Page 15 of 26
OR1.6 | Recent Advances in Orthopaedic Management — SDL Guide
Learning Objectives
- Describe recent advances in trauma orthopaedics including damage control orthopaedics and modern fixation strategies
- Outline developments in sports injury management including arthroscopic surgery and biological therapies
- Discuss advances in arthroplasty including minimally invasive techniques, bearing surfaces, and robotic assistance
- Describe current approaches to spine surgery including disc replacement, motion-preserving procedures, and minimally invasive spine surgery
- Critically evaluate the relevance of recent advances to clinical practice in the Indian healthcare context
INSTRUCTIONS
Orthopaedics is one of the most rapidly evolving surgical specialties. Techniques that were experimental a decade ago — arthroscopic ACL reconstruction, computer-assisted hip replacement, bone morphogenetic protein for non-union — are now standard of care. For a final-year student entering a field where evidence-based practice is constantly updated, knowing the direction of change is as important as knowing the current standard. This module surveys recent advances across the four domains identified in OR1.6: trauma, sports injuries, arthroplasty, and spine, with an emphasis on the principles behind the advances rather than the technical details.
References
- Maheshwari's Essential Orthopaedics, Chapter 25 — Recent Advances in Orthopaedics (textbook)
- Apley & Solomon's System of Orthopaedics and Trauma, Chapter 1 — Principles of Orthopaedic Surgery (textbook)
- Ebnezar's Textbook of Orthopaedics, Chapter 30 — Recent Advances (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
In 1980, a patient with a torn anterior cruciate ligament was told: 'Your knee will never be the same. Avoid sport.' Today, an arthroscopically reconstructed ACL allows elite athletes to return to competitive play within 9–12 months. In 1990, a complex tibial plateau fracture was managed with closed reduction and cast immobilisation. Today, computed tomography-guided pre-operative planning and locked plating restores anatomical articular reduction. In 2000, a patient with end-stage hip arthritis waited years for a conventional metal-on-polyethylene replacement that would last 15 years. Today, ceramic-on-ceramic bearings and cementless fixation aim for 25–30 year implant survival. Orthopaedics moves fast. The question is not 'what was the standard last year' — it is 'why does this advance work, and does the evidence support adopting it?'
WHY THIS MATTERS
For a final-year student, fluency in recent advances serves three purposes. First, patients and their families frequently ask about 'newer' or 'better' options — you must be able to explain the evidence basis for recommending or deferring an advance. Second, the MBBS curriculum explicitly requires awareness of current developments (OR1.6) as part of competency in orthopaedics. Third, many of these advances are already standard practice in teaching hospitals — you will encounter them in your postings and need a conceptual framework to understand what you are observing. This module provides that framework across trauma, sports, arthroplasty, and spine.
RECALL
Before proceeding, briefly recall:
- Principles of fracture fixation: intramedullary nailing (load-sharing, central axis), plating (load-bearing, periosteal blood supply implications), external fixation (temporary stabilisation, damage control)
- Articular cartilage biology: hyaline cartilage has very limited intrinsic repair capacity; fibrocartilage (which fills cartilage defects spontaneously) is biomechanically inferior
- Bone biology: cortical versus cancellous bone; bone remodelling (Wolff's law); implant stress-shielding
- The concept of minimally invasive surgery (MIS): smaller incisions reduce soft tissue trauma, blood loss, and recovery time but require advanced equipment and learning curve
- Arthroscopy: keyhole joint surgery using a fibre-optic camera and instruments; transformative for knee, shoulder, hip, and ankle surgery
Orientation: The Principles Driving Orthopaedic Advances
Every major advance in orthopaedic surgery can be understood as a response to one or more of five fundamental clinical problems: (1) inadequate fixation strength leading to implant failure or non-union, (2) excessive surgical trauma causing blood loss, infection, and slow recovery, (3) limited implant longevity requiring revision surgery, (4) inability to restore normal anatomy precisely enough to prevent post-traumatic arthritis or re-injury, and (5) inadequate biological healing of bone, cartilage, and soft tissue. Framing advances within these problems helps students understand why they were developed and what evidence is needed to adopt them.
The overarching trend across all four domains — trauma, sports, arthroplasty, and spine — is convergence of three technologies: imaging (CT, MRI, intraoperative fluoroscopy, navigation systems), implant materials (titanium alloys, ceramics, bioabsorbable polymers, hydroxyapatite coatings), and biological agents (bone morphogenetic proteins, platelet-rich plasma, stem cells, synthetic bone substitutes). Each advance typically harnesses one or more of these in a new combination.
