Page 11 of 18
OP6.4 | Systemic Uveitis Associations and Patient Counselling — SDL Guide
Learning Objectives
- Enumerate the systemic conditions associated with anterior, intermediate, posterior, and panuveitis
- Identify the clinical features of each systemic association that link the ocular presentation to the underlying disease
- Apply a structured five-domain framework to counsel patients with uveitis in a simulated environment
- Critically evaluate common errors in patient counselling about uveitis (over-reassurance, jargon, incomplete explanation of recurrence risk)
INSTRUCTIONS
Uveitis is often the presenting feature of a systemic disease — ankylosing spondylitis, sarcoidosis, Behçet's disease, JIA — that would otherwise have been missed for months or years. The ophthalmologist's ability to recognise these associations not only saves vision but may accelerate diagnosis of a systemic condition with significant morbidity. Equally important is the counselling skill: once the diagnosis is made, patients need to understand their chronic, recurrent disease, their medications, the systemic implications, and the red flags that warrant emergency return. OP6.4 is explicitly a communication competency (SH level — patient counselling in a simulated environment) in addition to a knowledge competency.
References
- Khurana AK. Comprehensive Ophthalmology, 7th ed. Ch. 8 — Diseases of the Uveal Tract (textbook)
- Parsons' Diseases of the Eye, 23rd ed. Ch. 17 — The Uveal Tract (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 32-year-old man presents with his third episode of acute painful left eye in two years. Each time, he has been treated with eye drops and improved. This time, as you examine him, you notice he walks with a slightly stiff gait and has difficulty turning his neck. He has never been told he has any systemic illness. You diagnose acute anterior uveitis and are about to prescribe atropine and prednisolone drops — but you pause. What systemic disease must you consider? What blood test will you order today? And when you counsel him about his eye disease, what does he absolutely need to know about the relationship between his eyes, his back, and his future health?
WHY THIS MATTERS
The ophthalmology outpatient clinic is, in many cases, the first place a patient encounters a physician who connects their recurrent eye inflammation with a systemic disease. As a doctor — whether in ophthalmology, general medicine, or primary care — you must be able to enumerate the systemic conditions that cause uveitis, recognise the clinical clues that link the eye to the body, and communicate this complex, chronic, often frightening diagnosis to patients and families in clear, compassionate, jargon-free language. OP6.4 is the competency that requires you to do both: know the associations, and counsel in a simulated environment. The communication skill is as examinable as the factual recall — both require deliberate practice.
RECALL
From OP6.1, recall that uveitis is classified anatomically (anterior/intermediate/posterior/panuveitis) by the SUN Working Group criteria. From OP6.1, recall also that granulomatous iridocyclitis (mutton-fat KPs, Koeppe/Busacca nodules) is associated with specific systemic conditions (sarcoidosis, TB, VKH) while non-granulomatous disease is predominantly HLA-B27-associated. From OP6.2, recall the investigation protocol — HLA-B27 typing, chest X-ray, Mantoux/IGRA, serum ACE — and when each is indicated. In this module, you will extend that knowledge to the full spectrum of systemic associations and learn to communicate the diagnosis, implications, and management plan to a patient using a structured counselling framework. Recall also from your communication skills training the core principles of patient-centred communication: ask first, then tell; check understanding; avoid jargon; invite questions.
Uveitis as a Window into Systemic Disease: Why Ophthalmologists Are Diagnosticians
One of the defining features of uveitis in clinical medicine is that the eye often reveals systemic disease before any other organ declares itself. Ankylosing spondylitis may smoulder for years as intermittent back pain before a classical acute anterior uveitis episode prompts HLA-B27 testing and a rheumatology diagnosis. Sarcoidosis may be asymptomatic except for bilateral granulomatous uveitis, prompting a chest X-ray that reveals bilateral hilar lymphadenopathy. JIA-associated uveitis in children is entirely asymptomatic — only regular slit-lamp screening detects the inflammation before it causes band keratopathy and vision loss. This sentinel role of the eye in systemic disease is not a curiosity — it is a clinical responsibility. The ophthalmologist who examines an acute uveitis patient and records only the ocular findings, without considering and documenting the systemic differential and arranging appropriate investigation, has discharged only half the clinical duty. The other half — connecting the eye to the body — is what transforms a competent eye doctor into a genuinely valuable clinician within the wider healthcare system.
