Page 5 of 26
OR1.2 | Shock in Orthopaedic Trauma — SDL Guide
Learning Objectives
- Define shock and classify its four types relevant to orthopaedic trauma
- Describe the etiopathogenesis of haemorrhagic shock including the compensatory mechanisms and their failure
- Identify clinical features and ATLS haemorrhagic shock classes (I–IV) from examination findings
- Outline the principles of management of shock in the orthopaedic trauma patient including haemostatic resuscitation
- Recognise neurogenic shock and distinguish it from haemorrhagic shock in the trauma setting
INSTRUCTIONS
Shock is the final common pathway of many orthopaedic emergencies — a femur fracture that bleeds 1–2 litres into the thigh, a pelvic fracture that haemorrhages into the retroperitoneum, a spinal cord injury that loses sympathetic vascular tone. Failing to recognise and treat shock promptly is a leading cause of preventable trauma death. This module gives you a mechanistic understanding of shock pathophysiology, teaches you to classify shock severity from bedside findings alone, and anchors management decisions in the physiology rather than in memorised protocols.
References
- Maheshwari's Essential Orthopaedics, Chapter 1 — Trauma and its Management (textbook)
- Apley & Solomon's System of Orthopaedics and Trauma, Chapter 23 — Complications of Fractures (textbook)
- ATLS Student Course Manual, 10th edition — Chapter 3: Shock (guideline)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 22-year-old motorcyclist is brought in after a high-speed collision. His right femur is visibly deformed and he is drowsy. BP 96/70 mmHg, HR 118/min, RR 22/min. There is no open wound and no obvious source of external bleeding. A medical student beside you says, 'His blood pressure is almost normal — he should be fine for now.' You know this is wrong. You know that a compensated young man with a femur fracture can be harbouring 1.5 litres of blood in his thigh and that his cardiovascular system is working at its limits to maintain that 'almost normal' pressure. The question is: what will you do in the next five minutes before that compensation fails?
WHY THIS MATTERS
Shock is the most immediately reversible cause of preventable death in trauma. Unlike a severe brain injury or aortic transection, haemorrhagic shock is treatable — IF recognised early and managed correctly. The orthopaedic surgeon must understand shock not as a generic emergency medicine problem, but as a direct consequence of the skeletal injuries they treat: femoral shaft fractures, pelvic ring disruptions, and open fractures all carry specific haemorrhage profiles. Additionally, spinal cord injury produces a distinct form of shock (neurogenic) that can be confused with hypovolaemic shock and overtreated with fluids, worsening pulmonary oedema. Mastery of shock classification and management is therefore foundational to safe orthopaedic practice.
RECALL
Before proceeding, recall:
- The Frank-Starling mechanism: how cardiac output responds to changes in preload (venous return)
- The sympathetic nervous system response to hypotension: vasoconstriction, tachycardia, increased contractility
- The four determinants of cardiac output: heart rate, preload, afterload, contractility
- Oxygen delivery (DO₂) = cardiac output × arterial oxygen content (CaO₂)
- The ATLS haemorrhagic shock classes: roughly Class I (<15% blood volume), II (15–30%), III (30–40%), IV (>40%)
Definition and Classification of Shock
Shock is defined as inadequate tissue perfusion and oxygen delivery to meet the metabolic demands of cells. It is not simply hypotension — a patient can be in shock with a normal blood pressure if cardiac output and tissue oxygen delivery are severely compromised, and conversely, a patient can be transiently hypotensive without cellular-level ischaemia. The critical consequence of sustained shock is anaerobic metabolism → lactate accumulation → metabolic acidosis → multi-organ failure.
Four mechanisms of shock are relevant to the trauma patient and each requires a different management approach:
1. Hypovolaemic shock (most common in orthopaedic trauma): loss of intravascular volume from haemorrhage (haemorrhagic shock) or plasma loss (burns, crush injury). The entire management is directed at restoring intravascular volume while controlling the source of haemorrhage.
2. Distributive shock: peripheral vasodilation with maldistribution of blood flow. In trauma, the most important subtype is neurogenic shock — loss of sympathetic tone below a cervical or high thoracic spinal cord injury. Presents with hypotension AND bradycardia (unlike haemorrhagic shock, which causes tachycardia). Warm, flushed, vasodilated peripheries are characteristic. Septic shock (later in the course) and anaphylaxis are other distributive subtypes.
