Page 17 of 23
OP8.6 | IMG Team Participation in Cataract Surgery — SDL Guide (Part 2)
Intraoperative Participation and Sterile Technique
The IMG's intraoperative role ranges from observer to active assistant, depending on the operating team's structure and the IMG's experience. Regardless of specific duties, two principles always apply: maintain sterility and anticipate the surgical sequence.
Sterile technique:
Anything within the sterile field — draped instruments, the surgeon's gloved hands, the surgical site — must not be contaminated. The IMG who is 'scrubbed' (gowned and gloved, part of the sterile team) must avoid touching non-sterile surfaces and must move around the patient without crossing the sterile field. The IMG who is 'un-scrubbed' (scout/circulator role) can handle non-sterile items, open packs onto the instrument tray, and manage the microscope or phaco machine settings at the surgeon's request — but must not reach into the sterile field.
Understanding the surgical sequence:
Having studied ECCE steps and phacoemulsification, you now understand the logical order of a cataract operation. This is operationally valuable: you know that after nucleus delivery comes cortex aspiration, and after I/A comes IOL insertion — so you can prepare the IOL introducer without being asked. The ability to anticipate one step ahead is what separates a useful scrub assistant from one who creates unnecessary pauses.
Specific intraoperative IMG duties may include:
- Monitoring the irrigation bottle level (BSS) and alerting the surgeon when it is low
- Confirming the correct IOL power before it is opened (by reading aloud the IOL label: power, type, and sterility expiry)
- Recording operative events (start time, anaesthesia administered, complications if any) in the operation notes
- Maintaining the running count of swabs and instruments (preventing retained foreign body)
- Adjusting the room lighting at the surgeon's request
- In camp settings: calling the next patient from the waiting area, ensuring the correct eye is marked
Critical safety check — correct eye verification:
Before draping, the IMG should confirm (with the patient verbally if awake): 'We are operating on your RIGHT/LEFT eye today, is that correct?' This verbal confirmation, combined with the consent form and surgical mark, is part of the WHO Surgical Safety Checklist that applies to all surgical specialities including ophthalmology.
Post-operative Care and Complication Recognition
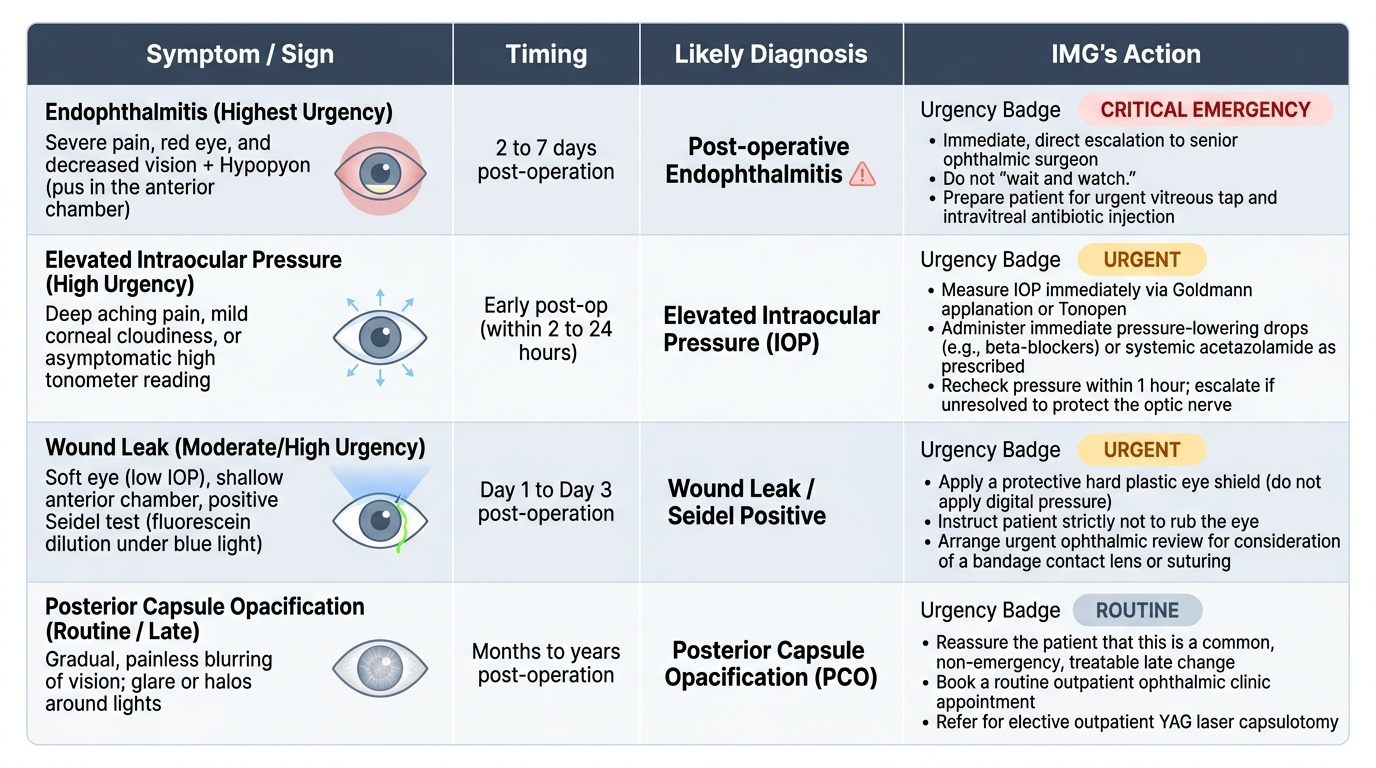
