Page 8 of 14
OR13.2 | Polytrauma Resuscitation Team Skills — SDL Guide (Part 4)
Self-Assessment: Consolidating Polytrauma Resuscitation Knowledge
Self-assessment of polytrauma skills requires you to test both declarative knowledge (the ATLS sequence, contraindications, thresholds) and procedural readiness — can you perform each task smoothly under pressure without prompting? These are distinct competency layers and both must be evaluated separately. Knowing that blood at the urethral meatus is a contraindication is declarative knowledge; refusing to catheterise when you find it in a real patient despite pressure from a senior to 'just get on with it' is applied procedural knowledge under social pressure — a categorically harder skill. Similarly, knowing the RSI 7 P's in sequence is very different from executing cricoid pressure correctly while simultaneously monitoring the patient's SpO₂ and maintaining verbal communication with the team leader. The most effective self-assessment for this SDL is therefore a mental simulation run from the moment the trauma call is activated to the moment the primary survey is complete — narrate each step aloud, including what you would say to the team leader at each transition. Where the narration stalls or becomes vague, that is your revision target.
Key self-check domains for this SDL:
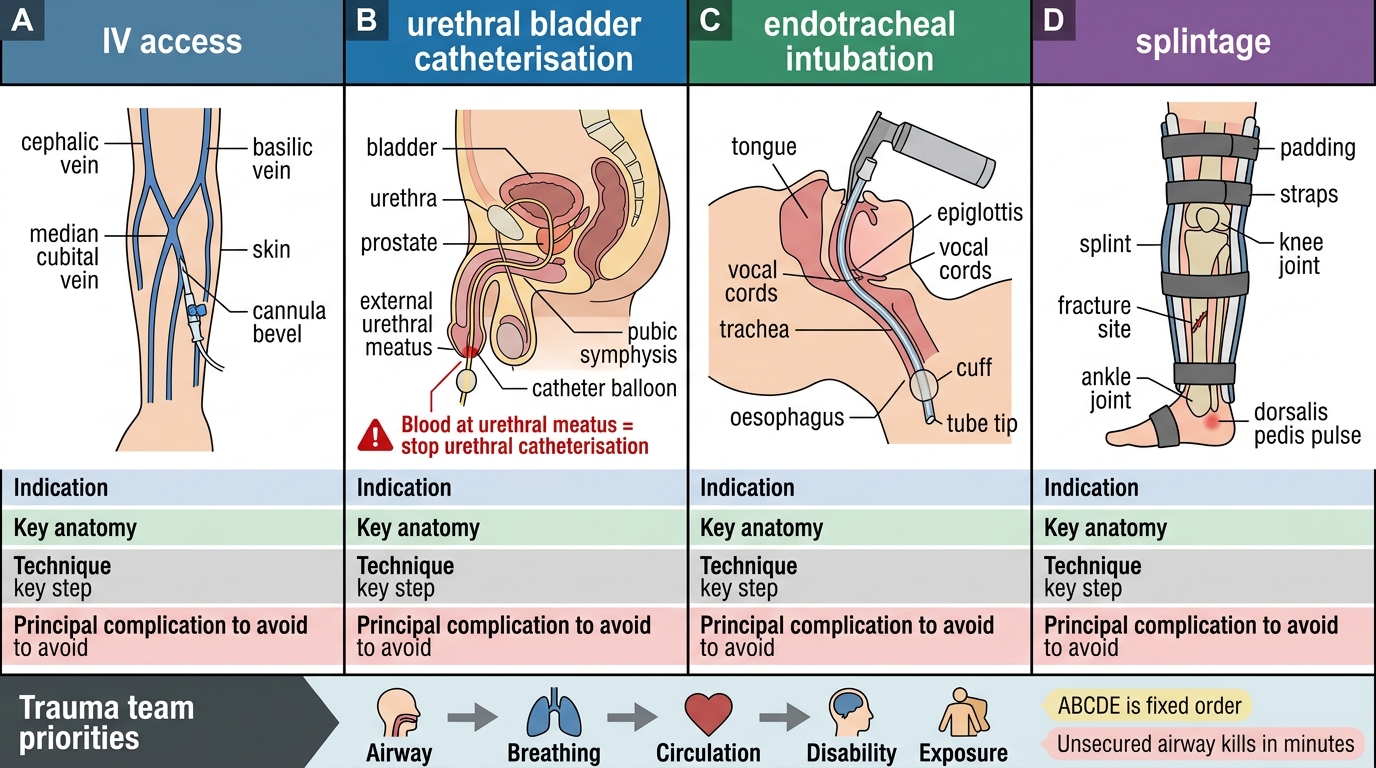
- ATLS ABCDE sequence: can you recite the five steps and their immediate actions from memory without prompting?
- IV access: can you name the first-choice site, the correct cannula gauge, the blood samples to take from the first cannula, and the Hagen-Poiseuille principle that explains why short wide-bore cannulae are faster?
- Bladder catheterisation contraindication: can you name all three clinical signs of urethral injury, and state the safe alternative?
- RSI 7 P's: can you walk through the seven steps including the induction agents, the neuromuscular blocker dose, and the confirmation method?
- Ketamine rationale: can you explain why ketamine is preferred over thiopentone in haemodynamically unstable trauma?
- ETCO₂: what does loss of the waveform mean after a confirmed intubation, and what is the DOPE check?
- Resuscitation response classification: what is the difference between a transient responder and a non-responder, and what does each imply for further management?
Trauma Team Procedures: Summary Revision Table
SELF-CHECK
Which of the following findings on the initial trauma assessment is an absolute contraindication to urethral bladder catheterisation?
A. Haematuria from the suprapubic region
B. Blood at the urethral meatus
C. Gross pelvic instability on compression
D. Systolic blood pressure of 70 mmHg
Reveal Answer
Answer: B. Blood at the urethral meatus
Blood at the urethral meatus is the absolute contraindication to urethral catheterisation because it indicates urethral injury. Gross pelvic instability increases the suspicion for urethral injury but is not itself a contraindication — the meatal check and perineal examination confirm the decision. Haematuria from the suprapubic region (suggesting bladder injury) and hypotension are not contraindications to the catheter itself.
CLINICAL PEARL
Four non-negotiable rules for polytrauma resuscitation:
- ABCDE is a fixed order — never skip a step. An unsecured airway kills in minutes; a missed distal pulse does not. The sequence is not alphabetically arbitrary — it reflects the time-to-death hierarchy of life threats.
- Blood at the urethral meatus = do NOT catheterise transurethrally. This single rule, applied correctly, prevents converting a partial urethral tear into a complete disruption. Call for suprapubic catheterisation by the surgeon.
- In haemodynamically unstable trauma, use ketamine for induction (1–2 mg/kg IV), not thiopentone or propofol. Thiopentone and propofol drop blood pressure in an already shocked patient. Ketamine supports it.
- Short and fat beats long and thin for IV access. A 14G peripheral cannula delivers fluid faster than a 16G central line because of Hagen-Poiseuille: flow ∝ r⁴ / length. Two large-bore peripheral cannulae before one central venous catheter.