Page 7 of 13
OP5.2 | Systemic Associations in Episcleritis/Scleritis Referral — SDL Guide (Part 3)
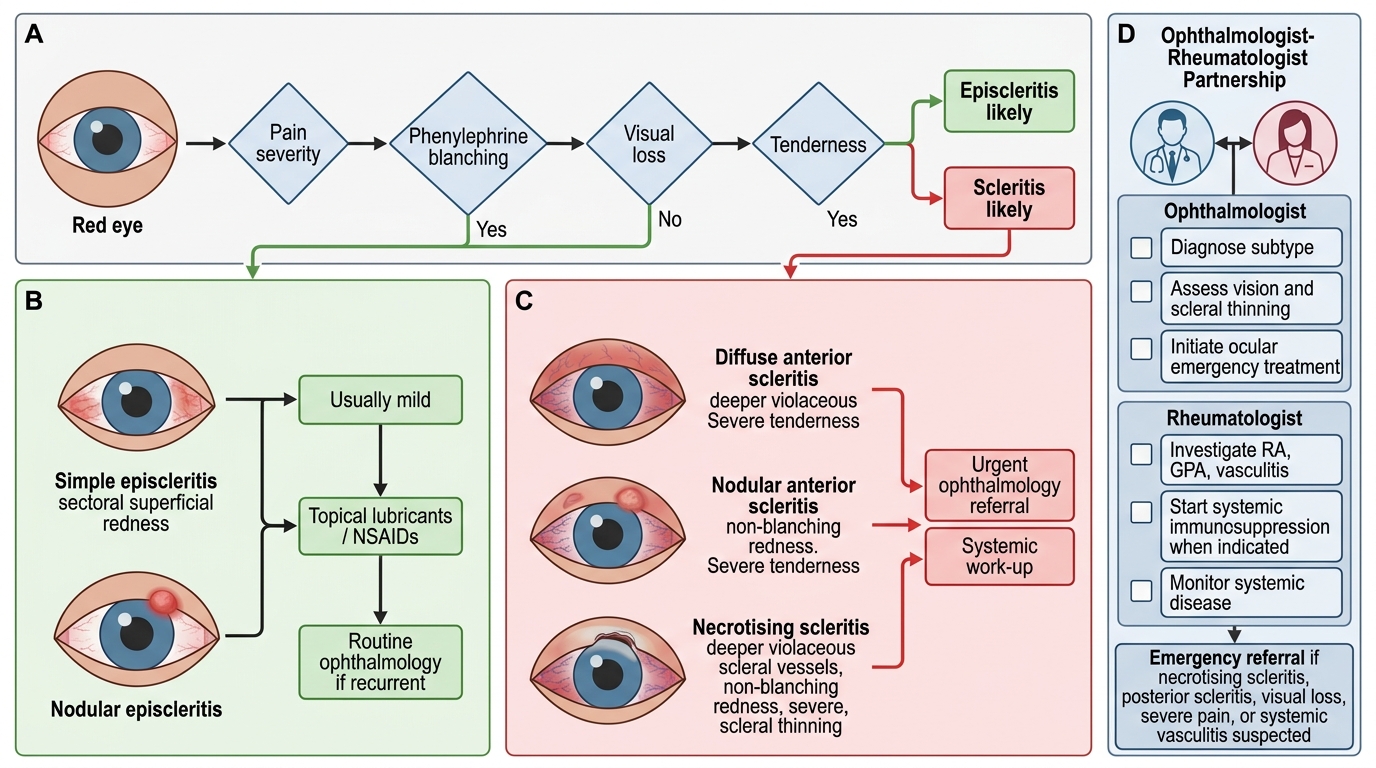
Diagnostic Algorithm: Red Eye to Referral Decision
The following clinical algorithm integrates the phenylephrine blanching test result, the scleritis subtype classification, and the systemic work-up findings into a structured referral decision. This algorithm is the practical summary of everything covered in OP5.1 and OP5.2 and represents the clinical workflow a junior doctor should be able to describe in an OSCE or explain to a patient. Algorithms of this type are frequently tested in postgraduate exit examinations because they represent the synthesis of diagnostic reasoning with management decision-making — a higher-order cognitive skill than recall alone. Follow each decision branch and ensure you can justify every step with a pathophysiological rationale, not merely as a memorised clinical rule.