The post-operative period is where the IMG's knowledge of cataract surgery directly translates into patient safety decisions. Knowing which post-operative findings are expected and which are red flags — and acting on the latter without delay — is the core clinical skill at this stage. In a busy ophthalmic unit, the intern is often the first doctor to see a post-operative patient reporting discomfort or worsening vision, and the ability to triage correctly — routine review versus emergency intervention — is a genuine patient safety competency. Post-operative endophthalmitis, the most feared complication, evolves rapidly and demands immediate senior involvement and intravitreal antibiotic injection, not a wait-and-watch approach. Elevated IOP in the early post-operative period can permanently damage the optic nerve within hours if untreated. Conversely, a patient with mild watering, minimal grittiness, and no pain three days after surgery simply needs reassurance and an instruction to continue their drops. Developing the clinical judgment to distinguish these scenarios — using history, visual acuity measurement, and a structured examination — is the principal learning objective of this section.
Provided image
Writing Post-operative Orders:
The standard post-operative prescription after phacoemulsification or ECCE includes:
1. Antibiotic eye drops (e.g. moxifloxacin 0.5% or tobramycin 0.3%) — 4 times daily × 4 weeks
2. Topical steroid eye drops (e.g. prednisolone acetate 1% or dexamethasone 0.1%) — 4 times daily, tapering over 6 weeks
3. NSAIDs (e.g. ketorolac 0.4%) — 4 times daily × 4 weeks (especially in diabetics, high CMO risk)
4. Eye pad and shield: applied on day of surgery; removed at day-1 review
5. Activity restrictions: no rubbing, no swimming × 4 weeks
Post-operative Counselling by the IMG:
Before the patient leaves the ward on the day of surgery, the IMG explains:
- What to expect: mild watering, light sensitivity, and blurred vision on day 1 are normal
- Drop instillation technique (one drop per application, lower lid retraction, eyes closed for 1 minute)
- PCO counselling: 'In 1–2 years, the membrane behind your artificial lens may become slightly cloudy. This is NOT the cataract returning. The artificial lens cannot get a cataract. We treat this with a brief, painless laser procedure in the outpatient clinic — no surgery needed.'
- Follow-up appointments: day 1, week 1, week 6
Red Flag Complication Recognition:
The following post-operative presentations require IMMEDIATE escalation to the attending ophthalmologist — the IMG must not manage these independently:
Endophthalmitis (day 2–7): Sudden severe pain, marked red eye, photophobia, hypopyon (visible white level in the anterior chamber), and severe reduction in vision. This is a SIGHT-THREATENING EMERGENCY. Action: inform the supervising ophthalmologist immediately; prepare for emergency intravitreal antibiotics. Do NOT give only topical drops and discharge.
