Page 5 of 23
OP9.2 | Diabetic Retinopathy — SDL Guide
Learning Objectives
- Describe the etiopathogenesis of diabetic retinopathy including the role of hyperglycaemia, pericyte loss, and VEGF in the progression from NPDR to PDR
- Classify diabetic retinopathy into non-proliferative (NPDR) and proliferative (PDR) stages with their specific fundoscopic features
- Distinguish clinically significant macular oedema (CSME) from other stages and explain its importance as the leading cause of visual loss
- Describe the stage-appropriate management of diabetic retinopathy: systemic control, focal laser, pan-retinal photocoagulation, anti-VEGF, and vitrectomy
- Describe the screening protocol for diabetic retinopathy including timing, method, and referral criteria
INSTRUCTIONS
Diabetic retinopathy is the leading cause of preventable blindness in working-age adults in India and worldwide. What makes it especially dangerous is its silence: patients lose retinal function for years without symptoms, and by the time vision blurs, irreversible damage may already be done. This module teaches you to classify retinopathy stages precisely, understand the biology driving progression, and act correctly at each stage — including when to screen, when to refer, and what treatment achieves.
References
- Khurana AK. Comprehensive Ophthalmology, 7th ed. Chapter on Diabetic Eye Disease (textbook)
- Parsons' Diseases of the Eye, 22nd ed. Chapter on Diabetic Retinopathy (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 40-year-old software engineer with a 12-year history of type 2 diabetes presents for a routine check-up. His glycaemic control has been 'okay — HbA1c around 8.5%.' He insists he sees perfectly. On dilated fundoscopy, you find: multiple microaneurysms, several dot-blot haemorrhages in all four quadrants, venous beading in one quadrant, and intraretinal microvascular abnormalities (IRMA) in two quadrants. No neovascularisation. This is severe NPDR — the 4-2-1 rule is met — and without intervention he has approximately a 50% chance of progressing to vision-threatening proliferative disease within 12 months. He felt nothing. You may be the only person who catches this.
WHY THIS MATTERS
Diabetic retinopathy affects approximately one in three people with diabetes worldwide and is the leading cause of new cases of blindness among working-age adults in India. With over 77 million people living with diabetes in India (IDF 2021), the scale of the problem is immense. The tragedy of diabetic retinopathy is that the most vision-threatening stages — severe NPDR and early PDR — are detectable on fundoscopy before any vision is lost, and timely intervention with pan-retinal photocoagulation and anti-VEGF therapy can prevent most blindness. As a clinician in any setting, you will encounter diabetic patients who need fundoscopy performed or arranged — understanding the stages and what each requires of you is essential for preventing a largely preventable cause of blindness.
RECALL
Recall the retinal vascular anatomy from the ophthalmoscopy SDL: the central retinal artery supplies the inner retinal layers, forming capillary networks between the arterioles and venules; the central retinal vein drains them. The capillary wall consists of endothelial cells and surrounding pericytes (contractile mural cells that regulate capillary tone and integrity). Pericytes are uniquely vulnerable to hyperglycaemia. Also recall from physiology: hyperglycaemia drives several pathological pathways — the polyol pathway (sorbitol accumulation), protein kinase C (PKC) activation, advanced glycation end-products (AGEs), and oxidative stress — all converging to injure the microvasculature. Finally recall VEGF (vascular endothelial growth factor): released by ischaemic tissue, it is the master driver of neovascularisation and the target of modern anti-VEGF therapies.
Presentation: How Diabetic Retinopathy Comes to Attention
Understanding the clinical presentation of diabetic retinopathy requires appreciating a fundamental and dangerous truth: the disease is asymptomatic in its most actionable early stages. This is why active screening by the clinician — not patient-reported symptoms — is the principal detection strategy.
In early and moderate NPDR, patients typically report no visual disturbance whatsoever. Microaneurysms, dot haemorrhages, and even hard exudates can be present in large numbers without the patient noticing any change in vision, because the macula is initially spared. The disease proceeds silently for years. The period of asymptomatic disease can span a decade or more in Type 2 DM, during which the retina accumulates progressive vascular injury. Each year without fundoscopy is an opportunity missed: microaneurysms progressing to haemorrhages, hard exudates tracking toward the fovea, and neovascularisation establishing a foothold that will eventually rupture into the vitreous. This natural history — predictable, gradual, and largely preventable — is what the screening programme is designed to interrupt.
Visual symptoms appear when the macula becomes involved:
- Blurred or distorted central vision — due to clinically significant macular oedema (CSME), which can develop at any stage of retinopathy (even mild NPDR). Patients may notice difficulty reading or recognising faces.