Step 1: Red eye — is it episcleritis or scleritis?
- Perform phenylephrine 2.5% test
- Blanches completely → EPISCLERITIS → go to Step 2A
- Does NOT blanch → SCLERITIS → go to Step 2B
Step 2A: Episcleritis pathway:
- First episode, uncomplicated, young patient, no systemic symptoms → conservative management (lubricants, topical NSAIDs); review in 2-3 weeks; no investigation needed
- Recurrent, bilateral, or systemic symptoms present → targeted investigation (ESR, CRP, serum uric acid, RF if RA suspected; FBC + CRP if IBD suspected) → refer to appropriate specialist based on findings
Step 2B: Scleritis pathway:
- Classify subtype: diffuse / nodular / necrotising / posterior
- Order the full investigative panel: FBC, ESR, CRP, RF, anti-CCP, ANA, anti-dsDNA, c-ANCA, p-ANCA, CXR, urine analysis ± B-scan
- Start systemic NSAIDs (first-line for diffuse/nodular); refer ALL to rheumatology
- If necrotising or PUK or haematuria/renal impairment → URGENT referral (24-48 hours)
- If c-ANCA positive with pulmonary or renal involvement → EMERGENCY admission
Step 3: Monitor and co-manage:
- Ophthalmologist monitors ocular disease (slit-lamp, IOP, corneal integrity, VA)
- Rheumatologist titrates systemic immunosuppression
- Review scleritis activity jointly; dose reduction based on both ocular and systemic control
Red Eye Algorithm: Episcleritis vs Scleritis Referral Pathway
Management at the Interface: The Ophthalmologist-Rheumatologist Partnership
The management of scleritis-associated systemic disease requires a structured partnership between the ophthalmologist and rheumatologist (and other specialists as appropriate), because neither alone can manage the full complexity of these patients. Understanding the division of responsibilities, the shared language of disease activity, and the thresholds for escalation is essential for effective clinical communication between specialties. In practice, the ophthalmologist initiates the diagnosis and emergency management of the acute scleral inflammation, while the rheumatologist investigates and manages the underlying systemic autoimmune disease. Neither can function optimally without the other: an ophthalmologist who treats necrotising scleritis with topical steroids alone — without addressing the underlying GPA — risks progressive scleral destruction and systemic vasculitic crisis; a rheumatologist who controls the RA systemically but fails to refer the patient for ophthalmic surveillance may miss the development of scleromalacia perforans until globe perforation is imminent.
The ophthalmologist's role:
- Diagnose and classify the scleritis subtype
- Initiate appropriate topical/systemic ocular therapy (lubricants; oral NSAIDs as first-line; periocular Tenon's capsule steroid injection for localised disease; topical steroids for associated anterior uveitis)
- Monitor ocular disease activity at follow-up visits: slit-lamp examination, assessment of scleral injection (blanching test), IOP measurement (steroid-induced glaucoma monitoring), corneal integrity (peripheral ulcerative keratitis surveillance), visual acuity
- Communicate flare status to the rheumatologist in a structured format ('scleritis active — current treatment inadequate; suggesting step-up')
The rheumatologist's role:
- Confirm and manage the underlying systemic diagnosis
- Initiate disease-modifying therapy:
- Methotrexate — first-line immunosuppressant for RA-associated scleritis
- Azathioprine / mycophenolate mofetil — alternatives for RA and SLE
- Cyclophosphamide — for GPA and severe necrotising scleritis; high toxicity mandates careful monitoring
- Rituximab (anti-CD20 monoclonal antibody) — for GPA and RA-associated scleritis refractory to cyclophosphamide; increasingly preferred over cyclophosphamide for GPA in remission induction
- Anti-TNF agents (infliximab, adalimumab) — for refractory RA-associated scleritis
- Monitor systemic disease markers (ANCA titres, CRP, ESR, complement levels, renal function)
Shared decision-making on corticosteroid dose: oral prednisolone is the bridge therapy until disease-modifying agents take effect (typically 6-12 weeks). Both specialties must agree on the steroid taper, because abrupt reduction can precipitate both ocular and systemic relapse. The ocular activity at slit-lamp and the systemic activity markers (CRP/ESR/ANCA) together inform the taper rate.