A critical thinking framework for evaluating any claimed advance has three questions:
1. What clinical problem does it solve? If the problem is rare, the advance is niche regardless of technical elegance.
2. What level of evidence supports it? A randomised controlled trial is more reliable than a case series. Industry-sponsored studies require critical appraisal.
3. Is it applicable in the Indian context? A $50,000 robotic arthroplasty system or an $800 bone morphogenetic protein vial may represent the gold standard internationally but remain inaccessible in district hospital practice. The skill lies in knowing the evidence and making appropriate adaptations.
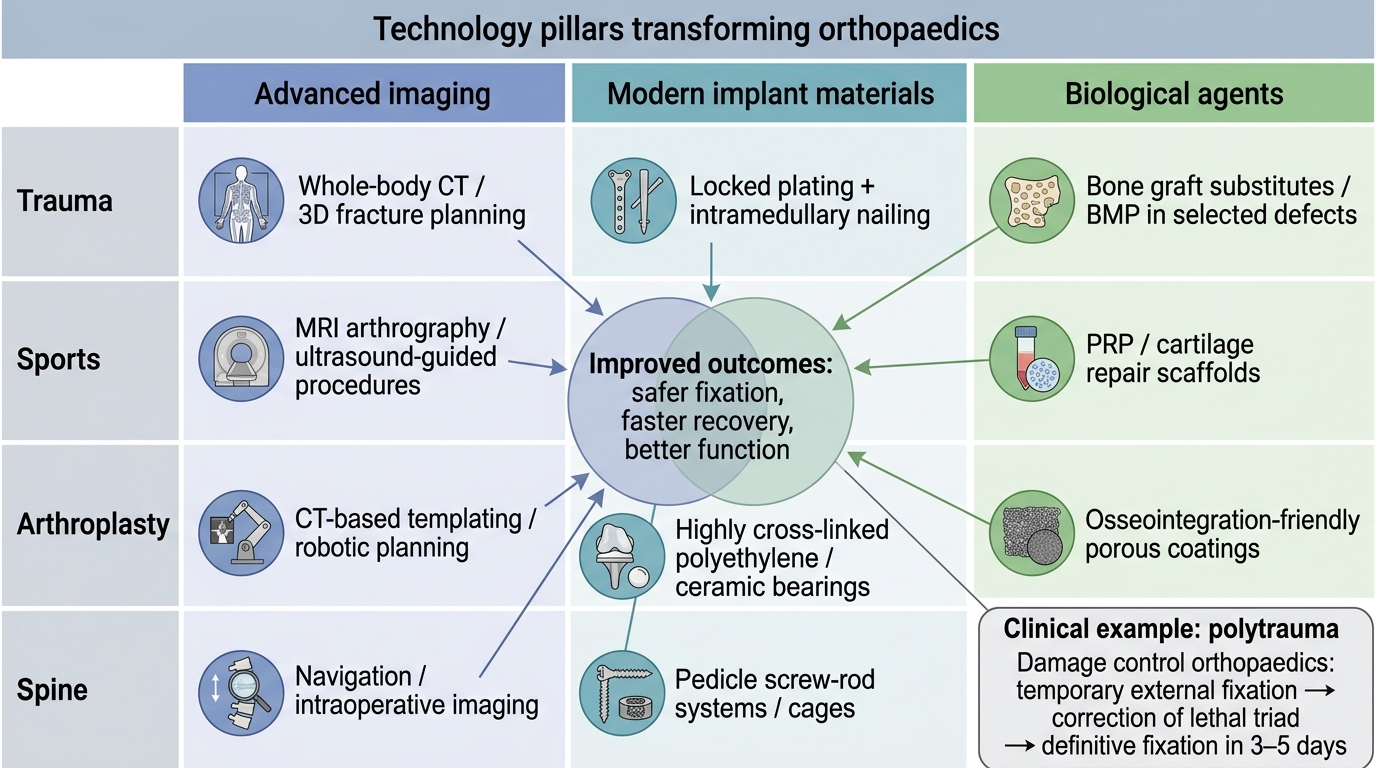
Technology Pillars Across Orthopaedic Domains
Advances in Trauma Orthopaedics
Trauma orthopaedics has been transformed by three advances: damage control orthopaedics (DCO), locked plating systems, and intramedullary nailing technology. These have collectively reduced mortality and improved functional outcomes for some of the most devastating injuries seen in orthopaedic practice, particularly high-energy polytrauma and peri-articular fractures.
