Page 13 of 23
OP9.4 | Posterior Segment Disorder Survey: Retinopathies, Detachment, Macular Disease, Dystrophy and Retinoblastoma — SDL Guide (Part 2)
Hypertensive Retinopathy and Vascular Retinopathies: Eales and ROP
These three conditions — hypertensive retinopathy, Eales disease, and retinopathy of prematurity (ROP) — share the unifying mechanism of retinal vascular injury, but they differ markedly in their underlying cause, the population they affect, the clinical urgency they demand, and the management they require. Hypertensive retinopathy reflects the chronic mechanical and haemodynamic stress of sustained systemic hypertension on the small arterioles of the retina, making it one of the most common incidental findings on fundoscopy in adult medicine. Eales disease is an idiopathic peripheral obliterative periphlebitis seen predominantly in young Indian males and is notable for its association with tuberculin hypersensitivity. Retinopathy of prematurity is a developmental vasoproliferative disorder unique to premature neonates, caused by dysregulation of retinal vascular growth in the context of supplemental oxygen therapy. Together, they illustrate how the retinal vasculature acts as a window into systemic and developmental disease, responding to insults with a limited repertoire of structural changes — narrowing, sheathing, haemorrhage, neovascularisation — that the clinician must learn to recognise and grade.
Provided image
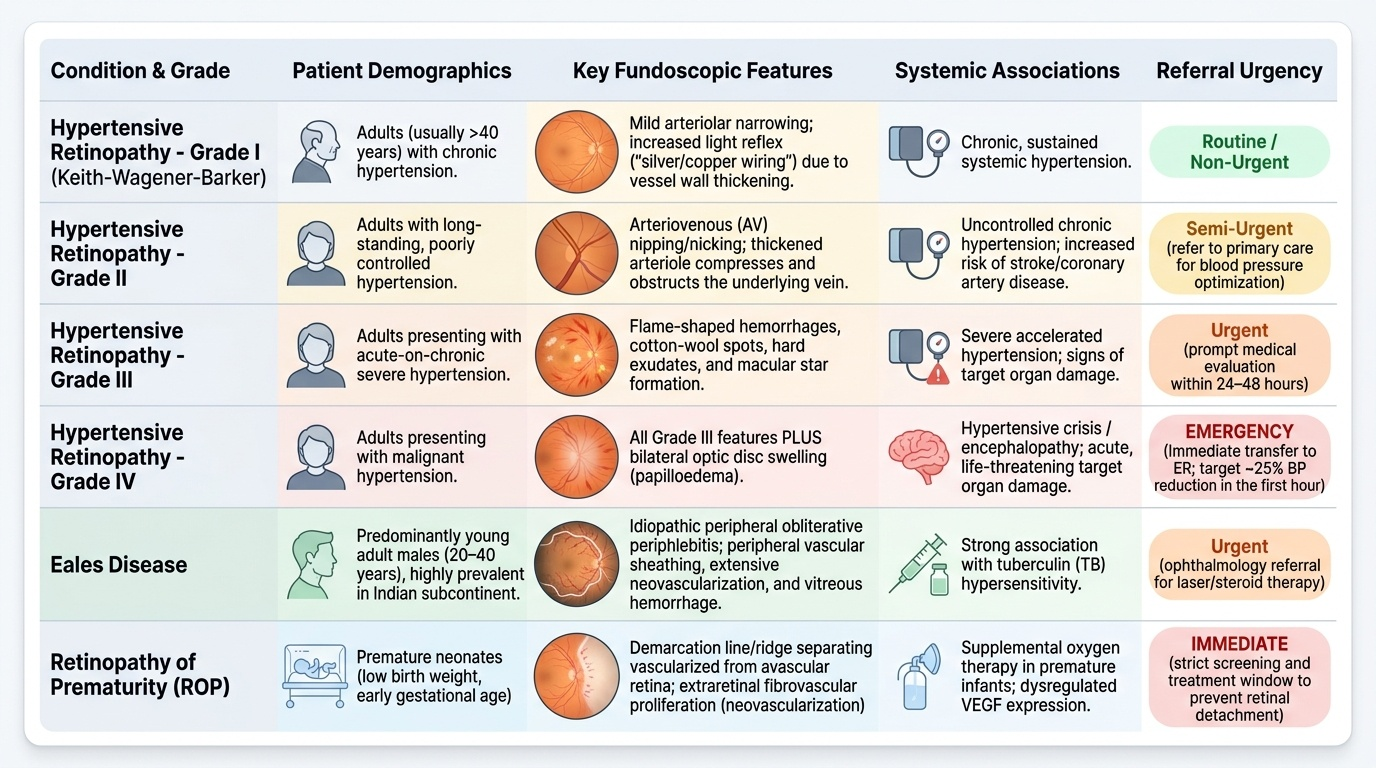
Hypertensive retinopathy (Keith-Wagener-Barker classification):
- Grade I: mild arteriolar narrowing and increased light reflex ('silver/copper wiring'). The arterioles are thickened and their normal orange reflex changes to a copper or silver sheen.