3. Cardiogenic shock: pump failure — in trauma, caused by blunt cardiac injury, tension pneumothorax (the most immediately reversible cause, treated with needle decompression), or cardiac tamponade (Beck's triad: hypotension + distended neck veins + muffled heart sounds; treated with pericardiocentesis or emergency thoracotomy).
4. Obstructive shock: mechanical obstruction to cardiac output. Tension pneumothorax and cardiac tamponade span cardiogenic and obstructive categories depending on the classification system used; their treatment is decompression of the obstruction.
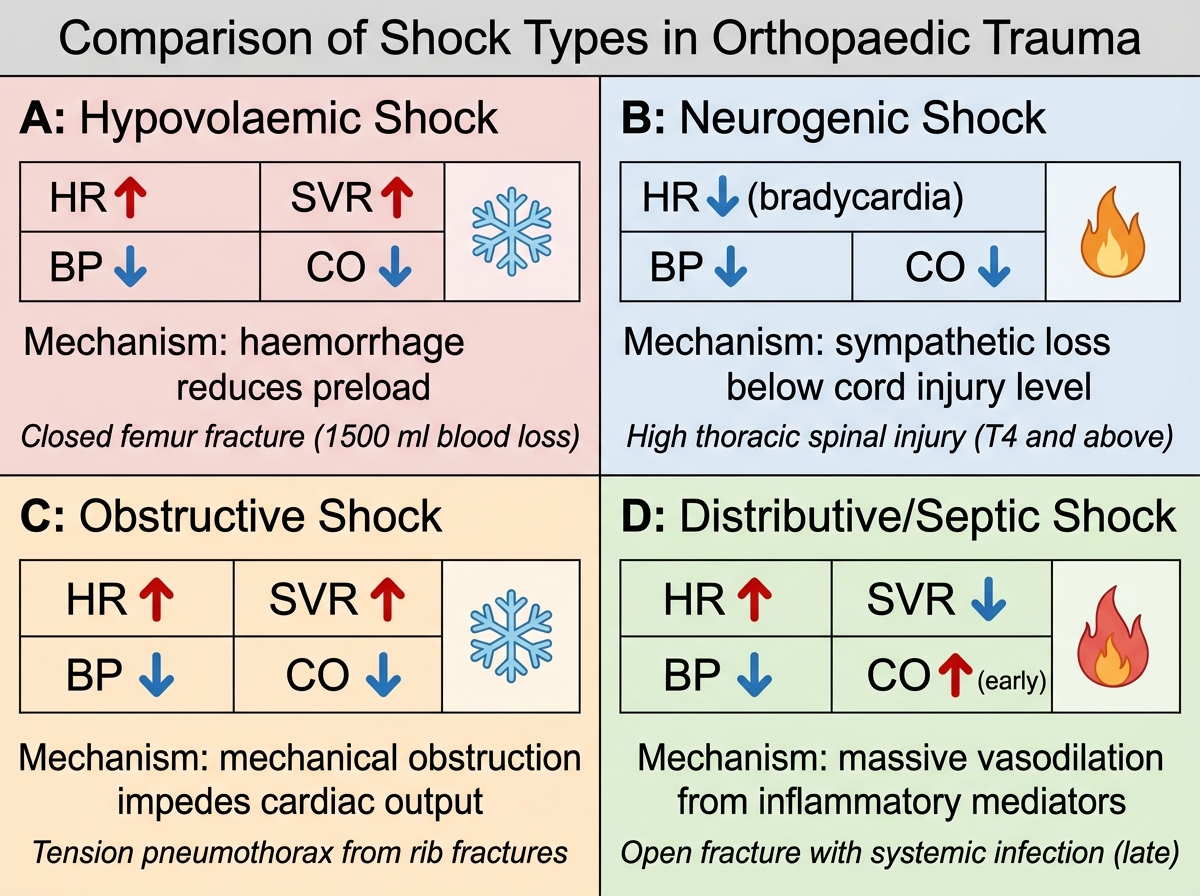
Comparison of the Four Shock Types in Orthopaedic Trauma
Etiopathogenesis of Haemorrhagic Shock
Haemorrhagic shock is the most lethal consequence of major orthopaedic trauma. Its pathophysiology follows a predictable cascade from initial blood loss through compensatory mechanisms to decompensation and irreversible shock. Understanding this sequence explains every clinical sign and management decision. The cascade is not merely academic — each physiological step corresponds to a clinical sign, and recognising where a patient sits in the cascade determines the urgency and nature of intervention. A patient who is compensating (tachycardia, preserved BP) is not 'fine' — they are on a slope that ends in cardiovascular collapse if haemorrhage is not controlled.