Damage control orthopaedics (DCO) emerged from military trauma experience and the recognition that early total care (definitive fixation within 24 hours) of all fractures in a haemodynamically compromised polytrauma patient carries an unacceptable mortality risk. DCO stages management: temporary external fixation for long bone and pelvic fractures in the acute phase (restoring length, alignment, and stability without the physiological insult of prolonged intramedullary nailing), followed by definitive fixation (intramedullary nail, ORIF) in 3–5 days once the lethal triad has been corrected and the patient is physiologically optimised ('window of opportunity'). This staged approach has significantly reduced the rates of adult respiratory distress syndrome (ARDS), multi-organ failure, and mortality in high-ISS (injury severity score) patients.
Locked plating systems represent a paradigm shift in the surgical treatment of peri-articular fractures (distal femur, proximal tibia, proximal humerus, distal radius). In conventional plating, screws compress the plate to bone — the bone provides stability by friction. In locked plating, threaded screw heads lock into the plate, creating a fixed-angle device that does not rely on bone-plate friction. This allows stable fixation in osteoporotic bone (where conventional screws pull out), near articular surfaces where screw direction must be precisely controlled, and in comminuted fractures where compression plating is biomechanically impossible.
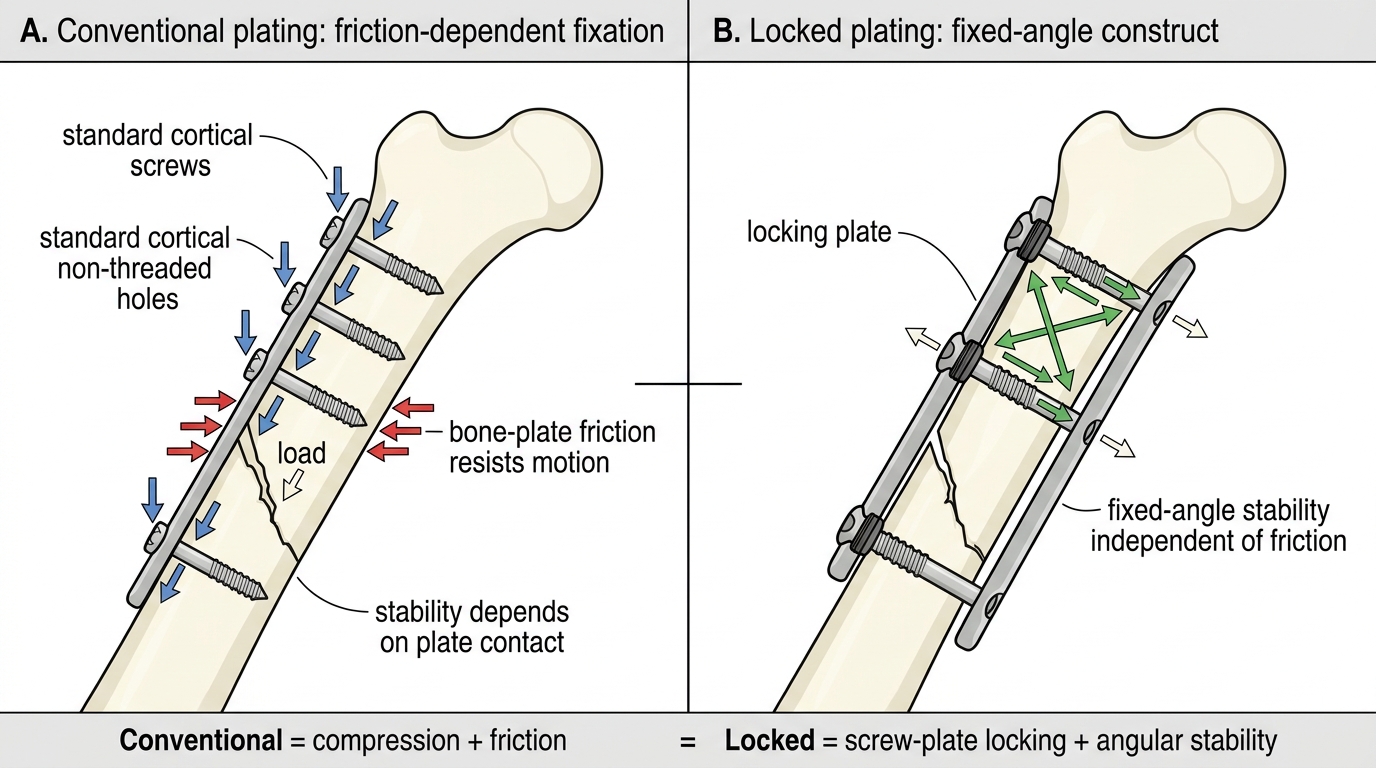
Conventional Versus Locked Plating Biomechanics
Intramedullary nailing advances include the development of nails for virtually every long bone (femur, tibia, humerus, radius-ulna, clavicle), interlocking screws that prevent rotation and shortening, and cephalomedullary nails for proximal femoral fractures (intertrochanteric and subtrochanteric fractures) that combine an intramedullary nail with a femoral neck screw, stabilising both the shaft and the femoral head with a single implant. Closed intramedullary nailing (without opening the fracture site) preserves the fracture haematoma, reduces infection risk, and accelerates healing by maintaining the biological environment.
