Page 5 of 16
OR14.3 | Referral Counselling for Orthopaedic Warning Signals — SDL Guide (Part 2)
Reading Urgency Cues and Managing the Reluctant Patient
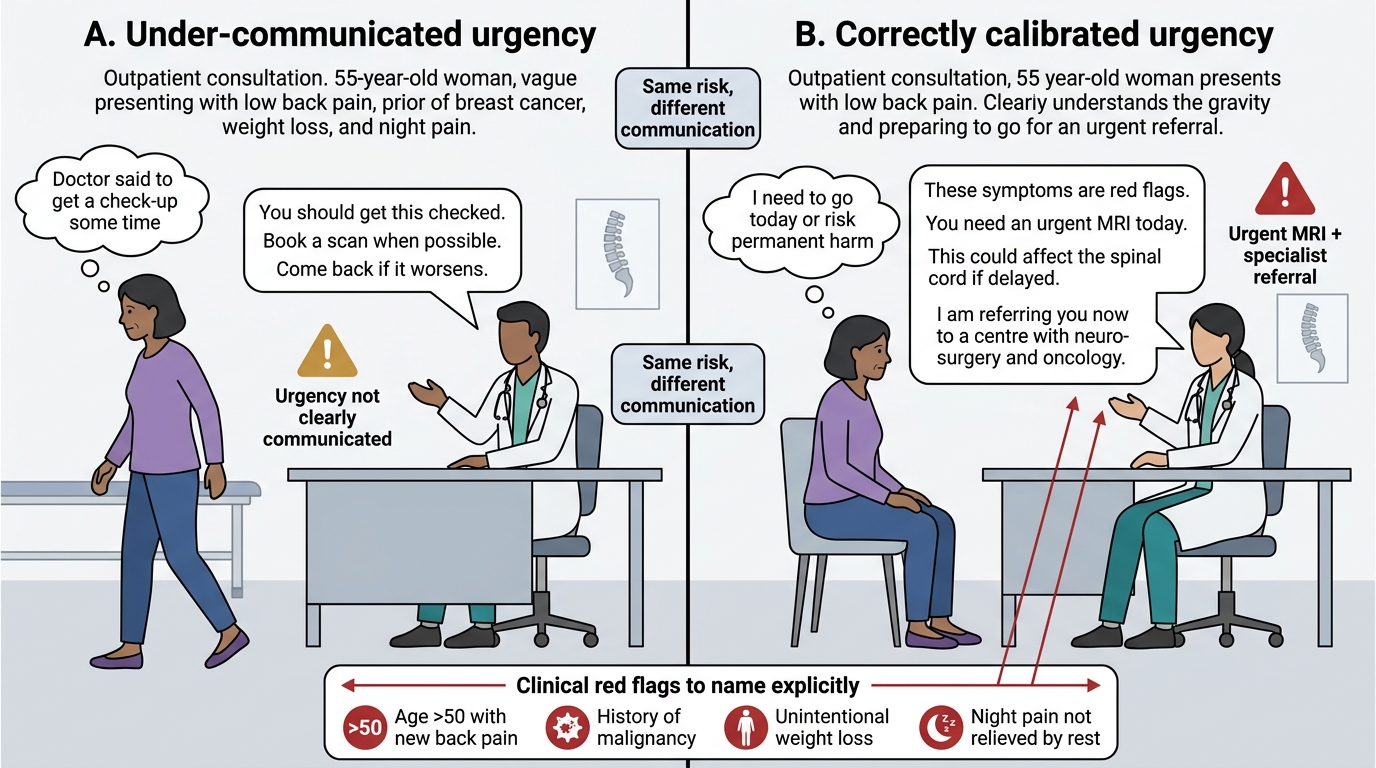
Calibrating your communication to the actual urgency of the clinical situation is a skill that prevents two opposite errors: under-communicating urgency to a patient who then delays, and over-communicating urgency to a patient who panics and becomes uncooperative. The mechanism for calibration is your clear understanding of the pathophysiological timeline — how much time does the patient have before the window of reversibility closes?