- Floaters — due to small vitreous haemorrhages from fragile new vessels in PDR; patients describe 'black spots', 'cobwebs', or a 'shower of dots' in vision.
- Sudden painless loss of vision — due to a large vitreous haemorrhage (blood filling the vitreous cavity) or tractional retinal detachment, both complications of advanced PDR.
On examination, the eye is typically white and quiet (no redness, no injection) — unlike acute glaucoma or uveitis. Visual acuity may be normal even with moderate NPDR, but reduced when CSME or advanced PDR is present. The critical examination is dilated fundoscopy, which is the definitive diagnostic tool.
Key point: a diabetic patient who says 'my vision is fine' may still have severe NPDR or early PDR. Never use symptom-absence as a reason to defer fundoscopy.
Pathogenesis: How Diabetes Damages the Retinal Vasculature
The pathogenesis of diabetic retinopathy is fundamentally a disease of the retinal microvasculature, driven by chronic hyperglycaemia and amplified by hypertension, dyslipidaemia, and duration of diabetes. The sequence from hyperglycaemia to blindness follows a logical molecular cascade that explains every clinical finding you will see on fundoscopy.
The first and most critical cellular event is selective loss of pericytes from retinal capillaries. Pericytes — the contractile mural cells wrapped around capillary walls — are exceptionally sensitive to hyperglycaemia-induced damage through the polyol pathway, PKC activation, and AGE accumulation. When pericytes are lost, the endothelial cell population is left unsupported, and the capillary wall becomes weak and abnormally permeable.
This produces two simultaneous and diverging processes:
