Page 11 of 20
OP7.4 | Secondary Glaucoma: Cause Framework — SDL Guide (Part 2)
Cause-by-Cause Catalogue: Named Secondary Glaucomas
Building on the mechanistic framework, the following catalogue covers the major secondary glaucomas that a final-year MBBS student must know. Each entry is anchored to its mechanism branch, characteristic clinical sign, and key management principle.
Provided image
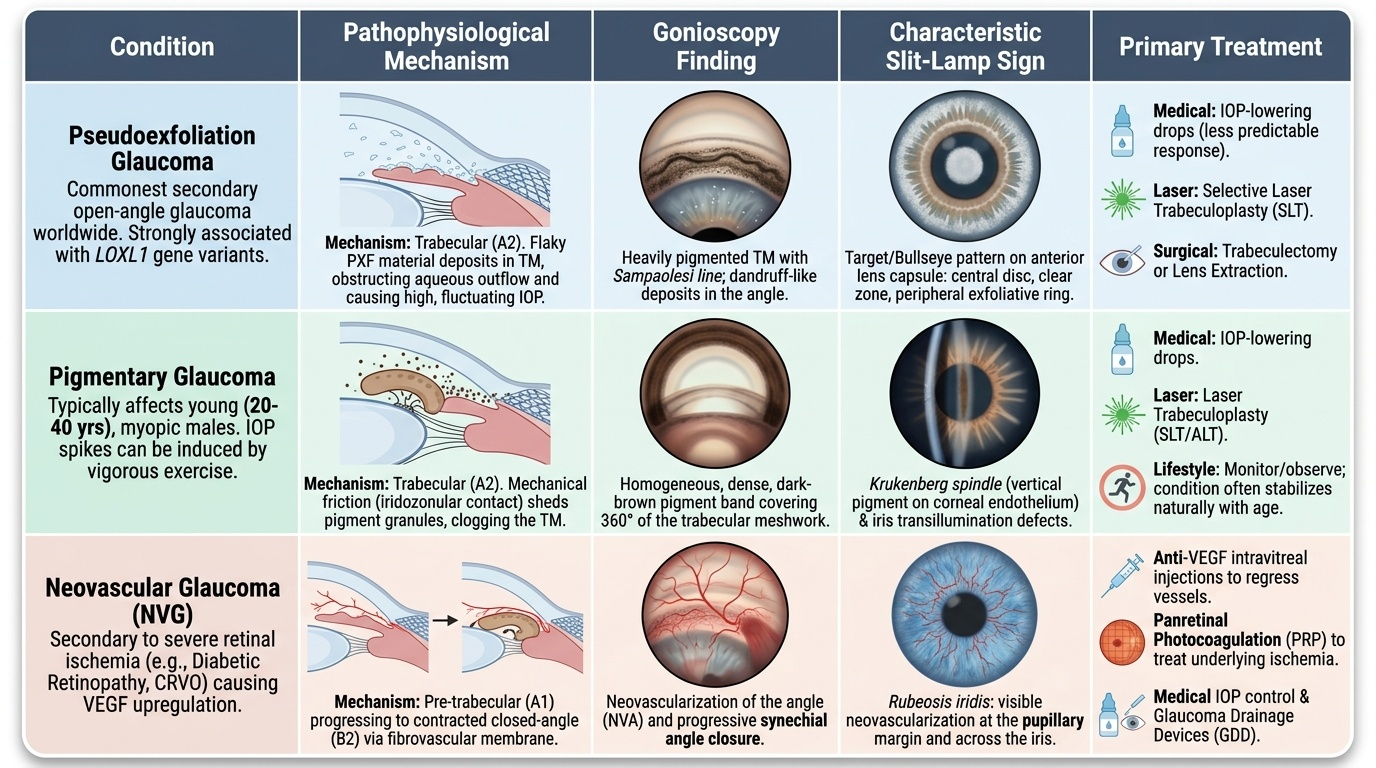
1. Pseudoexfoliation Glaucoma (COMMONEST secondary open-angle glaucoma worldwide)
Mechanism: trabecular (A2). PXF material — a fibrillar extracellular glycoprotein produced by abnormal processing of elastic microfibrils — deposits throughout the anterior segment. Characteristic slit-lamp sign: a white 'dandruff-like' ring on the anterior lens capsule with a central clear disc (where the iris rubs it off) and a mid-peripheral pigment zone. PXF material also deposits in the trabecular meshwork, obstructing outflow. IOP is typically markedly elevated and shows wide diurnal fluctuation — making glaucoma harder to control. Genetics: LOXL1 gene variants strongly associated. Treatment: same as POAG (drops, SLT, trabeculectomy) but responds less predictably; lens extraction may help.