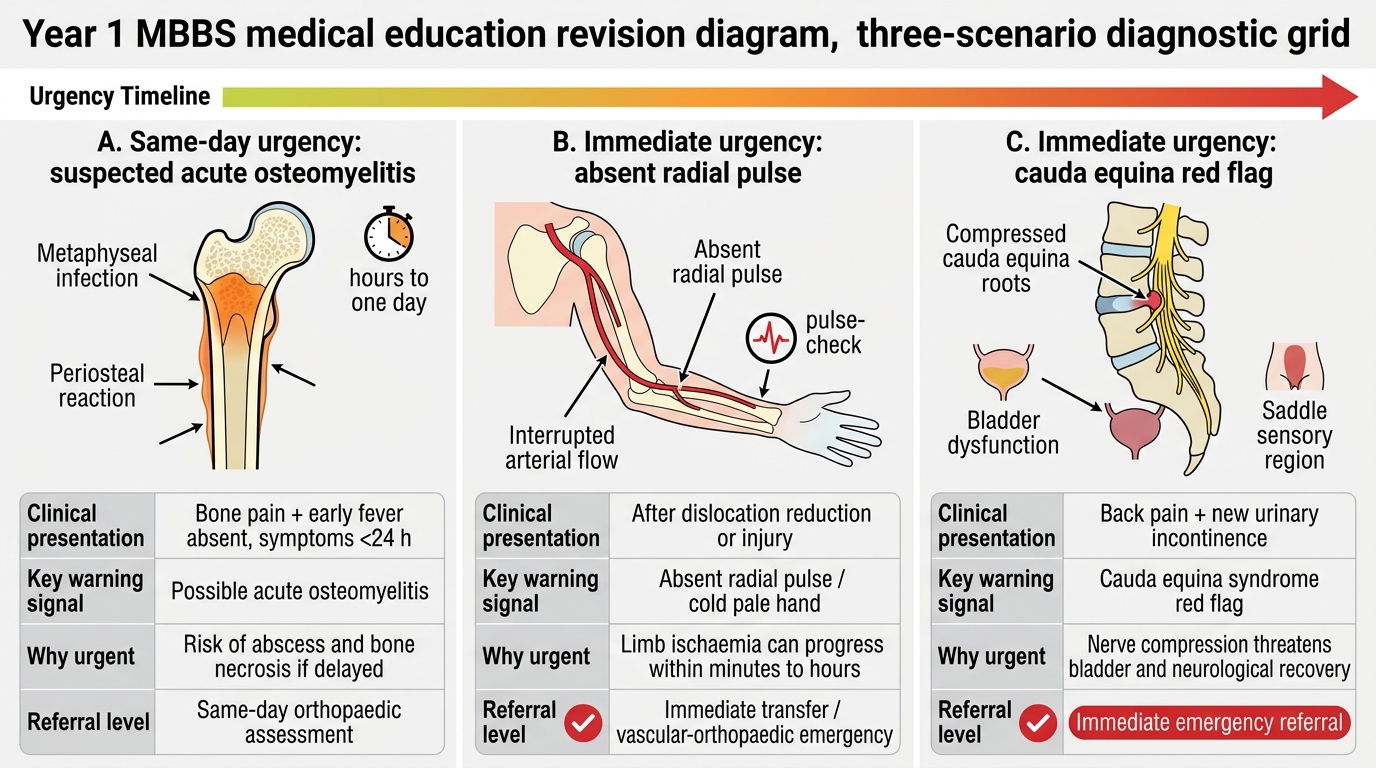
For a patient with suspected acute osteomyelitis who is systemically well, afebrile, and has had symptoms for only one day, you have a window of hours to a day before abscess formation. Your communication tone is firm and urgent, but not panic-inducing: 'This needs to be seen today — not tomorrow, but today.'
