Page 1 of 16
OR14.1-2 | Orthopaedic Prognosis and Consent Counselling — SDL Guide
Learning Objectives
- Counsel a patient with a fracture likely to result in permanent disability, communicating realistic functional outcomes and the expected recovery timeline
- Explain the prognosis of bone tumours to a patient and family, using plain language while addressing uncertainty and emotional distress
- Obtain valid informed consent for limb amputation or permanent internal fixation by ensuring capacity, adequate disclosure, voluntariness, and proper documentation
- Apply the SPIKES protocol to structure a difficult prognosis-breaking conversation in an orthopaedic setting
- Counsel the parent of a child with congenital disability, addressing long-term management expectations and community support resources
INSTRUCTIONS
Orthopaedic conditions frequently impose life-altering consequences — permanent disability from fracture complications, years of bed rest, mutilating surgery, or lifelong prosthetic dependence. The ability to communicate these realities compassionately and accurately is as essential as any surgical skill. This module develops your competence in prognosis counselling and valid consent procurement for major orthopaedic interventions, using the SPIKES structured communication protocol and the four legal pillars of informed consent. These skills directly affect patient safety, medicolegal protection, and the therapeutic relationship that determines whether patients accept and adhere to complex treatment plans.
References
- Maheshwari's Essential Orthopaedics, 6th ed, Ch 1 (General Principles) and Ch 35 (Rehabilitation) (textbook)
- Apley & Solomon's System of Orthopaedics and Trauma, 10th ed, Ch 1 (Diagnosis in Orthopaedics) (textbook)
- Ebnezar's Textbook of Orthopaedics, 5th ed, Ch 4 (Patient Assessment and Communication) (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 45-year-old labourer sustains a severely comminuted intra-articular calcaneal fracture after a fall from scaffolding. After surgery, the orthopaedic team know the patient will likely never return to heavy labour and may face chronic pain and subtalar arthritis. As the ward doctor, you are the first person to sit with him and his wife to explain what lies ahead. He looks at you and asks: 'Will I ever walk normally again, doctor?' How do you answer — truthfully, compassionately, and in a way that preserves hope without offering false reassurance?
WHY THIS MATTERS
Prognosis counselling and consent procurement are among the most legally and ethically consequential acts in clinical practice. In orthopaedics, the stakes are especially high: amputation is irreversible; permanent fixation devices alter a patient's body for life; prolonged immobilisation affects earning capacity and family dynamics; bone tumour prognoses involve mortality. A consent form signed without genuine understanding is legally void and ethically equivalent to assault. An inadequate prognosis conversation leads to unrealistic expectations, patient dissatisfaction, and litigation — the most common cause of medico-legal complaints in orthopaedic practice in India. For final-year MBBS students who will immediately begin internship in fracture wards and OPDs, this skill is not optional — it is a patient-safety requirement.
RECALL
Before proceeding, activate your existing knowledge: recall the four elements of a valid contract (offer, acceptance, consideration, capacity) and how 'capacity' is defined legally. Recall what you know about the informed consent doctrine from your ethics and forensic medicine postings — particularly the landmark case that established the duty to disclose material risks. Review in your mind the orthopaedic conditions listed in competency OR14.1 (fractures with disabilities, prolonged bed rest, bone tumours, congenital disabilities) and the procedures in OR14.2 (limb amputation, permanent internal fixation). Finally, recall the meaning of 'therapeutic privilege' and when, if ever, information may ethically be withheld.
Clinical Indications for Prognosis Counselling in Orthopaedics
Prognosis counselling is required whenever the natural course of an orthopaedic condition will impose a significant, lasting burden on the patient's physical function, livelihood, or quality of life. This requirement is not confined to life-threatening diagnoses — a young labourer told he will never return to heavy work faces an economic and identity crisis that demands the same careful communication as a cancer diagnosis. In orthopaedic practice, four broad clinical categories most consistently necessitate structured prognosis conversations.
The first category encompasses fractures with residual disabilities — intra-articular fractures of the calcaneus, tibial plateau, or distal femur that routinely result in post-traumatic arthritis, stiffness, or malalignment regardless of technically optimal surgical management. Patients in this group need to understand that 'fixing the bone' does not guarantee full functional recovery, and that rehabilitation will be prolonged and effortful.