This diagnostic role places the ophthalmologist at the intersection of internal medicine and surgical specialism — and demands two complementary competencies from every eye doctor:
1. Disease knowledge: recognising the clinical signature in the eye that points to a specific systemic condition, and knowing which investigation to order.
2. Communication skill: explaining to the patient — who may have walked in with 'just a red eye' — that they may have a systemic inflammatory or infectious disease requiring multi-disciplinary management, long-term monitoring, and potentially systemic immunosuppression.
The counselling encounter in uveitis is particularly challenging because the diagnosis is often chronic, the disease is often invisible between episodes, and the systemic implications can be alarming. Getting this communication right — in a simulated environment during training and in real clinical encounters thereafter — is the focus of this SDL.
Major Systemic Associations of Anterior Uveitis
Anterior uveitis has the broadest range of systemic associations because it is the most prevalent anatomical type. Organising these by clinical syndrome prevents memorisation fatigue and creates a clinically useful diagnostic framework. Rather than memorising a list of diseases associated with uveitis — a task that leads to superficial, rapidly forgotten knowledge — the goal here is to understand the pattern of each association well enough that you can reason to the correct investigation from the clinical presentation. A 32-year-old man with recurrent unilateral acute anterior uveitis and morning back stiffness tells a very different story from a 9-year-old girl with oligoarticular JIA and silent bilateral inflammation, even though both have anterior uveitis. The systemic context — age, laterality, course, granulomatous versus non-granulomatous pattern, and any accompanying systemic symptoms — is the clinical scaffold that makes the associations meaningful and memorable.
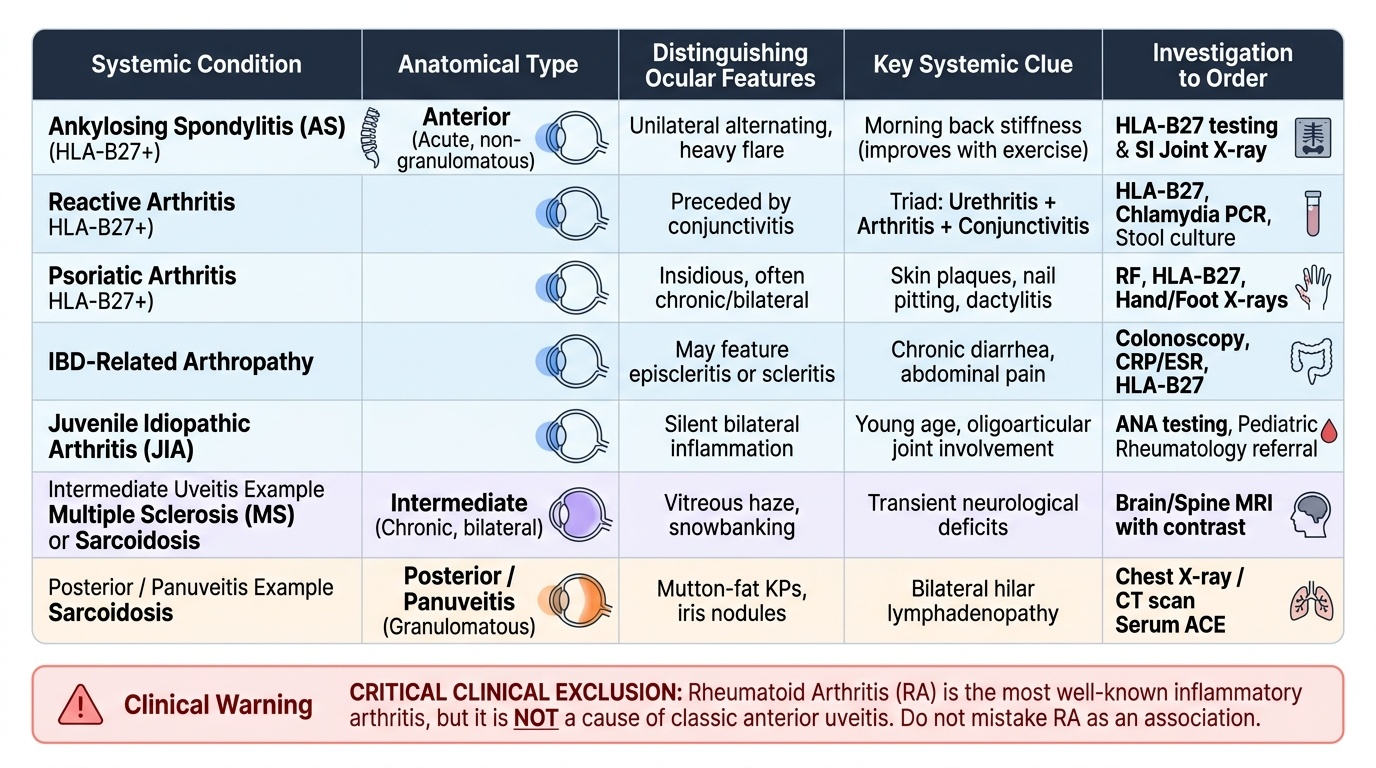
Provided image
HLA-B27-positive spondyloarthropathies (the most common identifiable cause of acute anterior uveitis):
The HLA-B27 antigen links four rheumatological conditions that all carry a significant risk of acute, non-granulomatous, recurrent anterior uveitis:
- Ankylosing spondylitis (AS): Chronic inflammatory arthritis of the sacroiliac joints and spine. Classic symptoms: morning stiffness improved by exercise (the opposite of mechanical back pain), progressive spinal rigidity, bamboo spine on X-ray. Uveitis occurs in ~25–40% of AS patients, typically acute, unilateral, alternating.
- Reactive arthritis (formerly Reiter's syndrome): Triad of urethritis/cervicitis + arthritis + conjunctivitis/uveitis, occurring 1–4 weeks after a genitourinary (Chlamydia) or gastrointestinal (Salmonella, Shigella, Yersinia, Campylobacter) infection. Now called reactive arthritis to remove the eponym.