For a patient with a post-dislocation absent radial pulse, you are communicating at the level of minutes to hours. Your communication is direct and unambiguous: 'The blood supply to the lower part of your arm may be blocked. We need to transfer you right now — this cannot wait.'
For a patient with new urinary incontinence and back pain (cauda equina syndrome), you are at the threshold of permanent damage. The conversation moves from counselling to near-emergency directive: 'I need to explain this very directly. The nerve to your bladder may be compressed. If we do not get you to surgery within hours, this incontinence may become permanent. I am calling an ambulance now.'
The pattern of patient reluctance in orthopaedic referrals is reasonably predictable. Financial concern is the most common stated reason for hesitation in rural and low-income urban populations — a specific, concrete response (naming the scheme, offering to call ahead about emergency coverage) is more effective than a general 'don't worry about money'. Fear of 'big operations' underlies many soft refusals — distinguishing between the diagnostic procedure (aspiration, which is minor) and the possible operation (washout, which may or may not be needed) often reduces resistance. Denial ('it's not that bad — I can still move it') can be addressed by repeating the examination finding in concrete terms: 'I want you to notice that your son is not putting any weight on that leg — even though he is trying to protect you from worry. That tells me the pain is more than he is showing.'
Information hierarchy: not every detail of the diagnosis needs to be communicated in the referral conversation. What must be communicated is: (1) what you found and why it is dangerous, (2) the time-sensitivity, (3) what the higher centre can do to fix it, and (4) the consequence of delay. What can wait: the precise microbiology, the surgical technique, the detailed prognosis — these are for the receiving team. An overwhelmed patient who has been told everything at once is paradoxically less likely to act than one who receives a focused, actionable message.
Calibrating Urgency in Red-Flag Back Pain Counselling
SELF-CHECK
A 55-year-old woman presents with a 6-week history of low back pain, unintentional weight loss of 5 kg, and night pain that wakes her from sleep. She has a history of treated breast cancer 4 years ago. The back pain is not relieved by rest. Which of the following is the MOST appropriate management?
A. Prescribe NSAIDs, refer for physiotherapy, and review in 4 weeks
B. Arrange urgent MRI of the spine and refer to a centre with neurosurgical and oncological capability
C. Order a plain X-ray of the lumbar spine in OPD and treat with muscle relaxants if no fracture
D. Reassure the patient that back pain after cancer treatment is usually benign and due to deconditioning
Reveal Answer
Answer: B. Arrange urgent MRI of the spine and refer to a centre with neurosurgical and oncological capability
This presentation carries four simultaneous red flags for serious spinal pathology: age >50 with new back pain, known history of malignancy, unexplained weight loss, and night pain unrelieved by rest. In the context of treated breast cancer, metastatic spinal disease is a leading diagnosis until excluded. This requires urgent MRI of the spine (plain X-rays can miss spinal metastases until >30% of trabecular bone is lost), and onco-spinal team assessment. Physiotherapy and NSAIDs alone are inappropriate. Reassurance without investigation is dangerous — cord or cauda equina compression from metastatic disease can cause permanent neurological deficit within days.
Applied and Supervised Practice: Referral Communication in Clinical Settings
Translating the conceptual framework of referral counselling into effective clinical practice requires deliberate supervised exposure to the relevant scenarios. The following structured activities are designed to build your competence progressively from observation through supervised practice to independent performance.
Observation of emergency referral conversations: During your orthopaedic and accident and emergency postings, identify cases where a referral to a higher centre or subspecialist is initiated. Observe the conversation structure — does the clinician name the finding explicitly? Do they explain the limitation of the current facility? Do they address the patient's stated concern? Is the referral letter written and handed to the patient? Note both what was done well and what was omitted, and debrief with your supervisor.