The second category involves fractures requiring prolonged bed rest or immobilisation — femoral shaft fractures managed conservatively with skeletal traction in children, unstable pelvic ring injuries, or high spinal fractures. Six to twelve weeks of traction carries enormous social costs (job loss, family disruption, pressure sores, deep vein thrombosis), and the patient must be prepared for this trajectory at the outset.
The third category is bone tumours, both benign (giant cell tumour, osteochondroma with malignant potential) and malignant (osteosarcoma, Ewing's sarcoma, metastatic disease). Prognosis here intersects with oncology and palliative care principles; the orthopaedic surgeon's role is often to communicate that limb-salvage surgery carries recurrence risk, and that amputation may be proposed not as a failure but as the option most likely to achieve cure or adequate palliation.
The fourth category involves congenital disabilities counselled in the paediatric or adolescent setting — children with severe clubfoot deformity, developmental dysplasia of the hip, congenital limb deficiencies, or osteogenesis imperfecta. Here, counselling is primarily directed at parents and caregivers, with evolving inclusion of the maturing child, addressing a lifetime of staged interventions, adaptive equipment, and psychosocial challenges.
In every category, the trigger for a formal prognosis conversation is the same: when the clinician knows, or has strong reason to believe, that the patient's life trajectory will be substantially altered by the condition or its treatment.
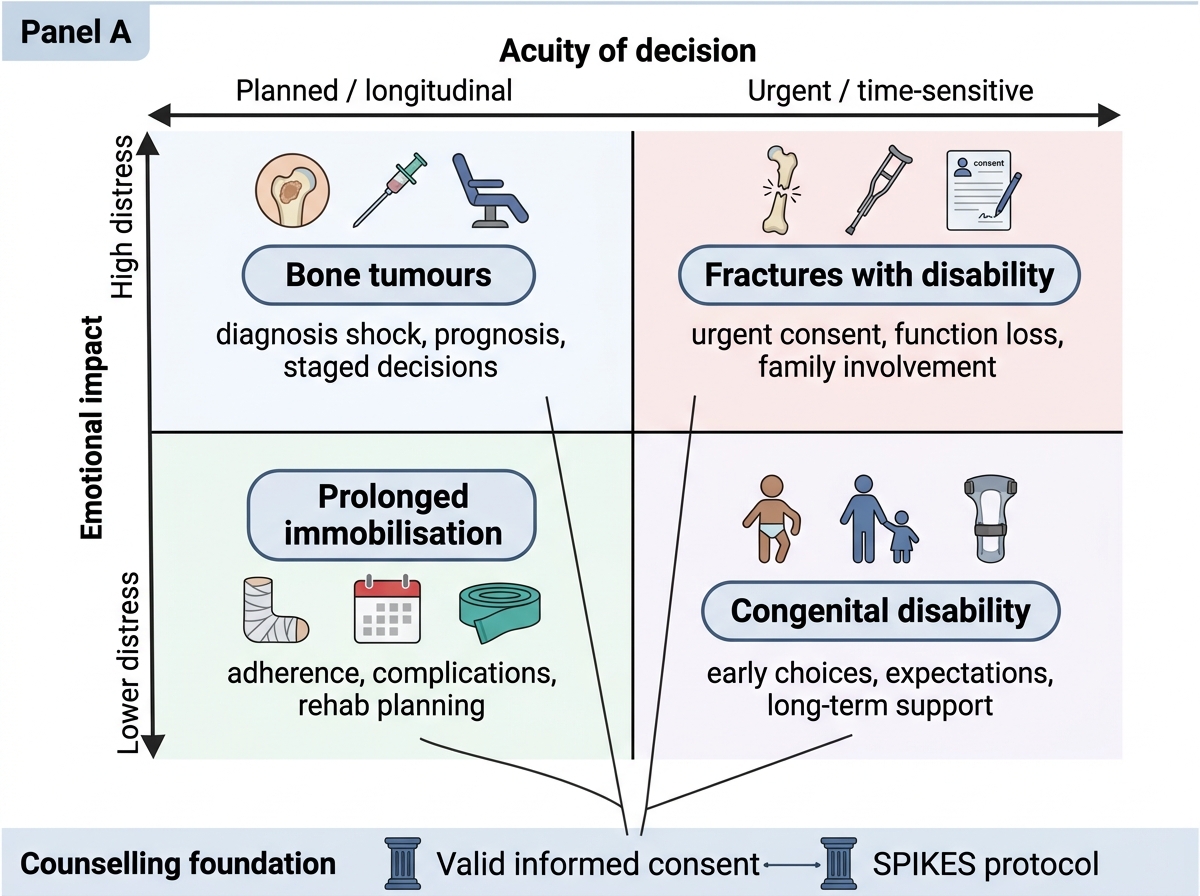
Orthopaedic Counselling Categories by Decision Acuity and Emotional Impact
Governing Principles: Valid Informed Consent and the SPIKES Protocol
The legal and ethical framework for orthopaedic counselling rests on two pillars: the doctrine of valid informed consent and the science of structured difficult-news communication. Understanding both in depth is essential before attempting either with a real patient.