Pathway 1 — Vascular leakage: Weak, pericyte-depleted capillary walls develop focal outpouchings called microaneurysms — the earliest detectable sign of DR. These microaneurysms leak plasma proteins and lipids into the surrounding retinal tissue, forming hard exudates (sharp-bordered yellow lipid-protein deposits in the outer retinal layers). Fluid accumulation in the macula — diabetic macular oedema (DME) — is the consequence of this leakage pathway and is clinically defined as CSME when it meets the ETDRS criteria for proximity to the foveal centre.
Pathway 2 — Capillary occlusion and ischaemia: As disease progresses, damaged capillaries become occluded (non-perfused). This creates areas of retinal ischaemia, clinically visible as cotton-wool spots (infarcts of the nerve fibre layer). The ischaemic retina releases VEGF (vascular endothelial growth factor) in large quantities. VEGF is the key driver of the proliferative phase: it stimulates neovascularisation — the growth of new but structurally abnormal, fragile blood vessels on the disc (NVD) and elsewhere on the retina (NVE).
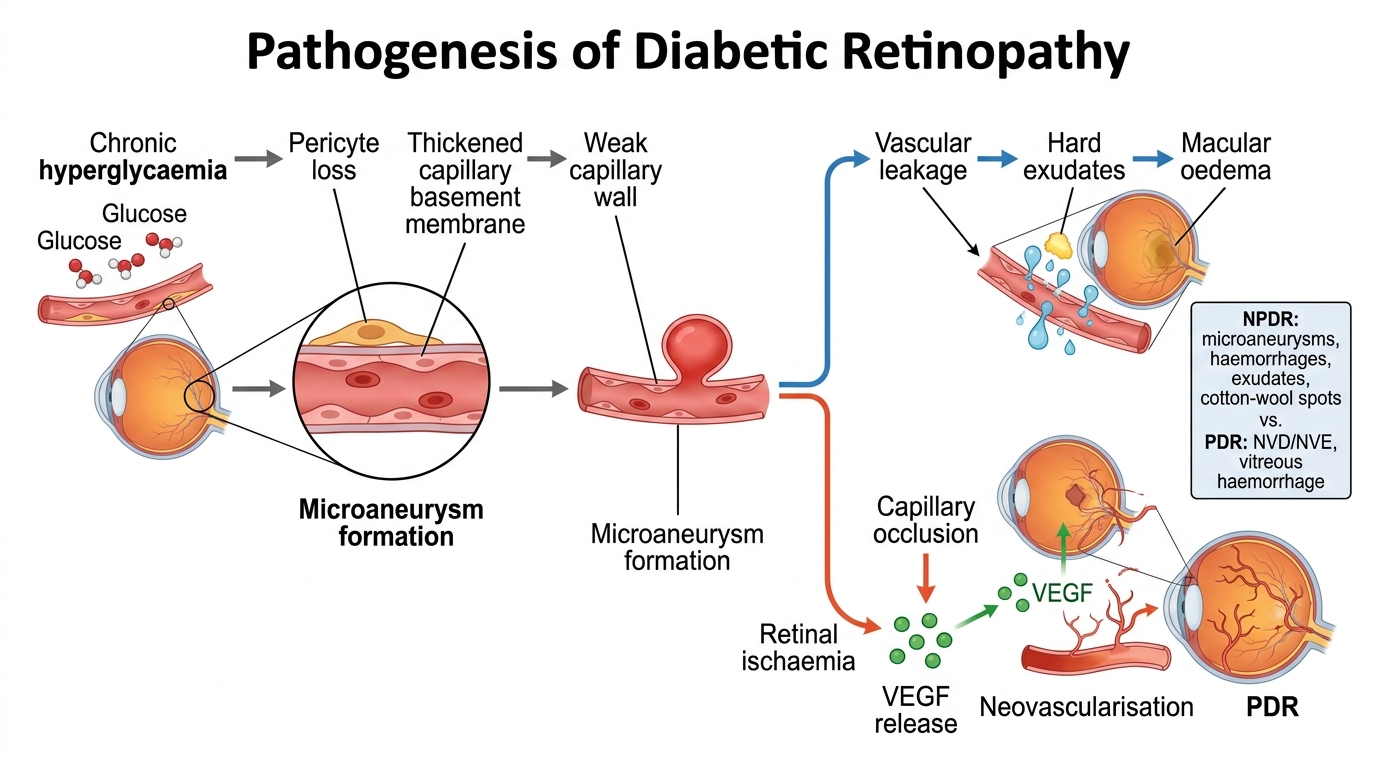
Pathogenesis of Diabetic Retinopathy
Risk factors that accelerate progression: duration of diabetes (most important single factor), poor glycaemic control (HbA1c >7%), hypertension (directly damages retinal vessels), dyslipidaemia (worsens hard exudate formation), renal disease, pregnancy (DR can worsen rapidly), and anaemia.
Clinical Classification: NPDR, PDR, and Macular Oedema
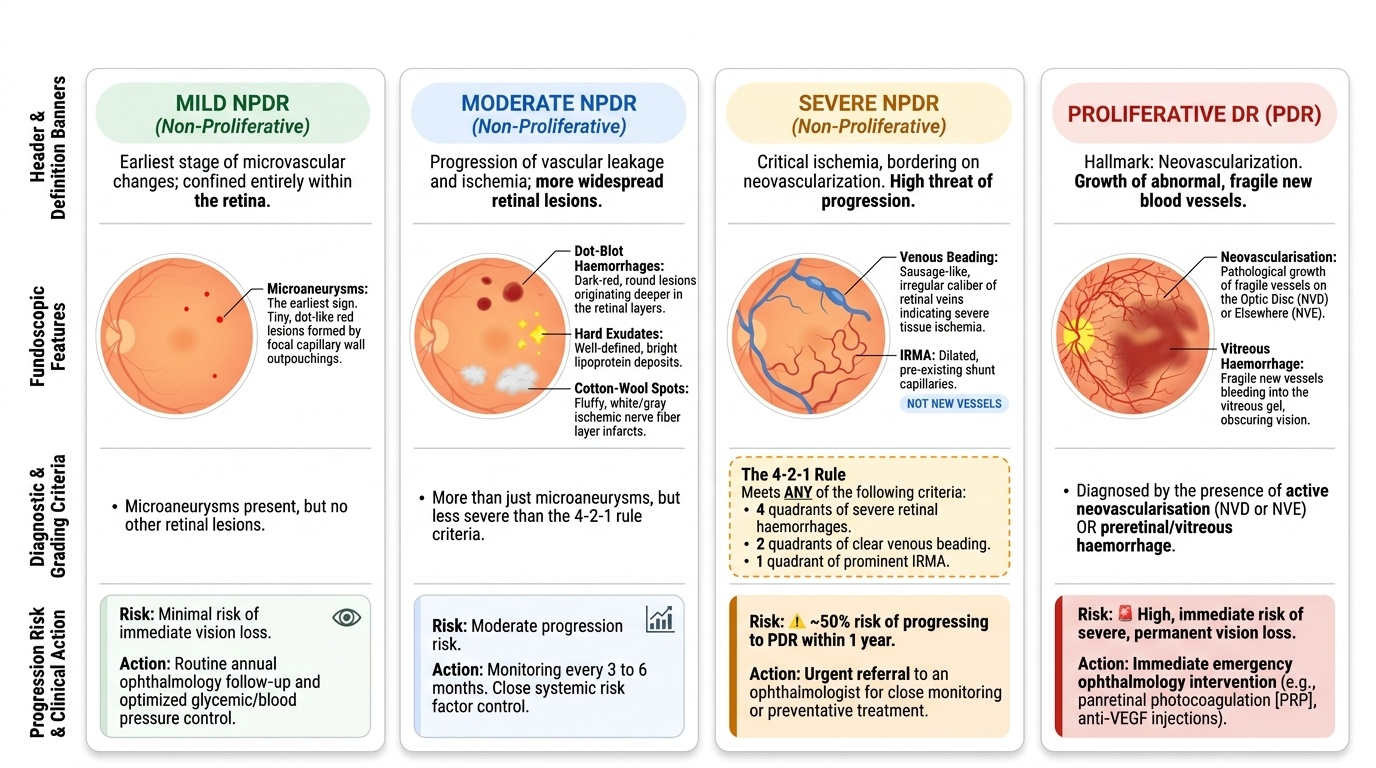
The classification of diabetic retinopathy is the most clinically critical aspect of this SDL — it determines treatment and referral urgency. The two major categories — NPDR and PDR — must be kept rigorously separate in your mind, as their defining features are completely distinct. The NPDR vs PDR distinction is one of the highest-yield ophthalmology examination points and one of the most common sources of clinical error.