Initial blood loss reduces the effective circulating volume, thereby reducing venous return and cardiac preload. By the Frank-Starling mechanism, reduced preload decreases stroke volume and cardiac output. Reduced cardiac output lowers mean arterial pressure (MAP = cardiac output × systemic vascular resistance), triggering baroreceptors in the carotid sinus and aortic arch.
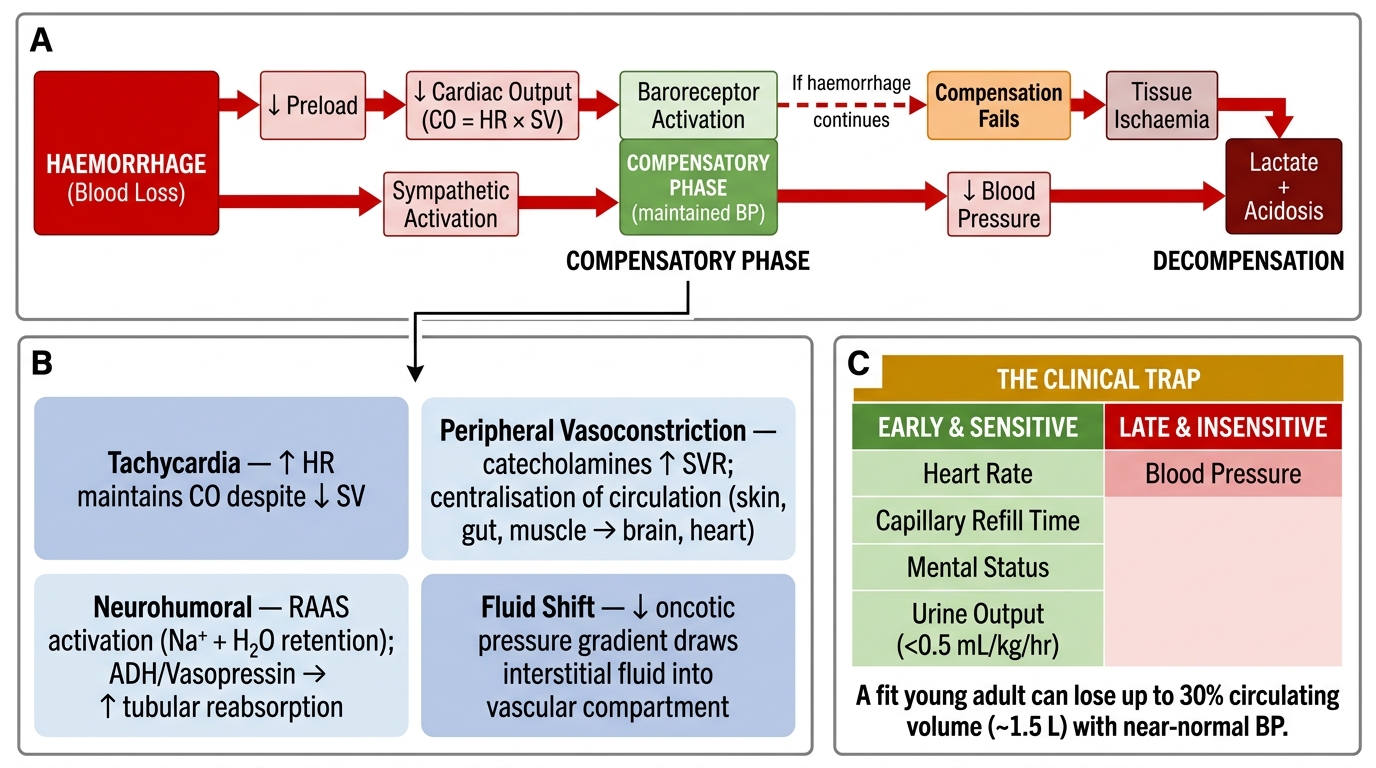
Haemorrhagic Shock Cascade: Compensatory Mechanisms and Clinical Indicators
Compensatory mechanisms are activated by the sympathetic nervous system:
- Tachycardia: heart rate increases to maintain cardiac output despite reduced stroke volume (CO = HR × SV)
- Peripheral vasoconstriction: catecholamine-mediated, increasing systemic vascular resistance and redirecting blood from skin, gut, and muscles to the brain and heart ('centralisation of circulation')
- Neurohumeral responses: renin-angiotensin-aldosterone system activation causes sodium and water retention; ADH (vasopressin) release increases tubular water reabsorption
- Fluid shift: oncotic pressure gradient shifts interstitial fluid into the vascular compartment
These compensatory mechanisms are remarkably effective in young, fit patients — a healthy adult can lose up to 30% of circulating volume (approximately 1.5 litres) while maintaining a nearly normal blood pressure. This is the key clinical trap: blood pressure is a late and insensitive marker of haemorrhagic shock in young trauma patients. Heart rate, capillary refill, mental status, and urine output are earlier and more sensitive indicators.