Structured referral letter writing: For each orthopaedic emergency you encounter during your posting, write a referral letter draft that includes: (a) the clinical findings that constitute the warning signal, (b) the urgency level (immediate/same-day/within 24 hours), (c) investigations already performed and their results, (d) treatment already initiated (analgesics given, antibiotics started), and (e) the question you want the receiving team to answer. Compare your draft with what the registrar actually sends — identify the gaps.
Red flag checklist practice: In your low back pain clinic, systematically apply the red-flag checklist to every patient presenting with back pain, regardless of whether you think the presentation is mechanical. This builds automaticity — the checklist must become reflexive rather than optional. Review your checklist application with your supervisor weekly.
Role-play for the reluctant-patient scenario: With a peer, simulate the following scenario: a rural labourer with a post-injury swollen knee and absent distal pulse refuses referral because 'I cannot afford to miss work tomorrow.' One plays the patient, one the doctor. Swap after 10 minutes. Debrief on which communication strategies were effective and which hardened the resistance.
Telephone handover practice: In modern hospital practice, referral begins with a telephone call to the receiving team. Practice the structured telephone handover format: Situation (what is the problem), Background (relevant history), Assessment (what you think it is and why it is urgent), Recommendation (what you are asking them to do). This SBAR format is the standard in most hospitals and ensures the receiving team is prepared before the patient arrives.
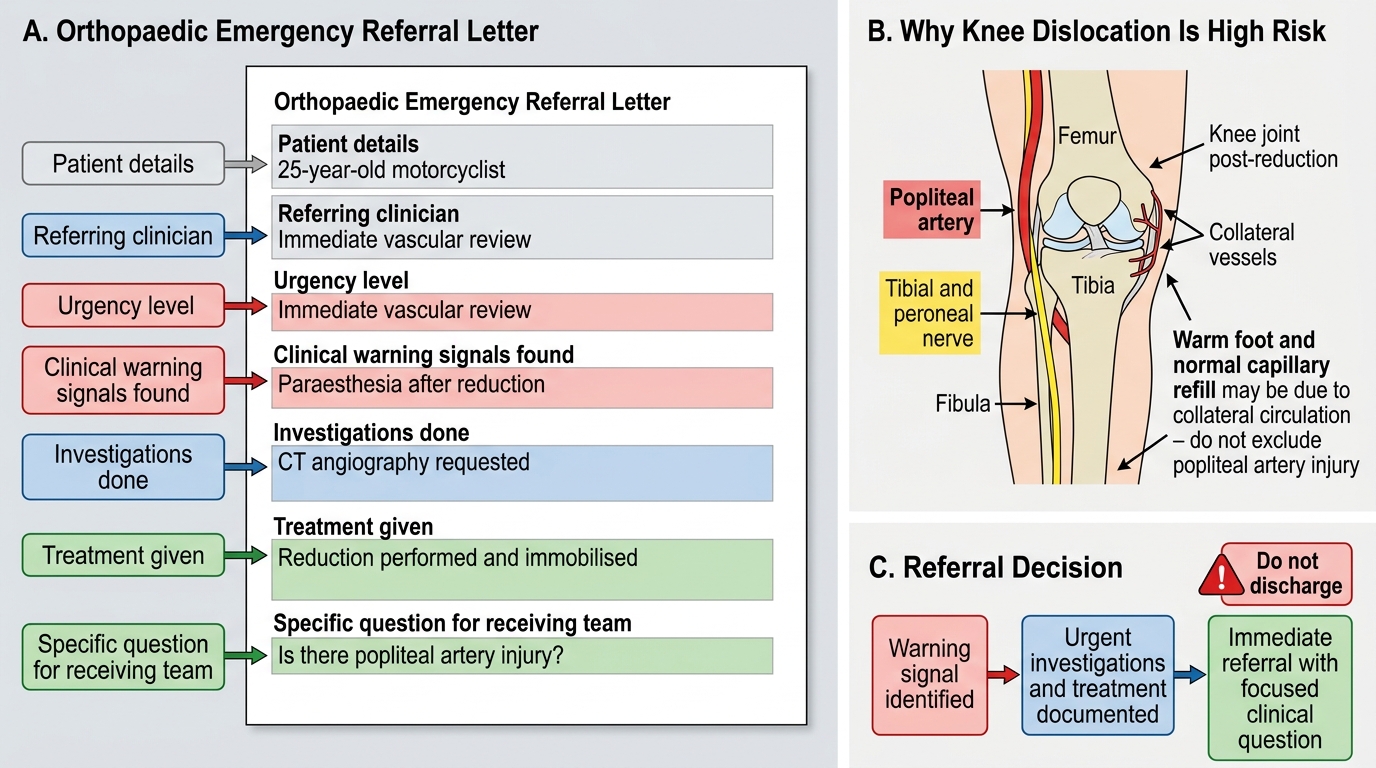
Orthopaedic Emergency Referral Letter Template
Self-Assessment: Testing Warning Signal Recognition and Referral Communication
Provided image
The following self-assessment scenarios test both warning-signal identification and referral counselling strategy. Work through each scenario before reading the discussion.