2. Pigmentary Glaucoma
Mechanism: trabecular (A2). Occurs in young (20–40 years), myopic males with a posteriorly bowed (concave) iris that rubs against the anterior zonule-lens equator interface, liberating iris pigment epithelium granules. These granules deposit: on the corneal endothelium as a vertical fusiform band (Krukenberg spindle), in the trabecular meshwork (causing outflow obstruction), and on the anterior chamber structures. Exercise (jogging, cycling) acutely disperses pigment and transiently raises IOP — the 'exercise-induced IOP spike' is a diagnostic clue. Treatment: IOP-lowering drops; laser trabeculoplasty; observe — many stabilise with age as the lens grows and iridozonular friction reduces.
3. Neovascular Glaucoma (NVG)
Mechanism: pre-trabecular (A1) → closed-angle (B2, contracted). Caused by retinal ischaemia → VEGF upregulation → rubeosis iridis (neovascularisation of the iris — new vessels first appear at the pupil margin and at the angle). The fibrovascular membrane initially covers but doesn't close the angle (open-angle NVG with high IOP); as the membrane contracts, it drags the iris over the angle, closing it permanently with peripheral anterior synechiae (closed-angle NVG). Leading causes: proliferative diabetic retinopathy (PDR), central retinal vein occlusion (CRVO), ocular ischaemic syndrome (carotid artery disease). Treatment: anti-VEGF injection (causes rapid regression of rubeosis — buys time); pan-retinal photocoagulation (PRP) to ablate ischaemic retina (removes the VEGF stimulus); IOP control with drops; filtration surgery if needed.
4. Steroid-Induced Glaucoma
Mechanism: trabecular (A2). Glucocorticoids (topical, systemic, periocular, inhaled) reduce phagocytic activity of trabecular endothelial cells → extracellular matrix accumulates → outflow resistance increases → IOP rises. The IOP rise typically begins 2–6 weeks after starting steroids and reverses within 2–4 weeks of stopping (if no structural TM damage has occurred). Potency: subconjunctival > topical > systemic (for ocular IOP effects). 'Steroid responders' (those with a ≥10 mmHg IOP rise) are at higher risk of having POAG. Clinical importance: steroids are prescribed by virtually every specialty; ophthalmological monitoring during steroid therapy is mandatory. Treatment: stop or substitute steroid (loteprednol, fluorometholone have lower IOP-raising potential); IOP-lowering drops; trabeculectomy if uncontrolled.
5. Uveitic Glaucoma
Mechanism: BOTH open-angle (trabeculitis, steroid side effect) and closed-angle (posterior synechiae → seclusio pupillae → pupil block → iris bombe). Anterior uveitis causes trabecular meshwork inflammation (trabeculitis) AND is typically treated with topical steroids (further raising IOP). Posterior synechiae (iris-lens adhesions) → 360° involvement = seclusio pupillae → complete pupil block → iris bombe → closed angle. On slit-lamp: keratic precipitates (KPs), cells and flare in AC, posterior synechiae visible at the pupil margin. Treatment: treat underlying uveitis (steroids paradoxically necessary but must be balanced); IOP-lowering drops; laser iridotomy if closed-angle with pupil block; cycloplegics to prevent synechiae formation.
6. Lens-Induced Glaucomas: Phacomorphic vs Phacolytic — the critical contrast
Phacomorphic glaucoma (closed-angle — B2, without pupil block): An intumescent (swollen, mature or immature) cataract absorbs fluid and expands, physically pushing the iris-lens diaphragm forward, mechanically closing the iridocorneal angle. Angle is CLOSED on gonioscopy. Presentation: acute, painful red eye (similar to acute PACG attack), very high IOP. Treatment: lens extraction (phacoemulsification) — removes the cause; IOP-lowering medications as bridge.
Phacolytic glaucoma (open-angle — A2, trabecular): A hypermature (Morgagnian) cataract has a liquefied cortex; lens proteins leak through the intact (but permeable with age) capsule. Macrophages engulf the lens material and enter the anterior chamber in large numbers; both the lens proteins and the macrophage-laden debris clog the trabecular meshwork. Angle is OPEN on gonioscopy (flocculent white material visible). Presentation: pain, red eye, elevated IOP in an eye with very dense cataract. Treatment: lens extraction — removes the source of the obstructing material.
Key contrast: phacomorphic = closed angle (big swollen lens pushes iris forward); phacolytic = open angle (lens protein + macrophages clog TM). Gonioscopy distinguishes them.
7. Traumatic Glaucoma (Angle Recession)
Mechanism: trabecular (A2, late). A blunt ocular injury (fist, ball, airbag) causes a tear in the anterior face of the ciliary body, between the longitudinal and circular muscle layers. On gonioscopy, the angle appears abnormally wide with a visible grey-white band of ciliary body and disrupted scleral spur. In the acute phase, a traumatic hyphaema (blood in anterior chamber) raises IOP. Years to decades later, progressive fibrous metaplasia of the injured trabecular meshwork leads to chronic open-angle glaucoma. It is UNILATERAL and associated with a history of trauma — always ask about previous ocular injuries.