Provided image
NON-PROLIFERATIVE DIABETIC RETINOPATHY (NPDR) is defined by the absence of neovascularisation. All NPDR findings represent changes within the existing retinal vasculature — leakage, microaneurysm formation, and ischaemia. NPDR features include: microaneurysms (earliest sign — tiny dot-like red lesions from focal capillary wall outpouchings), dot-blot haemorrhages (round, dark-red lesions from haemorrhage within retinal layers), hard exudates (bright yellow, well-defined lipoprotein deposits), cotton-wool spots (white fluffy ischaemic nerve fibre layer infarcts), intraretinal microvascular abnormalities (IRMA) (dilated, pre-existing capillaries shunting blood around occluded areas — NOT new vessels), and venous beading (sausage-like irregular calibre of veins, indicating severe ischaemia).
NPDR is graded mild → moderate → severe (4-2-1 rule): haemorrhages in 4 quadrants, OR venous beading in 2 quadrants, OR IRMA in 1 quadrant. Severe NPDR carries approximately 50% risk of progression to PDR within 12 months without treatment.
PROLIFERATIVE DIABETIC RETINOPATHY (PDR) is defined by the presence of neovascularisation: growth of new, fragile blood vessels driven by VEGF from ischaemic retina. These new vessels grow on the retinal surface and into the vitreous. PDR features: neovascularisation on the disc (NVD) — new vessels on or within 1 disc diameter of the optic disc, and neovascularisation elsewhere (NVE) — on peripheral retina or retinal surface. PDR complications arise from these fragile vessels: vitreous haemorrhage (bleeding of NVD/NVE into the vitreous — sudden painless vision loss), pre-retinal haemorrhage (boat-shaped blood between retina and vitreous face), and tractional retinal detachment (fibrovascular scar tissue from organised haemorrhage pulls the retina off the RPE).
CLINICALLY SIGNIFICANT MACULAR OEDEMA (CSME) can occur at any stage — NPDR or PDR. It is defined by the ETDRS criteria: (1) retinal thickening within 500 microns of the foveal centre, (2) hard exudates within 500 microns of the foveal centre with adjacent thickening, or (3) a zone of thickening ≥1 disc area within 1 disc diameter of the foveal centre. CSME is the leading cause of visual loss in diabetic retinopathy — not PDR, not vitreous haemorrhage — because it directly involves the fovea and degrades central vision. Modern terminology uses centre-involved DME (CI-DME) for oedema involving the foveal centre as detected on OCT.
SELF-CHECK
A diabetic patient's fundoscopy shows: multiple microaneurysms, dot-blot haemorrhages in all four retinal quadrants, and a frond of new vessels arising from the optic disc. Which stage of diabetic retinopathy is present, and what is the immediate management priority?
A. Severe NPDR — improve glycaemic control and review in 6 months
B. PDR (neovascularisation on disc, NVD) — urgent referral for pan-retinal photocoagulation (PRP) or anti-VEGF
C. Moderate NPDR with CSME — focal laser to the macula
D. Mild NPDR — no treatment required; annual review
Reveal Answer
Answer: B. PDR (neovascularisation on disc, NVD) — urgent referral for pan-retinal photocoagulation (PRP) or anti-VEGF
New vessels on the disc (NVD) define PDR — the presence of neovascularisation is the defining criterion that distinguishes PDR from NPDR, regardless of the presence of NPDR features (microaneurysms, haemorrhages). PDR is sight-threatening and requires urgent ophthalmological referral for pan-retinal photocoagulation (PRP) and/or intravitreal anti-VEGF therapy. Option A is wrong because NVD is not an NPDR feature. Option C refers to macular oedema management, which is not the immediate priority here. Option D (mild NPDR) does not apply — PDR is present.