Page 20 of 33
OP4.7 | Keratoplasty: Types and Indications — SDL Guide
Learning Objectives
- Enumerate the types of keratoplasty and the indications for each
- Describe the principles of DALK and explain why it avoids endothelial rejection
- Describe the technique and indications for endothelial keratoplasty (DSEK/DMEK)
- Describe penetrating keratoplasty and its specific indications
- Recognise the signs of graft rejection and describe the emergency management of endothelial rejection
INSTRUCTIONS
Keratoplasty — corneal transplantation — is the definitive surgical treatment for corneal blindness. Advances in surgical technique over the past two decades have transformed keratoplasty from a single operation (penetrating keratoplasty, replacing all five corneal layers) to a suite of targeted procedures replacing only the diseased layer. Understanding which procedure is appropriate for which clinical scenario is a core competency for the final-year MBBS student.
References
- Khurana AK. Comprehensive Ophthalmology, 7th ed. Ch 5: Diseases of the Cornea (textbook)
- Parsons' Diseases of the Eye, 23rd ed. Ch 9: The Cornea (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 25-year-old man with advanced keratoconus has been unable to tolerate contact lenses for the past year. His corrected VA with glasses is 6/60 in both eyes. His corneal specialist explains: 'We are going to remove just your scarred corneal stroma and replace it with a donor stroma — but we will keep your own endothelium in place. This means you won't have endothelial rejection.' Meanwhile, in the adjacent theatre, a 68-year-old woman with dense bilateral post-fungal leukoma involving the full corneal thickness undergoes a different procedure — full-thickness corneal transplantation — and is told she will need topical steroid eye drops for the rest of her life to prevent rejection. Same disease category (corneal blindness), same surgical principle (transplantation), very different operations and very different risks.
WHY THIS MATTERS
Keratoplasty is the most commonly performed tissue transplant in the world, with over 180,000 procedures performed annually. For the MBBS student, the value of understanding the types and indications is twofold: firstly, to counsel patients appropriately about what procedure they need and what complications to expect; secondly, because examinations consistently test the distinction between PK vs DALK vs DSEK — particularly the concept of endothelial rejection and the Khodadoust line. This module consolidates the transplant framework begun in SDL 4.
RECALL
From SDL 1: the five corneal layers (epithelium, Bowman's, stroma, Descemet's membrane, endothelium) and the fact that the endothelium is post-mitotic and cannot regenerate. From SDL 4: the management decision tree — anterior stromal disease with healthy endothelium → DALK; full-thickness disease → PK; endothelial failure without stromal opacity → DSEK/DMEK. From immunology: graft rejection involves T-lymphocyte-mediated immune recognition of donor HLA antigens expressed on donor tissue; the cornea is relatively 'immune-privileged' (lacks lymphatic drainage, blood vessels under normal conditions) but this privilege can be lost after corneal vascularisation.
Overview of Keratoplasty: Principles and Clinical Indications
Keratoplasty (corneal grafting, corneal transplantation) is the surgical replacement of diseased corneal tissue with healthy donor tissue from a deceased donor, processed and stored by an eye bank. It is the oldest and most successful form of solid tissue transplantation — the first successful penetrating keratoplasty was performed by Eduard Zirm in 1905. The immunological privilege of the cornea (due to avascularity and the absence of draining lymphatics under normal conditions) historically made keratoplasty the most successful transplant, but this privilege is lost once the host cornea becomes vascularised (as in healed infective keratitis or trachoma sequelae) — explaining why post-infective leukoma with corneal vessels has a worse graft prognosis than keratoconus.
Keratoplasty is classified by indication into four clinical categories:
- Optical keratoplasty: Performed to restore or improve visual acuity — the most common indication. Examples: post-infective leukoma (central corneal scar after fungal/bacterial keratitis), keratoconus (advanced), corneal dystrophies (Fuchs' endothelial dystrophy, granular dystrophy, lattice dystrophy), pseudophakic bullous keratopathy.
- Tectonic keratoplasty: Performed to restore the structural integrity of the globe rather than primarily for vision — when the cornea has thinned to the point of descemetocele or frank perforation. A tectonic PK 'patches' the globe and allows later optical correction once the eye is structurally sound.
- Therapeutic keratoplasty: Performed to remove an actively infected cornea (usually severe fungal keratitis) that has not responded to maximum medical therapy and is threatening perforation. The infected tissue is removed and replaced with healthy donor cornea, combined with systemic antifungals.
- Cosmetic keratoplasty: Performed in blind eyes with cosmetically unacceptable white corneas to improve the appearance of the eye, even when vision cannot be restored. Less commonly performed; donor tissue availability and graft risks must be carefully weighed.