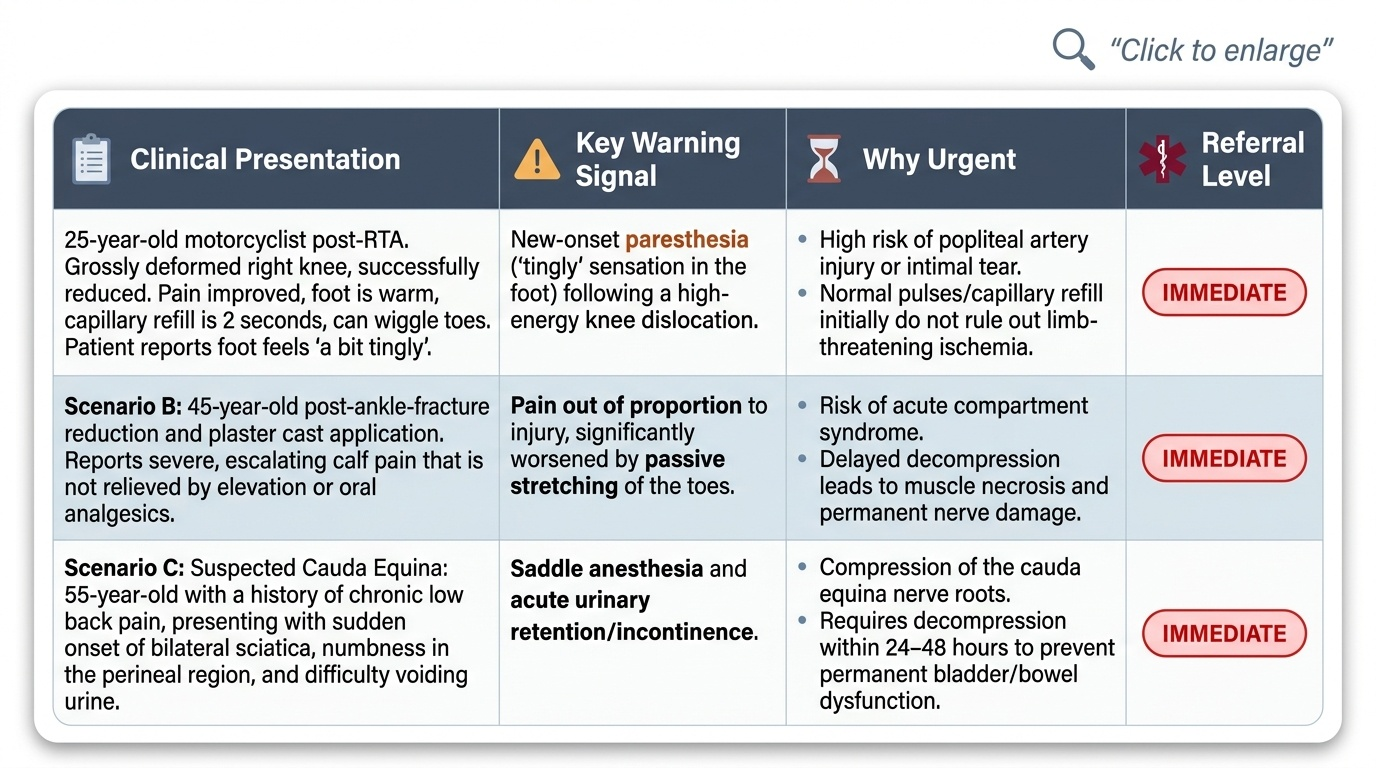
Scenario A: A 25-year-old motorcyclist is brought in after a road traffic accident. His right knee is grossly deformed — you suspect a knee dislocation. You reduce the knee successfully. The pain improves. On reassessment, the right foot is warm, capillary refill is 2 seconds, and the patient can wiggle his toes. He says his foot feels 'a bit tingly' and asks if he can go home. Should you refer?
