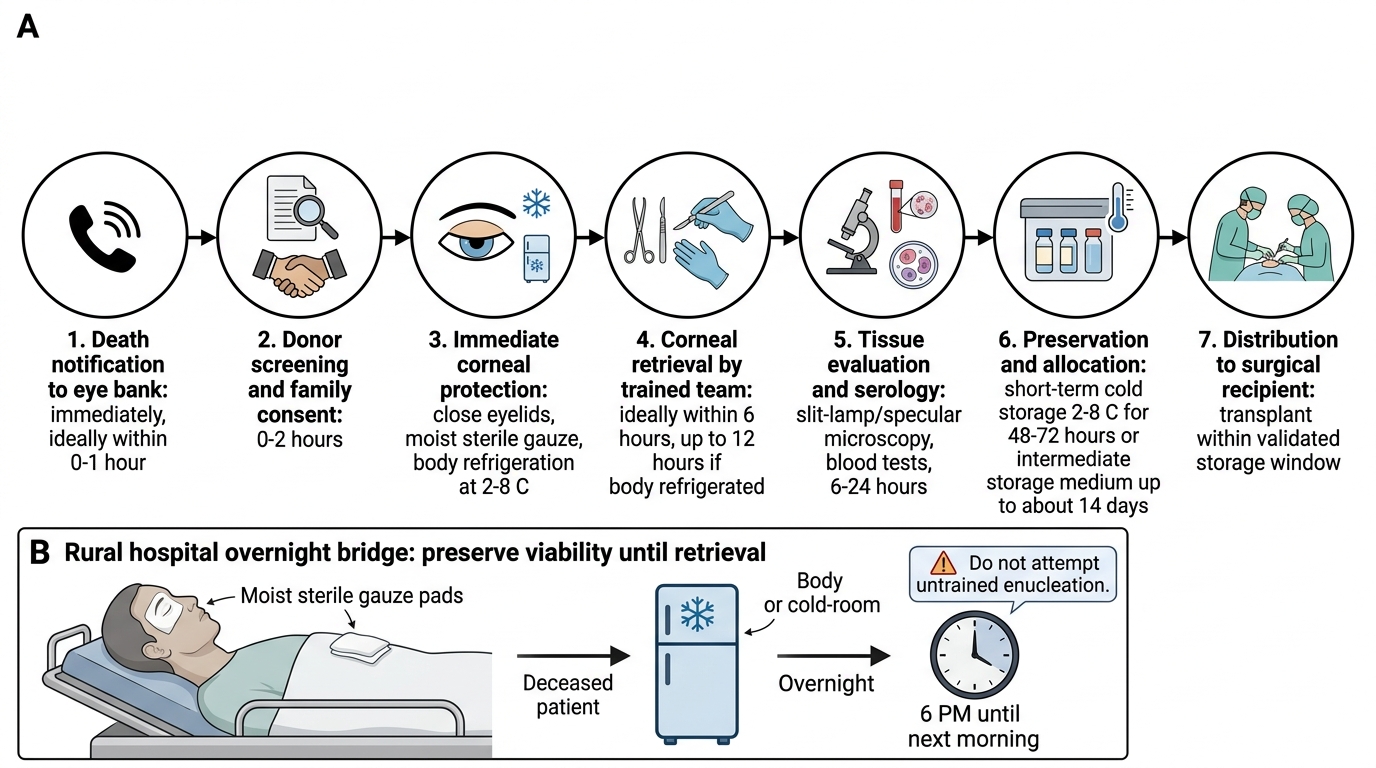
The eye banking process follows a defined sequence from the moment of death notification to the distribution of preserved tissue to a surgical recipient. Understanding each step allows the clinician to know when and how to intervene and counsel effectively.
Step 1 — Death notification and referral: When a patient dies in the hospital, the attending doctor or nurse notifies the eye bank coordinator. This must happen promptly — the window for viable corneal donation is approximately 6 hours from death (ideally; acceptable up to 12 hours, longer if the body is refrigerated). Eye banks typically have 24-hour helpline numbers for hospital referrals.
Step 2 — Consent: In India, donation requires written informed consent from the next-of-kin of the deceased donor. Consent cannot be given by the deceased in a will alone — family consent is legally required in practice. The counselling approach is critical: the conversation must occur within the narrow time window after death.