Lamellar Keratoplasty: DALK and Endothelial Keratoplasty
The principle of lamellar keratoplasty is to replace only the diseased layer while preserving healthy host tissue. This targeted approach — enabled by advances in surgical technique and anterior segment OCT — reduces rejection risk, speeds recovery, and preserves precious host tissue.
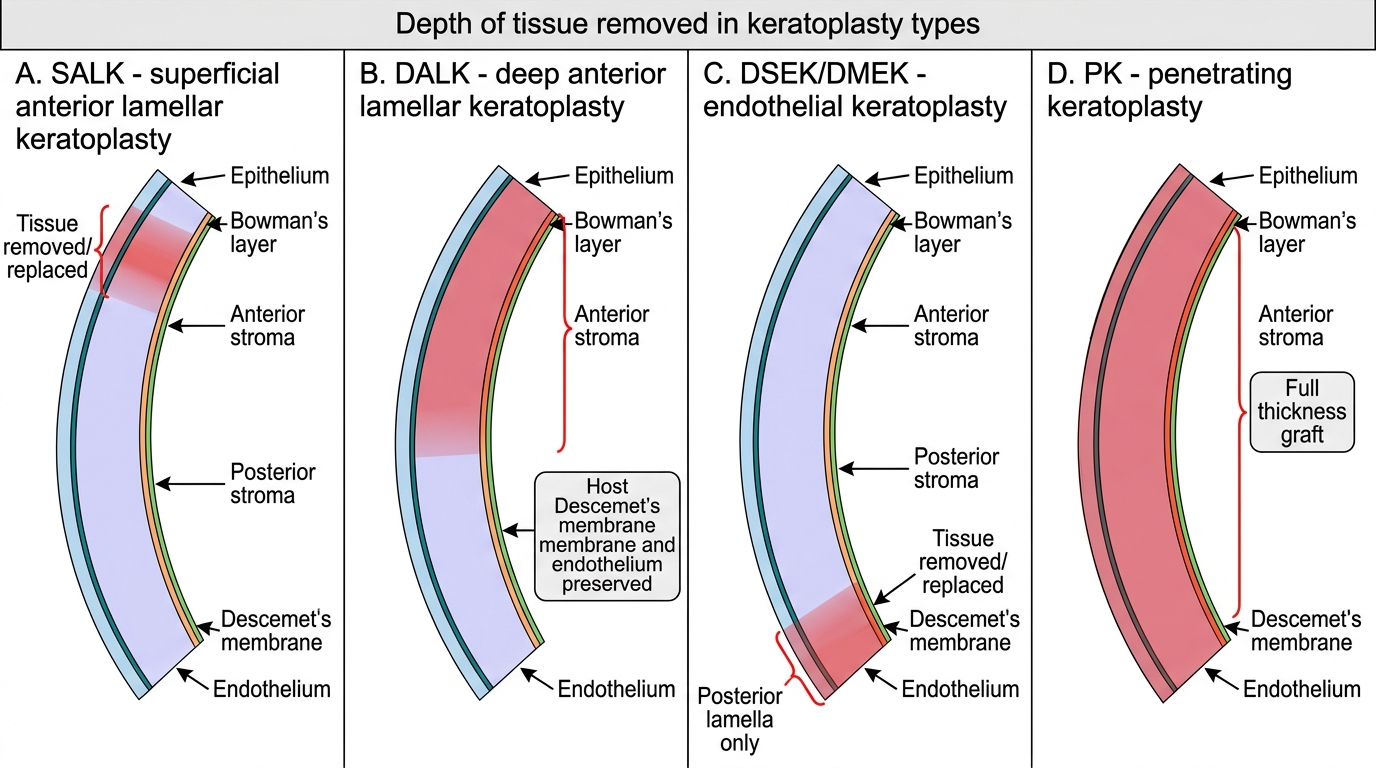
Deep Anterior Lamellar Keratoplasty (DALK) removes the host epithelium and stroma down to Descemet's membrane, leaving the host Descemet's membrane and endothelium in place. Healthy donor stroma (and epithelium) is sutured onto this preserved posterior surface. The Melles or big-bubble technique uses air injection into the stroma to dissect down to Descemet's membrane — the air creates a cleavage plane that allows surgical separation of stroma from Descemet's. The key advantage of DALK is that no endothelial tissue is transplanted — the patient retains their own endothelium. Without foreign endothelial cells, there is no risk of endothelial rejection — the most serious and sight-threatening form of graft rejection. DALK grafts therefore do not require lifelong topical steroid prophylaxis for endothelial rejection (though stromal rejection remains possible). Indications: keratoconus (the most common indication for DALK globally), anterior and mid-stromal scars from fungal/bacterial keratitis (if the scar spares Descemet's membrane), granular and lattice corneal dystrophies (which affect the stroma), and anterior macular opacities.