- Grade II: AV nipping (nicking) — arteriovenous crossing changes where a thickened arteriole compresses the underlying vein, causing apparent kinking or 'nipping'. The vein appears to taper and vanish at the crossing point.
- Grade III: haemorrhages (flame-shaped, superficial), hard exudates, and cotton-wool spots appearing in addition to grades I-II changes. Hard exudates may form a macular star (radiating pattern along Henle's fibres).
- Grade IV: all of grade III plus papilloedema (bilateral disc swelling). Grade IV indicates hypertensive encephalopathy — a medical emergency requiring immediate BP reduction (avoid excessive or rapid lowering; target ~25% reduction in first hour). Vision may be normal initially despite papilloedema.
Eales disease: an idiopathic peripheral obliterative periphlebitis predominantly affecting young Indian males aged 20-40 years (though seen globally). The aetiology is debated; an association with tuberculin hypersensitivity has been proposed. The clinical course passes through three stages: active periphlebitis (sheathed peripheral veins, visible through indirect ophthalmoscopy), ischaemia and neovascularisation (peripheral NVE from VEGF), and recurrent vitreous haemorrhage from ruptured NVE. Management: laser photocoagulation to ischaemic areas (sector PRP); vitrectomy for non-clearing haemorrhage; corticosteroids in the active inflammatory phase; rule out ocular tuberculosis with Mantoux and chest X-ray.
Retinopathy of Prematurity (ROP): a vasoproliferative disorder of the developing retinal vasculature in premature infants, caused by oxygen disruption during the normal progression of retinal vascularisation from the disc toward the periphery. Classification: by zone (I = most posterior, surrounding optic disc; II = mid-periphery; III = anterior/peripheral) and stage (1 = flat demarcation line, 2 = ridge, 3 = ridge with extraretinal neovascularisation, 4 = partial retinal detachment, 5 = total retinal detachment). Plus disease = dilation and tortuosity of posterior retinal vessels, indicating advanced disease. Treatment is indicated for Type 1 ROP (per ET-ROP criteria): any stage with plus disease in zone I; stage 3 without plus in zone I; stage 2 or 3 with plus disease in zone II. Treatment options: retinal laser photocoagulation (to avascular zone, destroying the source of VEGF) or intravitreal anti-VEGF (bevacizumab 0.625 mg — particularly for zone I disease). Screening: all infants <32 weeks or <1500 g birth weight; ophthalmologist examines from 31-32 weeks postmenstrual age.
Retinal Detachment: Types, Presentation, and Management
Retinal detachment is the separation of the neurosensory retina from the underlying retinal pigment epithelium. It is a surgical emergency when vision is threatened, particularly when the macula is involved or at risk. The three types arise through completely different mechanisms and require different surgical approaches.
Rhegmatogenous retinal detachment (RRD) — the most common type — occurs when a break (tear or hole) in the retina allows vitreous fluid to pass beneath and accumulate in the subretinal space. The most common cause is posterior vitreous detachment (PVD): as the vitreous gel liquefies and separates with age, it can exert traction on the retina at points of firm attachment, causing a U-shaped (horseshoe) tear at the flap's apex. Liquefied vitreous then flows through the tear and progressively detaches the retina. Predisposing factors: myopia (longer axial length, peripheral lattice degeneration), previous eye surgery, trauma, and family history.
Fundoscopy: the detached retina appears grey, elevated, and undulates with eye movement ('corrugated' appearance). Shafer's sign (tobacco dust — pigment granules floating in the vitreous) is highly suggestive of a retinal tear. The subretinal fluid shifts with changes in head position (gravity-dependent).
Management: any RRD requires urgent surgical repair. Pneumatic retinopexy (gas bubble + laser/cryotherapy for superior breaks), scleral buckling (silicone band indenting the scleral wall to close breaks), and pars plana vitrectomy (PPV with gas or silicone oil tamponade) are the three main approaches, chosen based on break location and extent of detachment. If the macula is not yet detached ('macula-on RRD'), surgery is performed within 24 hours — visual outcome is excellent. If the macula has detached ('macula-off'), surgery within 1 week yields better outcomes than delayed repair.