Step 3 — Immediate preservation: The eye bank coordinator visits the bedside and closes the deceased's eyelids; a moist chamber is created by placing moist sterile gauze pads over the closed eyelids, or by instilling antibiotic eye drops. This preserves the corneal epithelium and endothelium during the interval before retrieval.
Step 4 — Retrieval: Either enucleation (removal of the entire globe from the orbit) or corneoscleral rim excision (removal of the anterior segment including cornea with a rim of sclera, without the entire globe) is performed under aseptic conditions at the bedside or in a minor procedure room. Corneoscleral rim excision is now preferred by most eye banks — it is less disfiguring (prosthetic eyes are inserted) and technically simpler.
Step 5 — Evaluation of donor tissue: At the eye bank laboratory, the cornea is examined for: endothelial cell count and morphology (specular microscopy), presence of stromal opacity or scarring, epithelial integrity, and any contraindicated pathology. Serological testing of the donor's blood for HIV, hepatitis B surface antigen, hepatitis C, syphilis, and CMV is mandatory before the tissue can be cleared for transplantation.
Step 6 — Preservation and storage: Cleared tissue is placed in the appropriate preservation medium.
Step 7 — Distribution: Tissue is allocated to keratoplasty waiting-list patients, matched to urgency (therapeutic/tectonic > elective optical) and, in some systems, ABO blood group and tissue type (HLA matching is not routinely performed for corneal transplantation in most countries, unlike solid organ transplantation).
Eye Banking Process and Corneal Viability Timeline
SELF-CHECK
A patient dies in a rural hospital at 6 PM. No eye bank coordinator is available until the next morning. The doctor wants to preserve the deceased's corneas. What is the most important immediate step to maintain corneal viability until the eye bank team arrives?
A. Administer intravenous antibiotics to the deceased to prevent corneal infection
B. Refrigerate the entire body and place moist sterile gauze pads (moist chamber) over the closed eyelids to preserve corneal moisture and slow metabolic decline
C. Perform enucleation immediately without eye bank support using whatever surgical equipment is available
D. No action required — corneal cells survive 48 hours without intervention at room temperature
Reveal Answer
Answer: B. Refrigerate the entire body and place moist sterile gauze pads (moist chamber) over the closed eyelids to preserve corneal moisture and slow metabolic decline