Superficial Anterior Lamellar Keratoplasty (SALK) replaces only the epithelium, Bowman's layer, and very superficial stroma — for conditions confined to these layers (recurrent corneal erosion dystrophies, very superficial PTK-unsuitable opacities). Technically simpler than DALK but applicable to fewer conditions.
Endothelial keratoplasty addresses the opposite end of the cornea — the endothelium only — while leaving the healthy host stroma in place. Two main techniques:
DSEK (Descemet's Stripping Endothelial Keratoplasty): The host Descemet's membrane and endothelium are stripped from the central posterior cornea; a thin lenticule of donor Descemet's + endothelium + a thin layer of posterior stroma is introduced through a small incision and unfolded against the posterior corneal surface, secured by an air bubble in the anterior chamber. The graft self-adheres within hours.
DMEK (Descemet's Membrane Endothelial Keratoplasty): Even more selective — only Descemet's membrane + endothelium is transplanted, with NO posterior stroma. Technically more demanding (the graft is very delicate and scrolls), but results in the fastest visual recovery and lowest rejection rate of any keratoplasty technique. Vision returns to near-normal within 1–3 months.
Both DSEK and DMEK are indicated for endothelial failure without significant stromal opacity: Fuchs' endothelial dystrophy (the prime indication — the most common condition for which DSEK/DMEK is performed in high-income countries), pseudophakic bullous keratopathy, and iridocorneal endothelial (ICE) syndrome.
Keratoplasty Types by Depth of Tissue Replacement
SELF-CHECK
A 30-year-old man with advanced keratoconus undergoes DALK. His surgeon tells him he will NOT need topical steroid eye drops lifelong for rejection prophylaxis. Why is this correct?
A. DALK is not a true transplant — the donor tissue does not contain living cells that can be rejected
B. DALK preserves the host's own Descemet's membrane and endothelium; since no donor endothelium is transplanted, there is no endothelial rejection risk
C. Topical steroids are not used after any keratoplasty — rejection is treated only if it occurs
D. Keratoconus corneas are immune-privileged so they do not reject any donor tissue
Reveal Answer
Answer: B. DALK preserves the host's own Descemet's membrane and endothelium; since no donor endothelium is transplanted, there is no endothelial rejection risk
DALK replaces the anterior and mid stroma while preserving the host Descemet's membrane and endothelium. No donor endothelial cells are transplanted. Endothelial rejection — the most serious form of graft rejection — requires foreign endothelial cells to trigger the immune response. Without transplanted donor endothelium, this risk does not exist. Note: stromal rejection (less serious) remains possible after DALK, but the lifelong prophylactic steroid requirement is driven by endothelial rejection prevention. PK patients do need lifelong topical steroid prophylaxis.
Penetrating Keratoplasty: Technique and Indications
Penetrating keratoplasty (PK) — the replacement of all five layers of the cornea with a full-thickness donor button — remains the procedure of choice when the pathology involves Descemet's membrane and the endothelium, or when advanced scarring makes lamellar dissection unsafe or impractical.
The surgical technique: Under general or local anaesthesia, the recipient cornea is trephined (a circular cutting instrument) to remove a button typically 7.5–8.5 mm in diameter, centred on the corneal apex. A same-sized or 0.25 mm oversized donor button is prepared from the donor eye (or preserved corneoscleral rim stored in the eye bank). The donor button is sutured into the host bed with 16 interrupted 10-0 nylon sutures, or a running suture, or a combination — the sutures are placed in a precise radially symmetric pattern to minimise induced astigmatism. At the end of the procedure, the anterior chamber is reformed with balanced salt solution. Sutures are typically removed selectively 12–18 months postoperatively once the graft is stable.
Indications for PK:
- Full-thickness corneal pathology where Descemet's membrane and endothelium are involved or uncertain — e.g., dense leukoma from healed fungal keratitis where scar depth extends to or through Descemet's
- Adherent leukoma (leukoma adherens) — the iris-cornea adhesion cannot be managed by lamellar surgery
- Failed DALK attempt — if Descemet's perforates during DALK surgery, conversion to PK is required intraoperatively
- Therapeutic keratoplasty for uncontrolled fungal keratitis with imminent perforation
- Some cases of keratoconus with corneal hydrops (acute oedema from Descemet's rupture) where DALK is no longer feasible
Rejection risk: Unlike DALK, PK transplants all five layers including the donor endothelium, which expresses MHC class II antigens recognised by host T-lymphocytes. Endothelial rejection can occur at any time — weeks to decades after surgery — and requires lifelong vigilance. Patients are maintained on long-term topical steroids (prednisolone 0.5% or fluorometholone 0.1% once or twice daily for years) to suppress rejection. In vascularised host corneas, systemic immunosuppression (mycophenolate, systemic steroids) may be added.