Elements of valid informed consent in Indian law (derived from the Consumer Protection Act 2019 as applicable to medical services, and established case law) requires the simultaneous presence of four conditions. First, decision-making capacity: the patient must be legally competent (adult, ≥18 years under the Indian Majority Act 1875, or a competent minor above 12 years in certain states) and cognitively capable — not intoxicated, not delirious, not under the influence of sedative pre-medication. For a patient in the accident and emergency department who is in pain and distress, capacity must be explicitly assessed, not assumed. Second, adequate disclosure: the clinician must communicate, in the patient's own language and at their literacy level, the nature of the proposed procedure, its purpose, the material risks (those that a reasonable patient in that situation would consider significant), the benefits, the alternatives including non-surgical management, and the consequences of refusal. 'Material' in the Indian context is interpreted subjectively — what matters to this patient, not what a hypothetical 'reasonable patient' might abstractly want to know. Third, voluntariness: consent must be freely given, free from coercion, undue pressure from family members or healthcare providers, or financial desperation that distorts decision-making. A signature obtained by repeatedly emphasising that 'you will die without surgery' while blocking the patient's ability to seek a second opinion is not genuinely voluntary. Fourth, proper documentation: the signed consent form must record the specific procedure by name (not 'operation as decided'), the risks disclosed, the patient's questions and how they were addressed, the language used, and the date and time. A generic form signed hours before surgery in an incomprehensible language does not satisfy this element.
SPIKES is the most widely validated structured protocol for breaking bad news, developed by Baile et al. (2000) for oncology and now applied universally including in orthopaedic contexts. The six-step acronym provides a scaffolding that reduces clinician anxiety, ensures completeness, and creates a patient-centred encounter even when the content is devastating.
- S — Setting up the interview: choose a private room, not a crowded ward corridor; switch off your pager or hand it to a colleague; arrange seating so you are at eye level, not standing over the bed; invite the patient to bring a family member or support person if they wish.
- P — assessing Perception: before you disclose, ask what the patient already understands — 'What have the other doctors told you so far?' or 'How did you think the surgery went?' This reveals misconceptions, calibrates your starting point, and gives the patient agency in the conversation.
- I — obtaining an Invitation: ask explicitly whether the patient wants to hear the full details now — 'Would you like me to explain everything I know about how this is likely to progress?' Some patients use a 'gatekeeper' family member and prefer a staged approach; honouring this is not evasion, it is person-centred care.
- K — giving Knowledge and information to the patient: deliver the prognosis in plain language, in short segments, pausing to check understanding. Avoid euphemisms that obscure meaning — 'The tumour appears to be serious' is less kind than honest when a patient later learns 'serious' meant 'almost certainly fatal'. Signal the shift: 'I am afraid the news is not what we hoped…' prepares the patient cognitively for the content.
- E — addressing Emotions with Empathic responses: the emotional response (silence, tears, anger, denial) is not a disruption of the consultation — it IS the consultation. Stop the information-giving. Acknowledge: 'I can see this is very hard to hear' or 'It is completely understandable to feel angry'. Avoid premature reassurance ('Everything will be fine') which is dishonest and shuts down further questions.
