Page 2 of 13
OP5.1 | Episcleritis — SDL Guide (Part 2)
Classification of Episcleritis and Scleritis
The standard classification of episcleritis and scleritis is based on the landmark descriptive work of Watson and Hayreh (1976), which remains the foundation of clinical practice. This classification is not merely academic — each subtype carries distinct clinical implications for severity, systemic associations, and management.
Provided image
Clinically, the most important classification principle is that not all red, painful eyes carry equal risk: a simple episcleritis nodule and a necrotising scleral lesion may superficially resemble each other, yet their systemic implications, treatment requirements, and visual prognoses are poles apart. Recognising the specific subtype at the slit-lamp is therefore a gate-keeping decision — it determines whether the patient needs reassurance and lubricants or urgent systemic immunosuppression and rheumatological co-management. With that clinical weight in mind, the Watson & Hayreh classification divides these conditions as follows.
Episcleritis is classified into two forms:
1. Simple episcleritis — diffuse or sectoral bright-red injection of the episcleral vasculature. Bilateral in up to one-third of cases. Usually self-limiting (2-3 weeks). Recurrences common but each episode is benign.
2. Nodular episcleritis — a discrete, slightly raised, tender mobile nodule of inflamed episcleral tissue. More prolonged episodes and more frequent recurrences than simple episcleritis. Systemic associations slightly more common.
Scleritis is classified as anterior or posterior:
Anterior scleritis (90% of all scleritis) is subdivided by Watson & Hayreh into:
1. Diffuse anterior scleritis — most common form (40-45% of all scleritis); widespread, non-nodular scleral inflammation; moderate pain; usually responds to systemic NSAIDs.
2. Nodular anterior scleritis — a tender, immobile, hard scleral nodule; unlike episcleritis nodules, scleral nodules cannot be moved; moderate-to-severe pain.
3. Necrotising anterior scleritis WITH inflammation — the most severe form; intense pain; areas of avascularity and scleral necrosis; strong systemic associations (RA, GPA); risk of corneal melt and perforation.
4. Necrotising anterior scleritis WITHOUT inflammation (Scleromalacia perforans) — painless (a paradox for scleritis); found almost exclusively in long-standing severe RA, particularly women; grey avascular plaques form and the sclera thins progressively; may perforate without any acute inflammatory episode. The ABSENCE of pain and inflammation is a diagnostic trap.