Computer-assisted orthopaedic surgery (CAOS) and navigation use intraoperative CT or fluoroscopy data registered to the patient's anatomy, allowing the surgeon to plan screw trajectories and implant positions on a screen before drilling. This is particularly valuable for percutaneous iliosacral screw fixation in pelvic fractures and for pedicle screw placement in spine surgery, where misdirected screws can injure the spinal cord or pelvic vessels.
Advances in Sports Injury Management
Sports orthopaedics has been transformed by arthroscopy — the ability to visualise and treat joint pathology through small portals using a fibre-optic camera and purpose-built instruments. Arthroscopy replaced many open procedures that caused significant scarring, prolonged recovery, and complications from large incisions, and has enabled new reconstructive procedures that were not previously possible. The knee remains the most commonly arthroscoped joint in orthopaedics, but shoulder, hip, ankle, and elbow arthroscopy have all grown substantially.
Anterior cruciate ligament (ACL) reconstruction is one of the most evidence-based and performed orthopaedic procedures globally. The ACL cannot be primarily repaired (it does not heal due to poor intrinsic blood supply and hostile synovial fluid environment) and must be reconstructed using a graft. Options include:
- Bone-patellar tendon-bone (BPTB) autograft: the 'gold standard' for high-demand athletes; strong, reliable, good tunnel fixation, but donor site morbidity (anterior knee pain, patellar fracture risk)
- Hamstring tendon autograft (gracilis + semitendinosus, 4-strand): less donor site morbidity, widely used; requires cortical fixation
- Allograft: from cadaveric donors; used in multi-ligament reconstruction and in older, lower-demand patients; higher re-rupture rate in young athletes
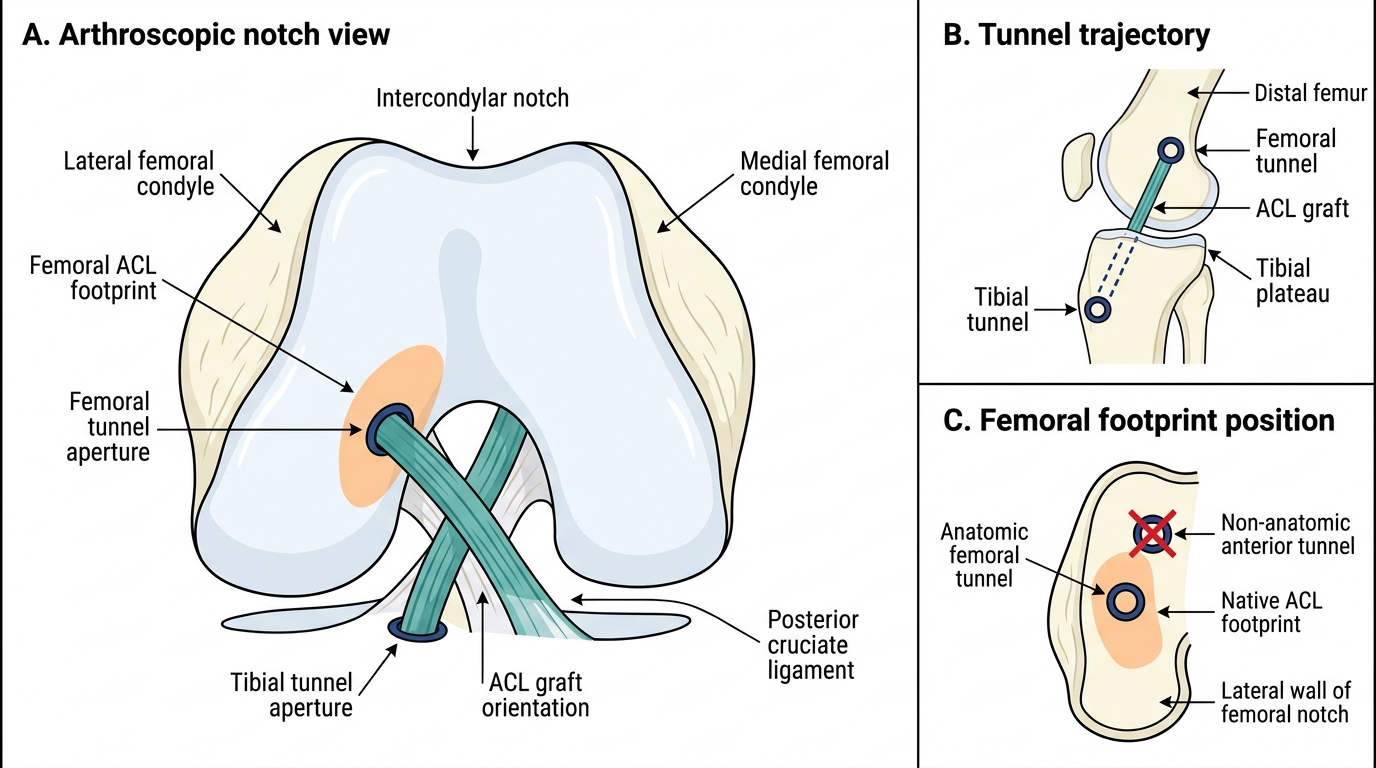
Arthroscopic ACL Graft Tunnel Placement
Meniscal surgery: The paradigm has shifted from 'remove the torn meniscus' (total meniscectomy — historically common, associated with accelerated osteoarthritis) to 'preserve as much meniscus as possible.' Partial meniscectomy (removing only the torn fragment) is the current standard for symptomatic irreparable tears. Meniscal repair (suturing the tear with arthroscopic suture devices) is preferred for peripheral, vascular zone tears in young patients, with healing rates of 85–90% for ideal candidates. Meniscal transplantation (cadaveric meniscus) is emerging for post-meniscectomy young patients with joint-line pain.
Biological therapies in sports orthopaedics:
- Platelet-rich plasma (PRP): concentrated autologous platelets containing growth factors (PDGF, TGF-β, VEGF) injected into tendinopathies (Achilles, patellar tendon, lateral epicondyle), cartilage defects, and ACL injuries. Evidence is heterogeneous — moderate benefit for lateral epicondylitis; evidence weaker for other indications.
- Bone morphogenetic protein (BMP): a family of growth factors that stimulate osteoblast differentiation and bone formation. BMP-2 and BMP-7 (rhBMP) are approved for use in specific clinical scenarios: BMP-2 in spinal fusion (anterior lumbar interbody fusion), BMP-7 in tibial non-union. Despite strong biological rationale, clinical trial results have been mixed and concerns about ectopic bone formation and cancer risk limit use.
- Stem cell therapy: mesenchymal stem cells (from bone marrow aspirate or adipose tissue) are being investigated for cartilage defect treatment, tendon healing, and AVN of the femoral head. Still largely experimental outside of clinical trials; not standard of care.
SELF-CHECK
A 28-year-old athlete undergoes ACL reconstruction using a bone-patellar tendon-bone autograft. His coach asks why a hamstring graft was not used instead. Which of the following best summarises the key trade-off between the two autograft options?
A. BPTB offers stronger initial fixation and proven performance in high-demand athletes but causes more donor-site morbidity (anterior knee pain); hamstring graft has less donor-site morbidity but requires reliable cortical fixation
B. Hamstring graft is always superior to BPTB because it avoids patellar fracture risk
C. BPTB is used only in elderly patients because of its superior bone-to-bone healing
D. Allograft is preferred over both autograft options in young competitive athletes because of lower re-rupture rate
Reveal Answer
Answer: A. BPTB offers stronger initial fixation and proven performance in high-demand athletes but causes more donor-site morbidity (anterior knee pain); hamstring graft has less donor-site morbidity but requires reliable cortical fixation
BPTB autograft is considered the gold standard for high-demand athletes because of its strong bone-to-bone healing in tunnels and its long-term track record. The main disadvantage is donor-site morbidity — anterior knee pain, kneeling discomfort, and a small risk of patellar fracture or patellar tendon rupture at the harvest site. Hamstring graft has less donor-site morbidity and is widely used, but requires cortical fixation devices. Allograft carries a higher re-rupture rate in young athletes and is generally avoided in this group.