- S — Strategy and Summary: close with a clear statement of the next steps — what happens tomorrow, what the patient needs to do, who will support them. Provide written information if available. Fix a follow-up appointment before leaving the room.
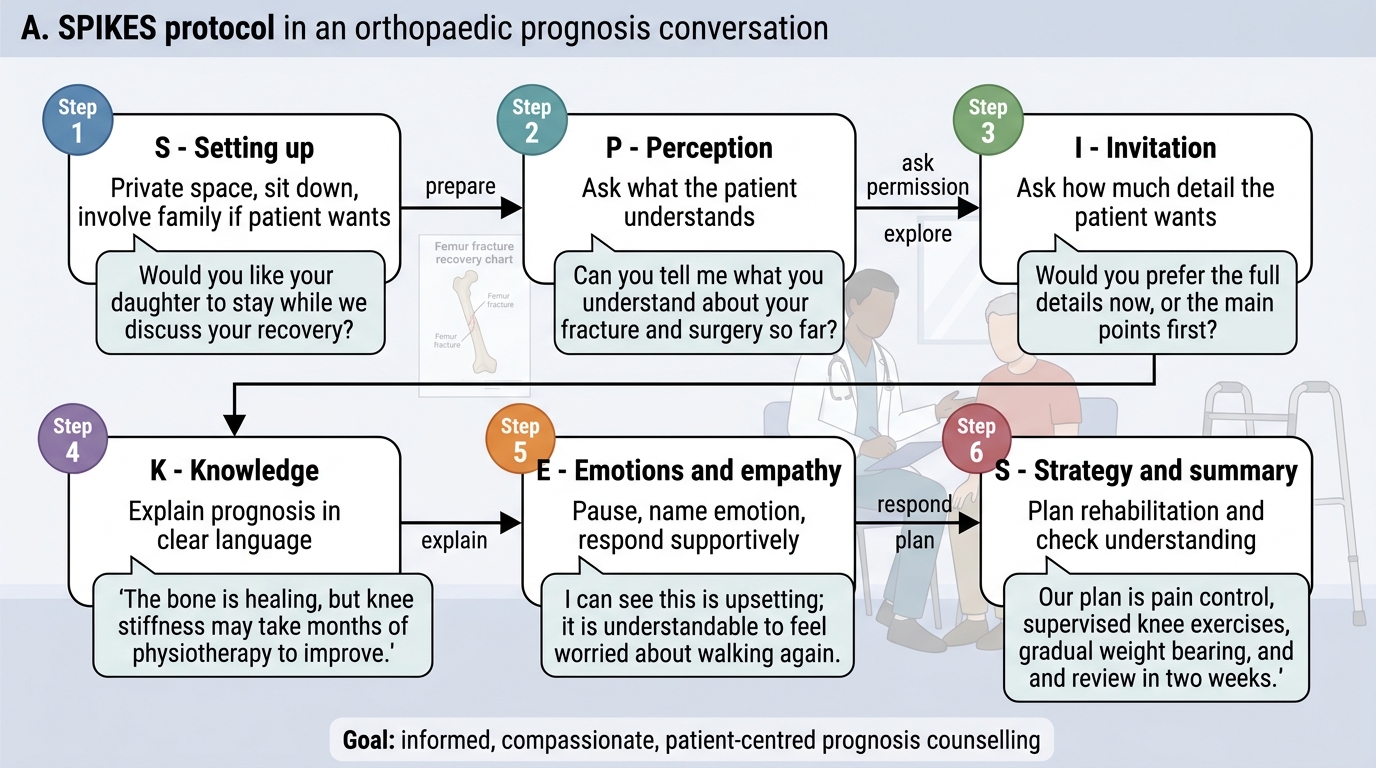
SPIKES Protocol for Orthopaedic Prognosis Counselling
SELF-CHECK
A patient recovering from a supracondylar femur fracture is told by a junior nurse, 'Doctor says you must sign this form for the operation — don't worry, it's routine.' The patient signs without asking questions. Which element of valid consent is MOST clearly absent?