Elevated IOP (day 1–3): Patient complains of eye ache, feels 'pressure' or throbbing. Confirm with tonometry (Goldmann or Schiotz). Elevated IOP (>30 mmHg) → inform senior; likely residual viscoelastic or pupillary block → oral acetazolamide or topical IOP-lowering drops pending senior assessment.
Wound Leak (day 1–3): Watery eye beyond expected; fluorescein Seidel test positive (fluorescein stream at wound). Inform senior immediately; apply firm pressure padding and refer for surgical re-suturing.
Gradual Blurring Months Later: PCO (posterior capsular opacification) — rule out by examining the posterior capsule with slit-lamp; if opaque, refer for Nd:YAG capsulotomy outpatient. NOT an emergency, but NOT a reason to repeat surgery.
SELF-CHECK
A post-ECCE patient returns to your primary health centre on day 5 with a painful right eye, reduced vision (CF 1 m, was 6/18 at discharge), and a small white fluid level visible in the anterior chamber. Your most appropriate action is:
A. Start intensive topical antibiotic drops and review in 2 days
B. Prescribe oral ciprofloxacin and reassure the patient that mild post-operative inflammation is expected
C. Immediately contact the ophthalmology unit and arrange same-day emergency transfer
D. Apply a pressure patch and review the next morning
Reveal Answer
Answer: C. Immediately contact the ophthalmology unit and arrange same-day emergency transfer
This presentation — painful eye, reduced vision to CF (from 6/18), and hypopyon (white fluid level in anterior chamber) on day 5 post-cataract surgery — is post-operative endophthalmitis until proven otherwise. This is a sight-threatening surgical emergency requiring urgent intravitreal antibiotics, which can only be administered at an ophthalmology unit with the appropriate equipment and expertise. Topical antibiotics alone are inadequate for endophthalmitis. Oral ciprofloxacin does not achieve adequate intraocular drug levels. A pressure patch is inappropriate. The only correct action for an IMG in a primary care setting is immediate emergency ophthalmology referral — same day.
CLINICAL PEARL
The correct eye is the most important pre-operative check. Wrong-site surgery — operating on the wrong eye — is a 'never event' (should never happen in any healthcare setting, and is a sentinel adverse event if it does). The WHO Surgical Safety Checklist, adopted in all accredited Indian hospitals, requires three time-outs: at anaesthesia, before skin incision, and before patient leaves the theatre. As an IMG, your verbal confirmation of the correct eye with the awake patient — 'We are operating on your right eye today, is that correct?' — combined with the surgical mark (a dot on the periorbital skin at the correct side) and consent form verification, forms a three-way independent check. This two-second conversation has the potential to prevent a catastrophic surgical error. Make it a non-negotiable reflex.
The Cataract Camp and NPCBVI — IMG as Community Eye Health Advocate
India's cataract surgery programme is delivered not only in hospitals but in large-scale outreach camps — mobile surgical teams that reach rural and underserved populations where patients cannot access tertiary care. These camps are the operational backbone of the NPCBVI, and the IMG's participation in them extends well beyond the operating theatre.
The NPCBVI framework:
The National Programme for Control of Blindness and Visual Impairment (NPCBVI), originally launched in 1976, aims to reduce the prevalence of blindness from ~1.1% in 1990 to below 0.3%. Cataract accounts for approximately 65% of India's blindness burden. The programme funds cataract surgeries, IOL procurement, and surgical camps, with targets set as the Cataract Surgical Rate (CSR) — the number of cataract operations per million population per year. India's target CSR is 8,000/million (one of the highest in the world). The Vision 2020 'Right to Sight' initiative (WHO-IAPB, 1999) is the global framework within which NPCBVI operates, targeting elimination of avoidable blindness by 2020 and continuing under its successor framework.
The IMG's role in a cataract camp:
- Community screening and outreach: Before the camp day, the IMG may participate in outreach screening at a primary health centre or rural school — using the torch (pen torch + direct ophthalmoscope) to assess visual acuity, screen for red reflex, and identify patients with likely cataract for referral to the camp. This is high-yield simple screening: the Snellen chart (or the E chart for illiterate patients) + torch examination identifies >90% of visually significant cataract.