Decompensation occurs when haemorrhage exceeds the capacity of compensatory mechanisms. Blood pressure falls precipitously (the 'cliff edge' of shock), tissue ischaemia becomes irreversible at the cellular level, anaerobic metabolism produces lactic acid, the coagulation cascade is consumed (trauma-induced coagulopathy), and the lethal triad of hypothermia–acidosis–coagulopathy is established. At this stage, organ damage is occurring even if blood pressure is temporarily restored.
Orthopaedic-specific haemorrhage sources include:
- Femoral shaft fracture: 1–2 L (from muscle tears and periosteal vessels; may be higher in the elderly)
- Pelvic ring fractures (especially open-book/lateral compression): 2–4 L or more from disrupted pelvic venous plexuses and sacral vessels; retroperitoneal haematoma may be very large
- Tibial shaft fracture: 0.5–1.5 L
- Humeral shaft fracture: 0.5–1 L
- Multiple rib fractures (flail chest): 0.3–0.5 L per haemothorax
Clinical Features: ATLS Haemorrhagic Shock Classification
The ATLS system classifies haemorrhagic shock into four classes based on the volume of blood lost and the corresponding physiological response. This classification is a teaching tool and a clinical decision framework — the exact percentage boundaries are less important than understanding the trend of physiological derangement as blood loss worsens. Assessment is made using four accessible bedside parameters: heart rate, blood pressure (systolic and pulse pressure), respiratory rate, and mental status. A clinician who can read these four parameters together can estimate shock class within seconds at the bedside, without waiting for any laboratory result. The key insight is that each class represents a different phase of the compensatory cascade described in the previous section, and the management urgency scales accordingly — Class I may be managed with careful observation, Class IV demands immediate operative haemorrhage control.
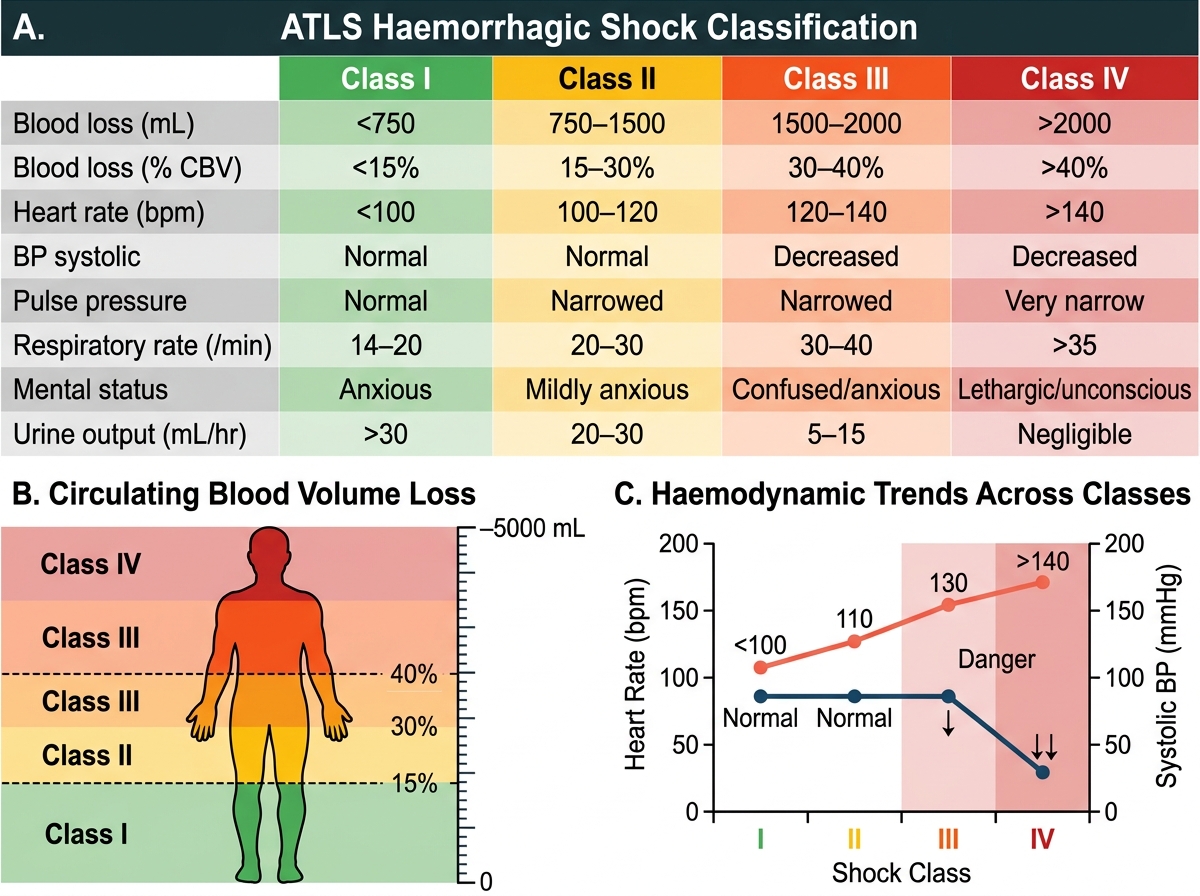
ATLS Classification of Haemorrhagic Shock (Class I–IV)
| Feature | Class I | Class II | Class III | Class IV |
|---|---|---|---|---|
| Blood loss (mL) | <750 | 750–1500 | 1500–2000 | >2000 |
| Blood loss (% CBV) | <15% | 15–30% | 30–40% | >40% |
| Heart rate | <100 | 100–120 | 120–140 | >140 |
| BP (systolic) | Normal | Normal | Decreased | Very low |
| Pulse pressure | Normal/↑ | Decreased | Decreased | Very decreased |
| Respiratory rate | 14–20 | 20–30 | 30–40 | >35 |
| Mental status | Normal | Anxious | Confused | Lethargic/unconscious |