Discussion: Yes — immediately, for vascular surgery assessment. Knee dislocation is the most dangerous fracture-dislocation pattern for vascular injury because the popliteal artery is tethered at both ends and is torn in approximately 20–35% of knee dislocations. The apparent warmth and capillary refill may reflect collateral circulation, not intact popliteal flow. The tingling (paraesthesia) is an early neurovascular warning signal. Successful reduction does not exclude arterial injury. This patient requires urgent angiography or CT angiography and vascular surgical assessment — a 'wait and see' approach risks limb loss.
Scenario B: A 60-year-old man presents with three months of gradually worsening low back pain. He also has a new difficulty starting urination and reports that he sometimes cannot tell when his bladder is full. He describes the back pain as 'constant'. Which red flag in this presentation mandates same-day referral?
Discussion: Bladder dysfunction (urinary retention, reduced sensation of bladder fullness) is the cardinal sign of cauda equina syndrome — compression of the sacral nerve roots by a large central disc prolapse, tumour, or haematoma. This is a neurosurgical emergency. The window for recovery of sphincter function after decompression is approximately 24–48 hours from onset; delay beyond 72 hours significantly reduces the likelihood of regaining continence. This patient must be referred immediately for emergency MRI of the lumbar spine and neurosurgical consultation, not reviewed in the next available outpatient slot.
Scenario C: A 12-year-old boy is brought to your clinic with a painful, swollen right upper arm one day after falling off a bicycle. The X-ray shows a supracondylar fracture with significant displacement. On examination, the radial pulse is present but the hand is pale and the first web space is numb. What is the referral priority?
Discussion: The presence of pallor and first-web-space numbness (indicating anterior interosseous nerve or median nerve compromise) in the context of a displaced supracondylar fracture is an emergency. The radial pulse being present does not exclude brachial artery kinking or impending thrombosis. This pattern — displaced supracondylar fracture + neurological deficit + pallor — requires emergency orthopaedic management (often urgent closed reduction and percutaneous Kirschner wire fixation, with vascular surgery on standby) within hours. This is a Category 1 referral: the patient should not wait at your facility for observation.
After working through these scenarios, reflect: for which emergency type do you feel least confident in identifying the critical warning signal? Prioritise that category for targeted review.
Urgency Cues and Referral Levels in Orthopaedic Red Flags
CLINICAL PEARL
The most dangerous moment in orthopaedic referral counselling is when the patient seems to accept referral but asks to 'just go home first to collect some things.' For vascular injuries with absent distal pulse and for suspected cauda equina syndrome, there is no safe interval between your clinic and the receiving hospital. In these cases, call the ambulance service (108) from your clinic, call ahead to the receiving team, and give the referral letter to the accompanying family member — not to the patient who may 'lose' it in transit. Document in your notes the time of referral, the name of the person you spoke to at the receiving centre, and the transport arranged. That documentation protects the patient and protects you.