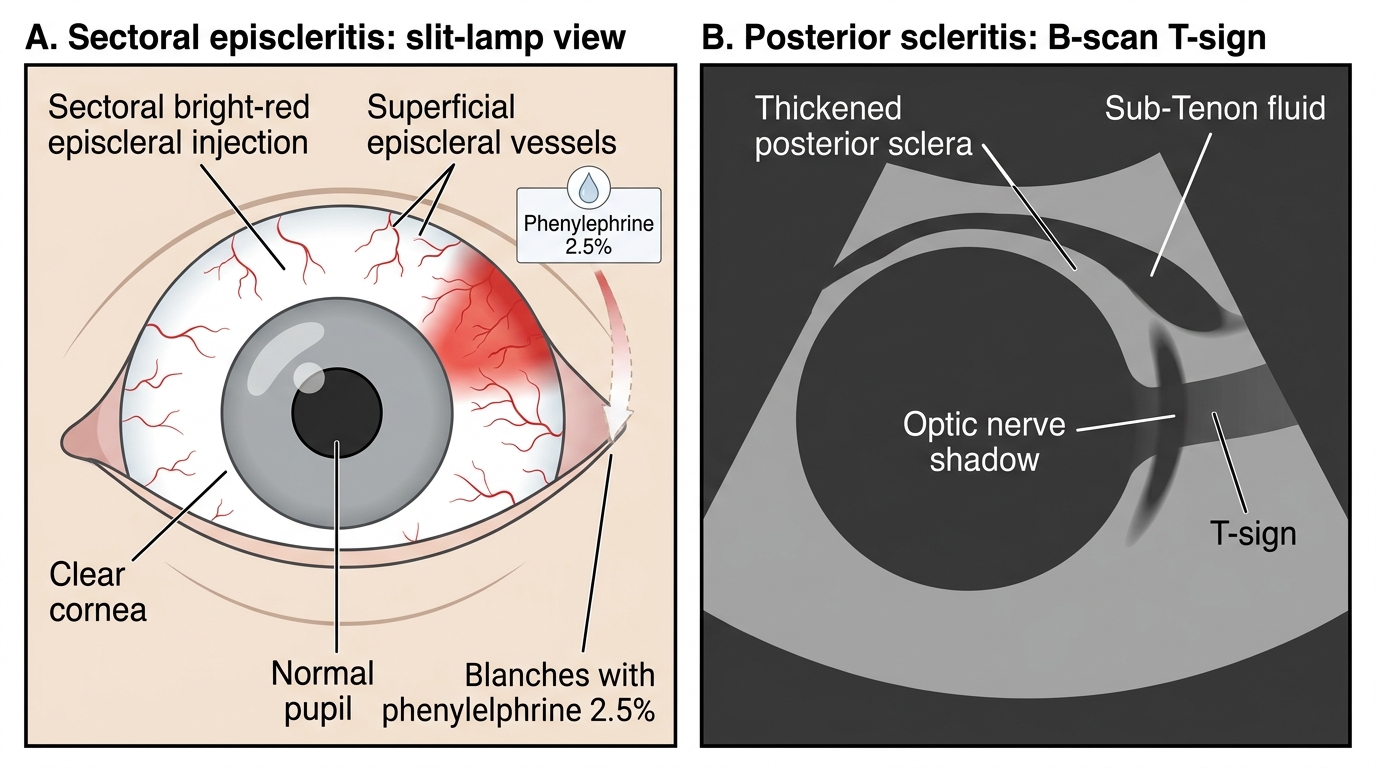
Posterior scleritis (10% of scleritis) — inflammation of the sclera posterior to the equator; often missed; presents with dull aching pain, restricted ocular motility, proptosis, disc oedema, exudative retinal detachment. Diagnosis by B-scan ultrasound showing characteristic T-sign (fluid in the sub-Tenon's space creating a T-shape at the optic nerve shadow).
Ocular Examination: Slit-Lamp, Phenylephrine Test, and Adjunct Investigations
The clinical examination of a patient with red eye suspected to be episcleritis or scleritis follows a systematic sequence that begins with careful external inspection and ends with targeted investigations when scleritis is confirmed.
External and penlight examination first establishes the pattern of redness: is it sectoral or diffuse? Is it superficial (bright red) or deep (violaceous)? Is there a nodule, and if so, can it be moved with a cotton tip? Is there any proptosis (posterior scleritis)? Tenderness on gentle palpation through the closed lid strongly suggests scleritis.
Slit-lamp biomicroscopy is the central examination tool. It allows assessment of: (a) the depth of vascular injection — episcleral vessels appear as a superficial, radially-oriented meshwork visible with diffuse illumination; scleral vessels are arranged in a deeper criss-crossing pattern; (b) the presence of anterior chamber flare or cells (which would suggest associated anterior uveitis, commoner in scleritis); (c) corneal involvement (peripheral ulcerative keratitis is a complication of scleritis, not episcleritis).
The Phenylephrine 2.5% Blanching Test is the single most important bedside test to distinguish episcleritis from scleritis. Phenylephrine is an alpha-1 adrenergic agonist that produces rapid vasoconstriction. At 2.5% concentration instilled into the conjunctival sac:
- In episcleritis: the superficial episcleral vessels constrict and blanch almost completely within 1-2 minutes, leaving a much whiter eye. The blanching is reliable and reproducible.
- In scleritis: the deep scleral vessels do NOT blanch with phenylephrine because they are embedded within a poorly-vascular, densely packed collagenous stroma that does not respond to topical vasoconstrictors.