Body refrigeration slows metabolic decline significantly, extending the viable donation window. Simultaneously, closed eyelids with moist sterile gauze pads (moist chamber) maintain corneal epithelial and endothelial viability. These two measures together can extend the viable window to allow morning retrieval. Enucleation without proper training and equipment should not be attempted outside the eye bank team. Corneal cells do NOT survive 48 hours at room temperature without intervention — the endothelium begins to deteriorate within hours of death at room temperature.
Corneal Preservation Media and Storage Protocols
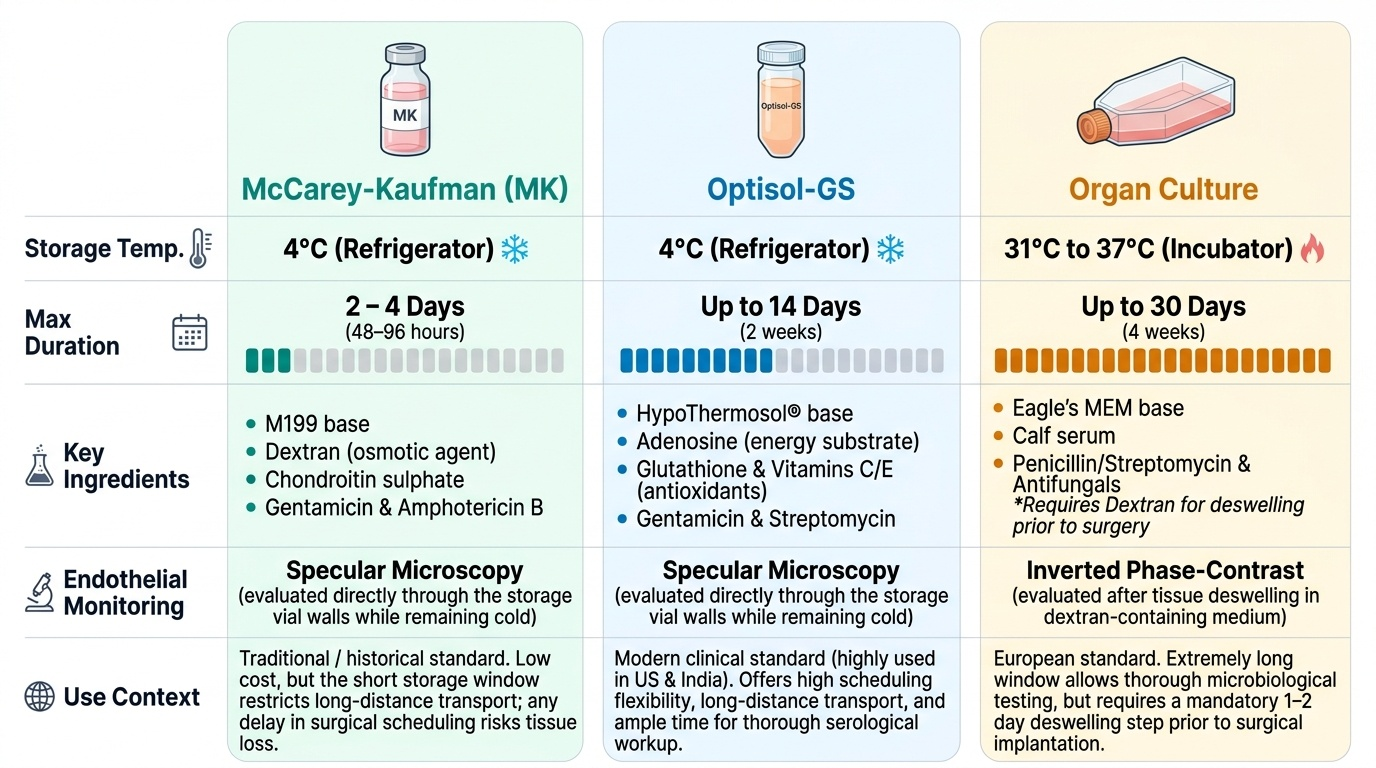
After retrieval, the corneoscleral rim is placed in a preservation medium that maintains endothelial cell viability during the interval between collection and surgical use. The choice of medium determines the maximum storage time and the ease of endothelial quality monitoring.
Provided image
McCarey-Kaufman (MK) medium is the traditional preservation medium developed in the 1970s by McCarey and Kaufman. It is a buffered tissue culture medium (M199) supplemented with dextran (to maintain osmolarity and prevent corneal swelling), chondroitin sulphate, gentamicin (antibacterial), and amphotericin B (antifungal). MK medium is stored at 4°C (refrigerator temperature) and maintains corneal viability for 48–96 hours (2–4 days). It was the standard for decades and is still used in settings where newer media are unavailable. Limitation: the short storage window means that any delay in surgical scheduling risks tissue loss.
Optisol-GS (Chiron Corporation, now Bausch & Lomb) is the current standard cold-storage medium in most of India's modern eye banks. It is based on a HypoThermosol® base supplemented with antioxidants (glutathione, vitamin E, vitamin C), energy substrates (adenosine), growth factors, gentamicin, and streptomycin. Stored at 4°C, Optisol-GS maintains corneal endothelial viability for up to 14 days. The extended storage window is a major practical advantage — it allows surgical scheduling flexibility, transport across distances, and time for thorough serological workup before tissue release. The majority of India's eye banks now use Optisol-GS or equivalent.
Organ culture medium is the standard preservation system in most European eye banks. The cornea is maintained in culture medium at 31–37°C (near body temperature) for up to 4 weeks. The advantage is the ability to monitor endothelial cell viability and morphology directly under light microscopy during storage, and to detect any contamination. The disadvantage is a higher infrastructure requirement (incubators, continuous monitoring) and higher cost. Before use, the cornea is typically transferred briefly to cold storage for transport.
| Medium | Temperature | Max duration | Principal use context |
|---|---|---|---|
| McCarey-Kaufman (MK) | 4°C | 48–96 hours | Short-term storage; limited-resource settings |
| Optisol-GS | 4°C | Up to 14 days | Standard in India; flexible scheduling |
| Organ culture | 31–37°C | Up to 4 weeks | European standard; extended viability monitoring |