For scleromalacia perforans (necrotising scleritis without inflammation in RA): no effective anti-inflammatory treatment exists for the scleral lesion itself. Rheumatology optimises RA therapy to prevent further scleral damage; ophthalmology provides protective management (avoidance of ocular trauma, protective spectacles, lubricants, monitoring for perforation). Scleral patching may be required for areas at risk of perforation.
SELF-CHECK
A 58-year-old man with known rheumatoid arthritis presents with newly diagnosed diffuse anterior scleritis. He has no systemic symptoms beyond his known joint disease. What is the most appropriate initial management step?
A. Topical corticosteroid eye drops only; no systemic treatment needed as scleritis is limited to the eye
B. Immediate high-dose oral prednisolone 1 mg/kg/day without referral
C. Oral NSAIDs (e.g. flurbiprofen 100 mg three times daily) plus routine rheumatology referral
D. Emergency nephrology referral due to risk of renal involvement in all RA patients with scleritis
Reveal Answer
Answer: C. Oral NSAIDs (e.g. flurbiprofen 100 mg three times daily) plus routine rheumatology referral
All confirmed scleritis — including diffuse anterior scleritis — requires systemic treatment (not just topical) and rheumatology referral. Oral NSAIDs (flurbiprofen or indomethacin) are first-line for diffuse/nodular anterior scleritis. Topical drops alone are insufficient. High-dose oral prednisolone is reserved for NSAID failure or necrotising subtypes. Emergency nephrology referral is not required for straightforward RA-associated scleritis without renal symptoms or haematuria.
Self-Assessment: Systemic Thinking in Episcleritis and Scleritis
Before moving to the summary, consolidate your learning with these applied reasoning challenges. The diagnostic and referral decisions in this SDL require you to synthesise the systemic epidemiology of scleritis, the targeted investigation strategy, and the ophthalmologist-rheumatologist partnership model — skills that are best cemented through effortful self-testing rather than passive review. Work through each scenario before checking your reasoning against the core principles covered in this SDL.
Scenario 1. A 40-year-old woman presents to the ophthalmology clinic with a four-week history of right eye scleritis, confirmed on examination (deep violaceous injection, severe boring pain, non-blanching). She mentions morning stiffness of her fingers lasting two hours and bilateral wrist swelling for the past year, but has not seen a rheumatologist. (a) Which systemic diagnosis should be at the top of your differential for the underlying cause of her scleritis? (b) Which three blood tests are most diagnostically important? (c) To whom and with what urgency should you refer?)
Scenario 2. A 65-year-old man with a fifteen-year history of seropositive RA presents with progressive painless scleral thinning bilaterally, with bluish discolouration visible at the scleral thinning sites. He reports no redness and no pain. (a) What specific condition does this represent and what is its clinical paradox? (b) What is the most serious complication this patient faces and how would it present? (c) What is the management strategy?)
Scenario 3. A 28-year-old man presents with left eye scleritis. Systemic history reveals recurrent epistaxis, haemoptysis, and a persistently blocked nose. Urinalysis shows haematuria. (a) What is the most likely systemic diagnosis, and which ANCA type is most strongly associated? (b) What chest investigation is indicated? (c) Which ophthalmological complication of this systemic disease, other than scleritis, should you specifically look for?)
Review your answers against the systemic associations table and investigation panel in this SDL. If you are uncertain about any scenario, revisit the relevant content block before proceeding to the summary.