8. Ghost Cell Glaucoma
Mechanism: trabecular (A2). Following a vitreous haemorrhage, red blood cells degenerate over weeks into rigid, pale khaki-coloured ghost cells (erythrocyte ghosts — degenerated cells that have lost haemoglobin). These rigid cells cannot squeeze through the trabecular meshwork pores and accumulate in the angle, obstructing outflow. Slit-lamp: khaki or hazel cells in the anterior chamber or visible as a khaki pseudohypopyon. Treatment: IOP control; anterior chamber washout if severe.
9. Sturge-Weber Syndrome
Mechanism: post-trabecular (A3). The episcleral haemangioma (part of the facial/leptomeningeal angioma) increases episcleral venous pressure. Since aqueous drains into the episcleral venous system, any increase in episcleral venous pressure is transmitted back to the angle, raising IOP. The glaucoma may be ipsilateral to the port-wine naevus. Treatment: IOP-lowering drops (prostaglandins may be challenging due to episcleral venous pressure dependency); trabeculectomy with caution (risk of choroidal effusion — 'expulsive haemorrhage risk').
CLINICAL PEARL
The two lens-induced glaucomas — phacomorphic and phacolytic — are easily confused but are mechanistically opposite and require the same treatment (lens extraction) for opposite reasons. The key memory hook: MORPHIC = MASS effect (the big swollen lens closes the angle by physical bulk); LYTIC = LEAK (the dissolving hypermature lens leaks proteins that clog open trabecular channels). Always examine the gonioscopy: closed angle = phacomorphic; open angle with white fluffy material = phacolytic. Another clinical pearl: neovascular glaucoma demands that you find and treat the retinal ischaemia, not just lower the IOP. Anti-VEGF buys time but pan-retinal photocoagulation removes the ischaemic stimulus — treat the cause.
Management Principles: Treat the Cause, Control the IOP
The management of secondary glaucoma follows a two-pronged strategy that distinguishes it from primary glaucoma: simultaneously reduce IOP (the common pathway of optic nerve damage) and treat the underlying cause (which, if successfully addressed, may resolve the glaucoma without lifelong IOP medication). This dual-track approach is philosophically different from POAG management, where IOP reduction is both the sole and the lifelong intervention. In secondary glaucoma, IOP reduction is the emergency measure that protects the optic nerve while the underlying cause is being addressed; cause treatment is the definitive intervention that may make IOP reduction unnecessary in the long term. Understanding which IOP-lowering agents are safe or contraindicated in each secondary glaucoma type is also critical — the drug list is not the same as for POAG. Prostaglandin analogues are generally avoided in active uveitic glaucoma because they may worsen intraocular inflammation and precipitate cystoid macular oedema. Pilocarpine is contraindicated in phacomorphic glaucoma because it increases lens-iris apposition and may worsen the angle closure. These cause-specific contraindications reflect the principle that mechanism determines management, not merely IOP level.
Prong 1 — IOP-lowering therapy:
The same drug classes used in POAG are available for secondary glaucoma, but choice must account for the underlying mechanism and contraindications:
- Prostaglandin analogues (latanoprost): increase uveoscleral outflow; generally safe; AVOID in active uveitic glaucoma (may worsen inflammation, precipitate cystoid macular oedema)
- Beta-blockers (timolol): reduce aqueous production; safe in most secondary types; avoid in asthma
- Carbonic anhydrase inhibitors (dorzolamide topical, acetazolamide systemic): reduce aqueous production; useful in acute high-IOP emergencies
- Alpha-2 agonists (brimonidine): reduce production + increase uveoscleral outflow; avoid in uveitic glaucoma (theoretically pro-inflammatory) and in children
- Miotics (pilocarpine): APPROPRIATE in uveitic angle-closure with pupil block (open the angle); AVOID in phacomorphic (lens is pushing the iris, pilocarpine worsens lens-iris contact) and in NVG (no angle mechanism to open)
Prong 2 — Treat the underlying cause:
- Steroid-induced: withdraw or reduce steroid; switch to lower-potency steroid (loteprednol, fluorometholone)
- Neovascular glaucoma: anti-VEGF injection + pan-retinal photocoagulation for PDR/CRVO
- Phacomorphic / phacolytic: lens extraction
- Uveitic: immunosuppression, cycloplegics; laser iridotomy for pupil-block closed angle
- Pseudoexfoliation / pigmentary: address with standard IOP-lowering; lens extraction may help PXF
- Angle recession: IOP-lowering drops; trabeculectomy if progressive
Surgical options:
Trabeculectomy (with MMC), glaucoma drainage devices (Ahmed, Baerveldt implants), and cyclodestructive procedures are used when medical therapy is insufficient. Neovascular glaucoma and uveitic glaucoma are known to have poorer surgical outcomes due to scarring and inflammation.