A. Decision-making capacity
B. Adequate disclosure
C. Voluntariness
D. Written documentation
Reveal Answer
Answer: B. Adequate disclosure
Adequate disclosure requires the clinician (or appropriately trained delegate) to ensure the patient understands the nature, risks, benefits, alternatives, and consequences of refusal in their own language at their literacy level. Being told 'it's routine' and signing without explanation constitutes wholly inadequate disclosure. The patient was not deprived of capacity, was not directly coerced (voluntariness), and the form was signed (there is documentation, albeit deficient). The core gap is the absence of genuine information exchange.
Counselling Technique: Delivering Prognosis for Specific Orthopaedic Conditions
Each major orthopaedic prognosis scenario requires a tailored communication approach because the emotional stakes, the decision urgency, and the clinical uncertainties differ considerably. A one-size-fits-all script fails patients and exposes clinicians.
Fractures with permanent disabilities: Begin by establishing what the patient currently understands about their injury. Most patients, especially those injured in road traffic accidents or workplace falls, have not yet processed the severity of their injury. Use plain anatomical language supported by simple diagrams or X-ray explanation. For intra-articular fractures (ankle, calcaneus, tibial plateau, hip), be explicit that joint cartilage damage may lead to post-traumatic arthritis over months to years, that full pre-injury function may not be achievable even after technically successful surgery, and that pain and stiffness may be lifelong. Quantify where possible using functional language the patient understands: 'You will likely be able to walk around your home and do gentle activities, but returning to heavy manual labour is unlikely.' Avoid using phrases like 'You will never walk again' if function is preserved — precision matters. Outline the rehabilitation pathway including physiotherapy duration and expected milestones.
Fractures requiring prolonged bed rest: Patients facing 8–12 weeks of skeletal traction (or enforced immobilisation for spinal injuries) face social disruption, financial crisis, and physical complications including pressure ulcers, deep vein thrombosis, urinary tract infections, and muscle wasting. Counsel explicitly about these risks — not to alarm, but to ensure the family and caregiving network are mobilised. For a rural patient with limited support structures, social service referral may be as important as the medical management. Set clear milestones ('By week 4 we expect you to be sitting up; by week 8 we aim to start mobilisation') to give the patient a sense of trajectory.
Bone tumours: This is the most emotionally demanding orthopaedic prognosis scenario. For malignant primary bone tumours (osteosarcoma, Ewing's sarcoma), use the SPIKES protocol fully. Disclose the diagnosis clearly, not through euphemism. Explain the treatment plan (neoadjuvant chemotherapy + surgery) and the functional outcomes of limb-salvage surgery versus amputation — both are legitimate oncological options with different risk profiles. For osteosarcoma, the 5-year survival with optimal treatment has improved to approximately 60–70% for localised disease, but this must be communicated as probabilistic, not certain. Avoid the trap of false optimism — 'Many patients do well' without qualification is misleading if the tumour is already metastatic. Involve the patient's family early (with the patient's consent), and always refer to a multidisciplinary oncology team.
Congenital disabilities counselled to parents: Parents of children with congenital talipes equinovarus (CTEV), developmental dysplasia of the hip (DDH), or congenital limb deficiencies are typically frightened, guilty (especially if they perceive causation as genetic), and overwhelmed. The counselling tone must be reassuring without minimising the challenge. Begin with what can be achieved: Ponseti's casting for CTEV achieves excellent functional correction in the majority of cases. DDH, if treated early (before 18 months), has an excellent prognosis. Explain the timeline of interventions, the need for regular follow-up, the role of bracing or serial casting, and when surgical correction becomes necessary. Signpost parent support groups and national disability services. Always address guilt directly: 'This condition was not caused by anything you did during pregnancy.'
Consent for amputation: This requires the most careful consent process in orthopaedic practice because the decision is irreversible and profoundly affects body image and function. Ensure the consent conversation is held when the patient is fully alert and not immediately post-injury (the Emergency Department is the wrong place for an amputation consent unless the limb is already unsalvageable). Disclose the reason for amputation (failed vascularisation, irreversible contamination, tumour ablation), the alternatives that were considered (limb salvage, revascularisation), and their outcomes in this specific case. Describe the expected post-amputation functional outcome including prosthesis options, rehabilitation timeline, and realistic activity expectations. Document specifically that the patient was informed of the irreversible nature of the procedure.