Tractional retinal detachment (TRD): fibrovascular membranes — from PDR, ROP stage 4-5, penetrating trauma, or proliferative vitreoretinopathy (PVR) — contract and mechanically pull the retina off the RPE. The detachment is typically concave, localised, and does not extend to the ora serrata. Management: pars plana vitrectomy with membrane peeling.
Exudative (serous) retinal detachment: sub-retinal fluid accumulates from choroidal disease (tumour, severe hypertension, posterior scleritis, Vogt-Koyanagi-Harada syndrome) without any retinal break. The detachment is smooth-domed, shifting with gravity, and the subretinal fluid shifts dramatically with position (bullous). Management: treat the underlying cause.
SELF-CHECK
A 55-year-old myopic man presents with sudden onset of floaters and a dark 'curtain' encroaching from the left side of his left visual field, starting this morning. On fundoscopy you see a grey, elevated, undulating retina in the temporal periphery. Tobacco-dust cells are visible in the anterior vitreous. What is the diagnosis and the immediate management?
A. Posterior vitreous detachment — reassure; floaters are benign
B. Rhegmatogenous retinal detachment — urgent surgical referral within hours (macula-on RRD)
C. Central retinal vein occlusion — blood-and-thunder fundus consistent with CRVO
D. Tractional retinal detachment from proliferative diabetic retinopathy
Reveal Answer
Answer: B. Rhegmatogenous retinal detachment — urgent surgical referral within hours (macula-on RRD)
Grey elevated undulating retina with a shadow/curtain in the visual field and tobacco-dust (Shafer's sign) in the vitreous is rhegmatogenous retinal detachment (RRD) — the break has allowed fluid behind the retina. This is a macula-on RRD (the curtain is approaching from the side, macula not yet involved), which is a surgical emergency: repair within 24 hours is the target to preserve macular function. Simple PVD causes floaters but no visual field defect and no retinal elevation. CRVO and DR-tractional RD do not match this fundoscopic pattern.
Macular Diseases: CSR, CMO, and AMD
The macula — the central 5 mm of retina — is the site of the most functionally significant pathology because it controls central and colour vision. Three important macular conditions merit systematic study: central serous retinopathy, cystoid macular oedema, and age-related macular degeneration.
Provided image
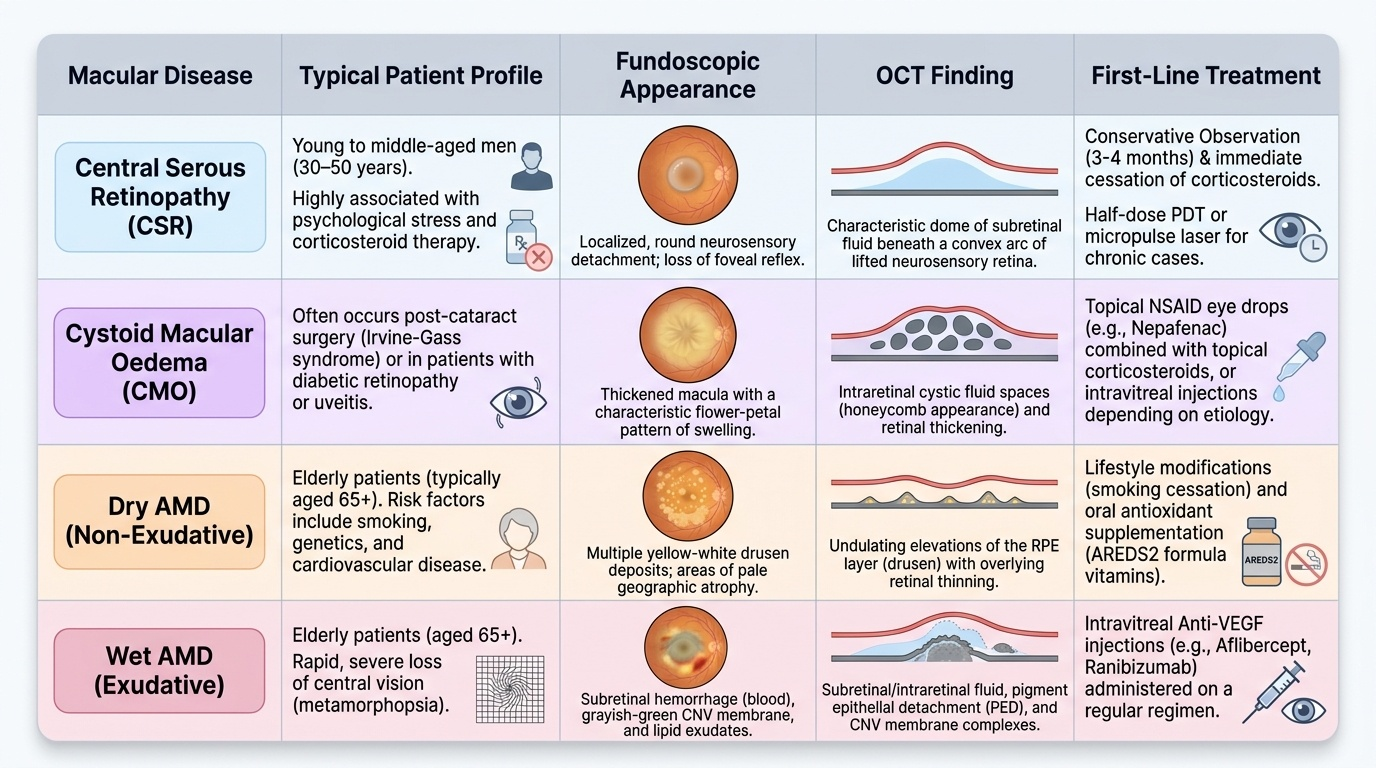
Central Serous Retinopathy (CSR): a condition characterised by a serous (fluid-filled) neurosensory detachment of the macula from the RPE, caused by a localised defect in the RPE barrier that allows fluid from the choriocapillaris to accumulate beneath the retina. The condition affects predominantly young to middle-aged men (30-50 years), particularly those under psychological stress, and those on corticosteroid therapy (corticosteroids are a strong risk factor). Patients present with sudden central visual blur, reduced acuity, and metamorphopsia (distortion of straight lines, as the neurosensory retina is lifted and the photoreceptors are displaced). On OCT, there is a characteristic dome of subretinal fluid beneath a convex arc of lifted neurosensory retina. FFA shows the classic 'smokestack' or 'inkblot' pattern of fluorescein leakage at the RPE defect.