- Patient selection and triage at the camp: On the camp day, the IMG assists in verifying which patients meet surgical criteria (VA <6/18 in the better eye from cataract; systemic fitness for surgery), which need further workup (diabetics with fundal disease, uncontrolled BP), and which need referral for non-cataract conditions (glaucoma, retinal disease).
- Pre-operative and post-operative roles at camp: Same as hospital — mydriatics, systemic checks, consent, post-op drops prescription. In camp settings these are often compressed into a tight timetable; efficient, focused execution is essential.
- Patient communication in a culturally sensitive setting: At rural camps, patients may be elderly, illiterate, and deeply afraid of surgery. The IMG's ability to communicate clearly in the local language, address cultural misconceptions about 'eye operations causing blindness,' and deliver post-operative instructions in simple, concrete terms (demonstrated drop instillation, written instructions in the local script) is a clinical communication skill of high practical value.
- Follow-up coordination: At a camp, post-operative follow-up is the weak link — patients travel far and may not return for the day-1 check. The IMG can help by ensuring every patient has a specific follow-up appointment, a contact number to call if red flags develop, and that the local primary health centre is briefed on endophthalmitis red flags for camp patients.
SELF-CHECK
At a rural cataract camp, which of the following is the MOST important reason for performing a B-scan ultrasonography on a patient with a mature cataract before listing them for surgery?
A. To measure the axial length for IOL power calculation
B. To rule out retinal detachment or posterior segment pathology that would limit visual recovery
C. To assess the corneal endothelial cell density
D. To diagnose coexisting glaucoma
Reveal Answer
Answer: B. To rule out retinal detachment or posterior segment pathology that would limit visual recovery
In a patient with a mature cataract, the fundus cannot be visualised because no light passes through the opaque lens. B-scan ultrasonography is mandatory to detect retinal detachment, vitreous haemorrhage, or other posterior segment pathology before surgery — if the retina is detached, successful cataract surgery will not restore vision, and the patient must be counselled accordingly. Axial length measurement uses optical biometry (IOL Master) or immersion A-scan, not B-scan. Corneal endothelial cell density is measured by specular microscopy. Glaucoma assessment uses tonometry and optic disc examination (possible in immature cataract but not mature).
Self-Assessment — IMG Participation in Cataract Surgery
Self-assessment in this practical skills SDL requires you to think as an active team member in the cataract surgical setting, not as a passive observer. The questions below test your understanding of the IMG's specific responsibilities at each stage — pre-operative, intraoperative, post-operative, and community — and your ability to respond to the clinical challenges that arise in each phase. Work through each question independently before consulting the SDL content; the goal is to surface gaps in your knowledge so you can address them during your clinical posting. Competency in team participation is assessed in OSCE stations through structured observation checklists and scenario-based questioning, so the ability to articulate what you would do and why is as important as knowing the facts.
Scenario-Based Questions:
- You are the intern assigned to the cataract list. The first patient arrives in the pre-operative bay. Describe, in sequence, all tasks you need to complete before the patient enters the theatre, including the rationale for each step and the threshold values you would act on (e.g., what BP would prompt you to inform the surgeon?).
- During a cataract surgery you are observing, the surgeon calls out "posterior capsule rupture." What does this mean anatomically? What are the immediate surgical implications? What change in post-operative care should you anticipate for this patient?
- A post-operative patient on day 2 returns complaining of pain and redness. On your examination, visual acuity has dropped from the 6/9 measured at discharge to 6/60, and there is a white layer at the bottom of the anterior chamber. (a) Name this sign. (b) What is the diagnosis? (c) What is your immediate action?
- Describe the NPCBVI programme and the National Blindness Control Programme in India. What are the targets of the current phase? How does cataract surgical rate (CSR) relate to blindness prevalence, and what is the current CSR target for India?
- At a cataract camp, you are asked to counsel a patient being listed for surgery. The patient says: "My neighbour had this operation and can see perfectly, but my son says I should not risk it." Structure a counselling response that addresses the patient's fear, explains the benefits and realistic risks, and supports informed decision-making without coercion.