- Psoriatic arthritis: Inflammatory arthritis associated with psoriasis; uveitis occurs in ~7–25% of psoriatic arthritis patients.
- IBD-related arthropathy: Both Crohn's disease and ulcerative colitis can cause peripheral or axial arthropathy and anterior uveitis. Uveitis activity may or may not parallel bowel disease activity.
Important exclusion: Rheumatoid arthritis (RA) is NOT a cause of classic anterior uveitis (despite being the most well-known inflammatory arthritis). RA is associated with scleritis and keratoconjunctivitis sicca (dry eye), not with iridocyclitis.
JIA (juvenile idiopathic arthritis) — oligoarticular ANA-positive type:
The highest-risk JIA subtype for chronic anterior uveitis is oligoarticular JIA in young girls who are ANA-positive. The uveitis is asymptomatic, bilateral, and progressive — requiring regular slit-lamp screening every 3 months for the first 4 years after arthritis onset (regardless of symptoms). Band keratopathy and cataract are the hallmark complications.
Behçet's disease:
A systemic vasculitis characterised by the diagnostic triad of recurrent oral aphthous ulcers + genital ulcers + ocular inflammation. The uveitis is severe, bilateral, panuveitis pattern with migratory hypopyon (as discussed in OP6.3). Particularly common along the Silk Road (Turkey, Middle East, Central Asia, East Asia).
Herpetic uveitis (herpes simplex virus and varicella-zoster virus):
HSV and VZV can cause anterior uveitis, often with elevated IOP (due to trabecular involvement — trabeculitis), sectoral iris atrophy, and KPs that may be pigmented. Diagnosis is supported by history of herpetic disease; treatment includes antiviral cover (aciclovir) alongside topical steroids.
Systemic Associations of Intermediate, Posterior, and Panuveitis
Intermediate, posterior, and panuveitis have more restricted but equally important systemic associations. Understanding these requires recognising that posterior segment involvement generally signals a more systemic or infectious process. Unlike anterior uveitis — where purely local, idiopathic inflammation is common — intermediate and posterior uveitis rarely occur without a definable cause, and the search for that cause is both clinically urgent and therapeutically determinative. A young adult with intermediate uveitis and vitreous snowballs may be harbouring early multiple sclerosis; missing this connection delays a neurological diagnosis that carries significant long-term consequences beyond the eye. Similarly, posterior uveitis in an immunocompromised patient in India demands immediate consideration of CMV retinitis and TB choroiditis simultaneously — conditions requiring opposite treatments (antiviral versus antimycobacterial) that cannot both be started empirically without diagnostic clarity. The systemic context is therefore not background information but the primary clinical driver in posterior segment uveitis.