Management: most acute CSR episodes (especially the first) resolve spontaneously within 3-4 months — conservative management with observation is appropriate initially. The patient must stop any corticosteroids. If the episode is chronic (>4 months), or recurrent, treatment with half-dose photodynamic therapy (PDT) or micropulse laser to the RPE leakage site is effective.
Cystoid Macular Oedema (CMO): accumulation of fluid in cyst-like spaces within the inner nuclear and outer plexiform layers of the macula, typically in a petaloid pattern around the fovea on FFA. CMO is not a primary disease but a response to multiple triggers: post-operative CMO (Irvine-Gass syndrome — commonest after cataract surgery, resolves spontaneously in most cases), uveitis-related CMO, diabetic macular oedema, vein occlusion-related oedema, and retinitis pigmentosa-associated CMO. OCT is the gold standard for diagnosis and monitoring. Management depends on cause: topical NSAIDs and steroids for post-operative CMO; intravitreal anti-VEGF or steroid for uveitic and vascular CMO.
Age-Related Macular Degeneration (AMD): the leading cause of irreversible blindness in patients over 60 years in developed countries. AMD is classified into two forms:
Dry (non-neovascular) AMD: characterised by the accumulation of drusen — small yellow-white extracellular deposits beneath the RPE — and progressive geographic RPE atrophy. Drusen appear on fundoscopy as yellow-white spots of varying sizes; large soft drusen carry the highest risk of progression to wet AMD. Visual loss in dry AMD is gradual, central, and associated with scotoma, but rarely total. There is currently no proven pharmacological treatment; the AREDS2 formula (vitamins C, E, zinc, copper, lutein, zeaxanthin) reduces the risk of progression in intermediate AMD.
Wet (neovascular) AMD: choroidal neovascularisation (CNV) — invasion of new blood vessels from the choroid through Bruch's membrane into the sub-RPE or subretinal space. These vessels leak, bleed, and form a fibrovascular disciform scar. Visual loss is more rapid and more severe than in dry AMD. Fundoscopy in wet AMD: subretinal haemorrhage, greyish subretinal membrane (the CNV), hard exudates, and (on FFA) classic or occult CNV patterns with early hyperfluorescence. Management: intravitreal anti-VEGF (ranibizumab, bevacizumab, aflibercept) is first-line and can preserve or improve vision if started promptly. Treatment must be maintained long-term (typically monthly injections initially, then treat-and-extend protocols).