Note: 10% phenylephrine is NOT used for this diagnostic test (it is used for mydriasis and carries cardiovascular risk in the elderly). The diagnostic test uses 2.5% phenylephrine only.
Adjunct investigations are not needed in pure episcleritis. When scleritis is confirmed, a systemic work-up must be initiated:
- Full blood count, ESR, CRP
- Rheumatoid factor, anti-CCP antibodies (for RA)
- ANCA (c-ANCA for GPA, p-ANCA for microscopic polyangiitis)
- ANA, anti-dsDNA (for SLE)
- Chest X-ray (for GPA — upper respiratory tract + lung involvement), sacroiliac X-ray (for ankylosing spondylitis)
- B-scan ultrasonography is essential when posterior scleritis is suspected: the T-sign (echo-free space between the optic nerve and posterior globe creating a T-shape on B-scan) is pathognomonic.
Episcleritis and Posterior Scleritis: Key Diagnostic Signs
Diagnosis and Differential Diagnosis
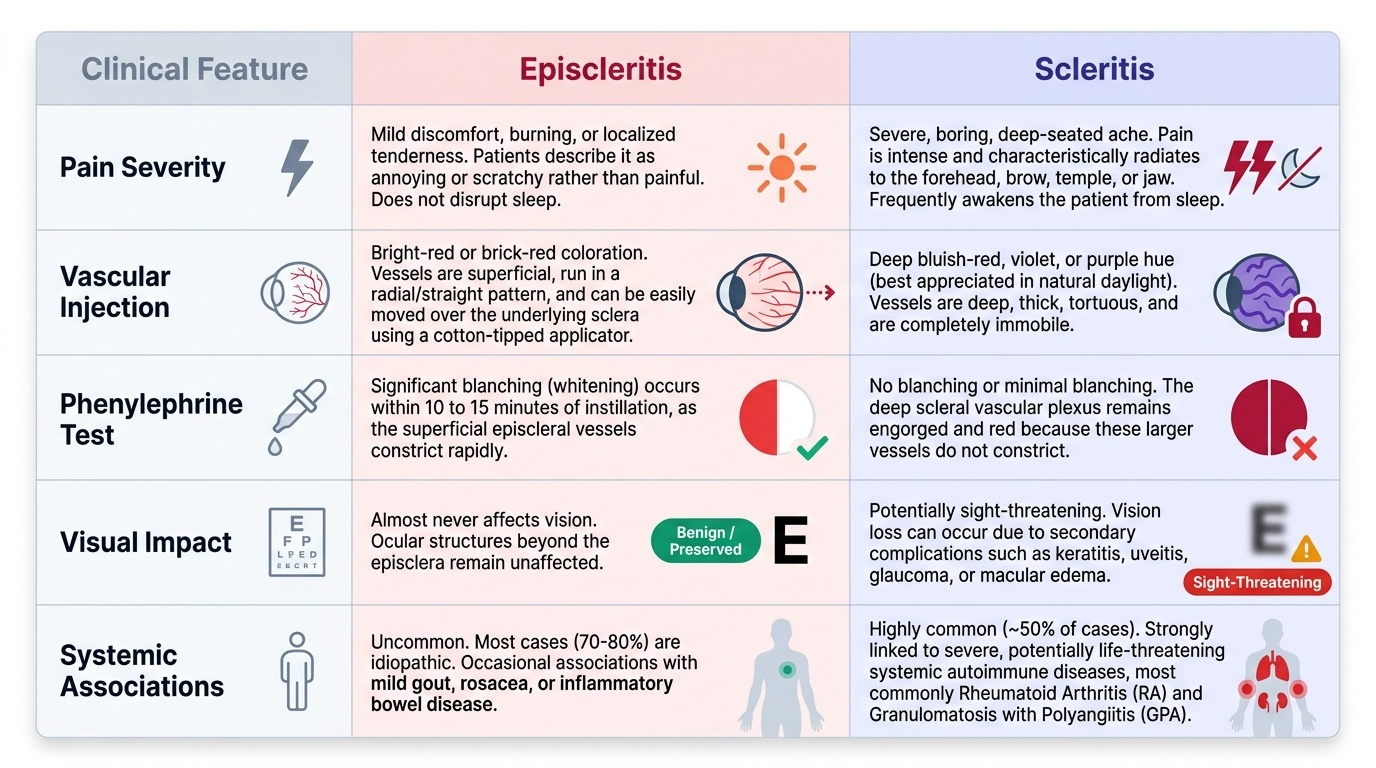
The diagnosis of episcleritis is clinical and rests on three criteria: (1) sectoral or diffuse episcleral injection with a characteristic bright-red colour; (2) mild-to-moderate discomfort without severe pain, photophobia, or visual loss; and (3) complete blanching of the injection with topical phenylephrine 2.5%. No investigations are required for straightforward episcleritis.