Consent for permanent internal fixation: For patients receiving intramedullary nails, plates, or joint replacements, explain that the implant is designed to remain in situ permanently, that implant removal later is possible but itself carries surgical risk, that some metal sensitivity reactions are possible (though rare), and that certain activities (e.g. high-impact sports, contact sports with an arthroplasty) should be modified.
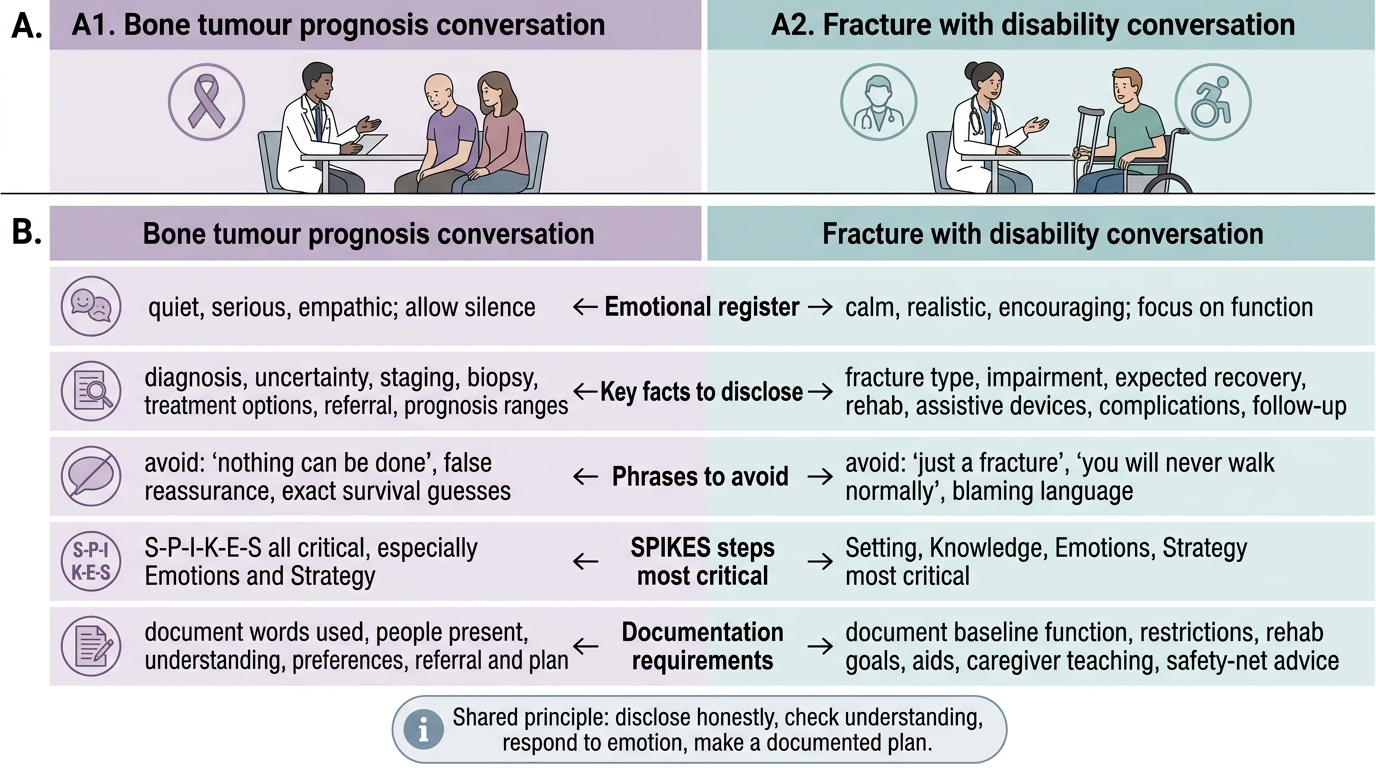
Comparing Difficult Orthopaedic Counselling Conversations