Intermediate uveitis (pars planitis) and systemic associations:
- Multiple sclerosis (MS): Approximately 10–15% of patients with intermediate uveitis have MS, and conversely, intermediate uveitis occurs in ~10% of MS patients. The ophthalmologist may be the first to suspect MS in a young adult with pars planitis and subtle neurological symptoms.
- Sarcoidosis: Can cause any anatomical type; intermediate uveitis with vitreous 'snowballs' is a sarcoidosis pattern.
- Lyme disease: Borrelial uveitis can present as intermediate uveitis in endemic areas; history of tick bite or erythema migrans rash.
Posterior uveitis systemic associations:
- Toxoplasma gondii (toxoplasma retinochoroiditis): The most common cause of posterior uveitis globally. Presents as a focal necrotising pale lesion in the retina adjacent to an old pigmented scar (the 'headlight in fog' appearance). Most commonly reactivation of congenital infection. Acquired by ingestion of undercooked meat or contaminated soil/water.
- CMV retinitis: Occurs in severely immunocompromised patients (HIV with CD4 <50 cells/μL). Characteristic 'pizza-pie' or 'scrambled-egg' appearance of the fundus — areas of retinal necrosis and haemorrhage along vascular arcades. Life-threatening opportunistic infection.
- Tuberculosis (TB choroiditis): The most important cause of posterior uveitis in India. Presents as choroidal tubercles (yellowish-white discrete lesions), serpiginous-like choroidopathy, or multifocal choroiditis. Requires ATT; endemic context critical.
- Ocular histoplasmosis: Seen in endemic areas (Ohio/Mississippi valley in USA); classic triad of peripapillary atrophy, macular scar, and peripheral 'histo spots'; usually inactive.
Panuveitis systemic associations:
- Vogt-Koyanagi-Harada (VKH) syndrome: Bilateral granulomatous panuveitis with exudative retinal detachment in the acute phase, followed by a convalescent (sunset-glow fundus) and chronic phase. Associated with systemic features affecting melanocyte-containing tissues: neurological (meningism, tinnitus, dysacusis, CSF pleocytosis in the meningitic phase), and dermatological (vitiligo, alopecia, poliosis — whitening of hair/eyebrows/eyelashes). More common in pigmented races (Japanese, Indian, Middle Eastern, Latin American). High-dose systemic steroids are the treatment.
- Sympathetic ophthalmia: Bilateral granulomatous uveitis following penetrating injury or surgery (including vitreoretinal surgery) to one eye. The injured eye is the exciting eye; the fellow uninjured eye develops inflammation and is called the sympathising eye. The latency period is typically 2 weeks to 2 years, rarely longer. Mechanism: exposure of uveal antigens at the wound site sensitises T-lymphocytes, which then attack melanocyte-associated antigens in both eyes. Critical prevention fact: enucleation of the exciting eye within 2 weeks of injury can prevent sympathetic ophthalmia in the sympathising eye — after 2 weeks, enucleation does not reliably prevent it.
SELF-CHECK
A 16-year-old girl with oligoarticular JIA (ANA-positive, diagnosed at age 12) has never had a red eye or eye pain. At what interval should she be having slit-lamp examinations for uveitis screening?
A. Only when she develops eye symptoms (red eye or blurred vision)
B. Every 12 months, as her JIA is well controlled
C. Every 3 months, as she is ANA-positive oligoarticular JIA within 4 years of arthritis onset
D. Every 6 months, as she is now older than 15 years
Reveal Answer
Answer: C. Every 3 months, as she is ANA-positive oligoarticular JIA within 4 years of arthritis onset
JIA-associated uveitis is completely asymptomatic — waiting for symptoms means waiting until complications have occurred. ANA-positive oligoarticular JIA within 4 years of arthritis onset carries the highest uveitis risk and requires slit-lamp screening every 3 months. After 4 years, the frequency reduces to every 6 months. She is now 4 years into her disease (diagnosed age 12, now 16) so she may be transitioning to 6-monthly — but the principle of asymptomatic screening remains absolute. Only if she were ANA-negative would 6-monthly screening apply from the start.