The diagnosis of scleritis rests on: (1) severe, boring pain with nocturnal worsening and tenderness on palpation; (2) deep, violaceous, non-blanching scleral injection; and (3) systemic associations in approximately half of cases. Posterior scleritis requires imaging (B-scan, T-sign).
The differential diagnosis of red eye relevant to this context must systematically exclude the sight-threatening causes — because the clinical and medicolegal consequence of missing acute angle-closure glaucoma or anterior uveitis in a patient labelled as 'simple episcleritis' is catastrophic. The following table anchors the key distinguishing features:
| Condition | Key distinguishing features |
|---|---|
| Episcleritis | Mild discomfort, sectoral bright-red injection, BLANCHES with phenylephrine 2.5%, vision normal |
| Scleritis | Severe boring pain, deep violaceous injection, does NOT blanch, may have systemic disease |
| Conjunctivitis | Discharge (mucopurulent, watery), diffuse injection, no pain, follicles/papillae on palpebral conjunctiva, vision normal |
| Acute Angle-Closure Glaucoma (AACG) | Severe pain, halos, reduced vision, fixed mid-dilated pupil, hard globe, IOP grossly elevated — EMERGENCY |
| Anterior Uveitis (Iridocyclitis) | Ciliary flush, photophobia, reduced vision, keratic precipitates, cells/flare in AC, miotic pupil |
| Microbial Keratitis | Corneal ulcer visible, discharge, reduced vision, hypopyon (bacterial) — SIGHT-THREATENING |
A useful clinical rule: any patient with a red eye and (a) severe pain, (b) reduced visual acuity, (c) photophobia, or (d) a fixed/irregular pupil requires urgent slit-lamp examination and IOP measurement to exclude AACG, anterior uveitis, and corneal pathology before a diagnosis of episcleritis is entertained.
CLINICAL PEARL
The phenylephrine 2.5% blanching test is your clinical shortcut at the slit-lamp: instil one drop, wait 60-90 seconds, and reassess. Episcleritis blanches completely — you can literally watch the redness fade. Scleritis does not blanch — the eye remains violaceous and injected. This single manoeuvre saves unnecessary systemic investigations in the vast majority of patients with red eye who have episcleritis. When you see a patient with a red eye and severe, boring, nocturnal pain — do NOT wait for the phenylephrine result to start your systemic work-up. That pain pattern alone mandates a slit-lamp, scleritis work-up, and referral.
SELF-CHECK
A 35-year-old woman presents with a 4-day history of redness and mild aching in the right eye. She has no discharge, vision is 6/6 in both eyes, and the redness is sectoral and bright red. One drop of phenylephrine 2.5% is instilled. After 90 seconds, the redness blanches almost completely. What is the most likely diagnosis?
A. Anterior scleritis
B. Episcleritis
C. Acute angle-closure glaucoma
D. Anterior uveitis
Reveal Answer
Answer: B. Episcleritis
Complete blanching with phenylephrine 2.5% is the hallmark of episcleritis. The superficial episcleral vessels are responsive to topical vasoconstrictors. Scleritis does NOT blanch. AACG and anterior uveitis would present with more severe symptoms (pain, reduced vision, photophobia).