Key principle: the secondary glaucoma that is caught early (before PAS formation, before significant optic nerve damage) and whose underlying cause is reversible has the best prognosis. Screening for IOP in high-risk groups (steroid users, diabetic retinopathy patients, post-traumatic eyes) is as important as clinic-based treatment.
SELF-CHECK
A 65-year-old woman with longstanding anterior uveitis develops a IOP of 40 mmHg. Slit-lamp shows 360-degree posterior synechiae with the iris bowed forward touching the cornea peripherally. Gonioscopy confirms angle closure with iris bombe. What is the MECHANISM of this closed-angle glaucoma and the most appropriate initial intervention?
A. Pre-trabecular (fibrovascular membrane) — anti-VEGF injection
B. Pupil block from seclusio pupillae — laser peripheral iridotomy (LPI)
C. Trabecular clogging by PXF material — topical prostaglandins
D. Post-trabecular (raised episcleral venous pressure) — trabeculectomy
Reveal Answer
Answer: B. Pupil block from seclusio pupillae — laser peripheral iridotomy (LPI)
This is uveitic closed-angle glaucoma due to seclusio pupillae (360-degree posterior synechiae) causing complete pupil block → iris bombe → angle closure. The mechanism is pupil block (B1 in the framework). The appropriate intervention is laser peripheral iridotomy (LPI) to create an alternate aqueous flow path, bypassing the occluded pupil. Anti-VEGF is for neovascular glaucoma. Prostaglandins/PXF management addresses trabecular-level open-angle disease. Trabeculectomy is not the initial step when the angle is closed from a reversible pupil-block cause.
Self-Assessment: Clinical Reasoning in Secondary Glaucoma
Having mapped the mechanistic framework of secondary glaucoma and catalogued its major named types, you are now ready to apply this knowledge to integrated clinical reasoning — the kind of thinking required in an OSCE station or when a real patient presents with an unusual combination of findings.
Return to the three patients from the hook and build their full management plans. Patient A (35-year-old myopic male, Krukenberg spindle, IOP 28 mmHg): this is pigmentary glaucoma. The management is IOP-lowering drops (prostaglandin analogue first-line, but with awareness that exercise causes transient IOP spikes — ask about sports habits), selective laser trabeculoplasty, and counselling that the condition may naturally stabilise with age as the lens grows and iridozonular friction decreases. He needs regular perimetry and OCT RNFL to detect field progression. Patient B (70-year-old diabetic, rubeosis iridis, IOP 46 mmHg): this is neovascular glaucoma from proliferative diabetic retinopathy. The immediate priorities are intravitreal anti-VEGF injection (causes rapid regression of rubeosis within 24–72 hours, buying a window for further intervention), urgent pan-retinal photocoagulation to destroy ischaemic retina and eliminate the VEGF source, and IOP reduction with acetazolamide and timolol while awaiting laser. His systemic diabetes must be optimally controlled. Patient C (65-year-old on prednisolone drops, IOP 34 mmHg from baseline 14 mmHg): steroid-induced glaucoma. Stop or reduce the prednisolone if possible; switch to loteprednol or fluorometholone (lower IOP-raising potential); add IOP-lowering drops (timolol, dorzolamide); recheck IOP in 2–4 weeks expecting normalisation. If the inflammatory condition absolutely requires steroid continuation, add IOP-lowering medication and monitor closely.
A key self-assessment question: which of the following patients has the CLEAREST textbook contraindication to pilocarpine? (a) A patient with uveitic closed-angle glaucoma from seclusio pupillae; (b) a patient with phacomorphic glaucoma; (c) a patient with neovascular glaucoma. Answer: (b) phacomorphic is the clearest contraindication — pilocarpine increases lens-iris contact, worsening the mechanical angle closure from the swollen lens. However, this is a nuanced question: all three are cases where pilocarpine should be avoided or is not the correct treatment. In (a), seclusio pupillae (360° posterior synechiae), pilocarpine is NOT appropriate — the iris pupil margin is already tethered by synechiae and cannot constrict further; the correct intervention is laser peripheral iridotomy (LPI) to bypass the blocked pupil, plus cycloplegics (not miotics) to prevent further synechiae formation. Pilocarpine is appropriate for simple pupil-block in an acute PACG attack where the iris is anatomically normal and mobile, not in a synechiae-frozen iris. In (c), pilocarpine is also avoided in NVG — the angle is closed by a contracted fibrovascular membrane, not by a mobile iris that pilocarpine can retract; pilocarpine would be both ineffective and potentially harmful.