| Urine output (mL/h) | >30 | 20–30 | 5–15 | Negligible |
Several nuances deserve emphasis. The pulse pressure (systolic minus diastolic) narrows early in shock as peripheral vasoconstriction raises diastolic pressure while systolic pressure is maintained — this is an early and sensitive sign. A patient with Class II shock typically has a normal systolic BP but a narrowed pulse pressure. Urine output is one of the most reliable continuous monitors of tissue perfusion; a catheter placed during the primary survey provides moment-to-moment feedback. Mental status deteriorates as cerebral perfusion falls, progressing from anxiety to confusion to obtundation.
Factors that distort the ATLS classification:
- Age: elderly patients compensate poorly (limited cardiac reserve, beta-blocker use) and decompensate at lower blood loss volumes
- Beta-blockers and calcium channel blockers: blunt the tachycardia response; a 'normal' heart rate of 80 in a medicated elderly patient with a pelvic fracture may represent Class III shock
- Athletes: high resting vagal tone; their 'normal' heart rate of 50–60 may mask significant haemorrhage
- Pregnancy: expanded circulating volume (30–40% above baseline at term); significant blood loss before fetal compromise
- Hypothermia and spinal cord injury: further complicate the haemodynamic picture
SELF-CHECK
A 30-year-old woman with a closed femoral shaft fracture has BP 110/80 mmHg, HR 108/min, RR 22/min, and is anxious but oriented. Urine output is 22 mL/h. What ATLS shock class is this, and what is the most important early bedside sign that flagged shock despite a near-normal systolic BP?
A. Class I — the tachycardia is the early sign
B. Class II — the narrowed pulse pressure (110-80=30 mmHg) and tachycardia are the early signs
C. Class III — the low urine output alone defines Class III
D. Class IV — any urine output below 30 mL/h is Class IV
Reveal Answer
Answer: B. Class II — the narrowed pulse pressure (110-80=30 mmHg) and tachycardia are the early signs
This is Class II haemorrhagic shock (750–1500 mL blood loss, 15–30% CBV). The systolic BP is maintained (compensated), but the PULSE PRESSURE is narrowed (110-80 = 30 mmHg, normal ~40 mmHg), indicating peripheral vasoconstriction raising the diastolic. Tachycardia (HR 108), mild tachypnoea (RR 22), anxiety, and reduced urine output (22 mL/h, below the 30 mL/h floor) all confirm Class II. Blood pressure alone is misleading — pulse pressure and heart rate are more sensitive early indicators.