Page 6 of 18
OR2.15 | Open Fracture Infection Prevention — SDL Guide (Part 2)
Emergency Management -- Antibiotics, Tetanus, and Wound Care
The three immediate non-surgical priorities for an open fracture are antibiotics, tetanus prophylaxis, and wound care. These must be initiated in the emergency department immediately upon clinical assessment and must not be deferred until the patient reaches the operating theatre. Deferring any one of these three priorities multiplies the subsequent infection risk in a way that no degree of surgical skill during debridement can fully reverse.
Antibiotics should be administered within 1 hour of presentation -- this is the current evidence-based standard that has replaced the older and now-obsolete concept of 'debridement within 6 hours' as the primary determinant of infection risk. The biological rationale is well-established: bacteria introduced at the time of injury begin adhering to devitalised tissue, fibrin, and any metalwork within minutes of inoculation; biofilm formation that renders the organisms resistant to both antibiotics and host phagocytes is substantially established within a few hours. The goal of early systemic antibiotics is therefore to suppress the initial inoculum before this biofilm-protected state is reached, not to sterilise a fully established infection -- which antibiotics cannot do without surgical source control. The antibiotic regimen is graded by wound classification and contamination type:
- Grade I and II: first-generation cephalosporin (cefazolin 1-2 g IV) provides adequate Gram-positive (especially staphylococcal) coverage. Continue for 24-48 hours post-surgery.
- Grade III: add an aminoglycoside (gentamicin) for Gram-negative coverage. Continue 48-72 hours post-debridement.
- Farm/soil contamination or vascular injury: add penicillin (high-dose benzylpenicillin) for clostridial coverage against gas gangrene (Clostridium perfringens).
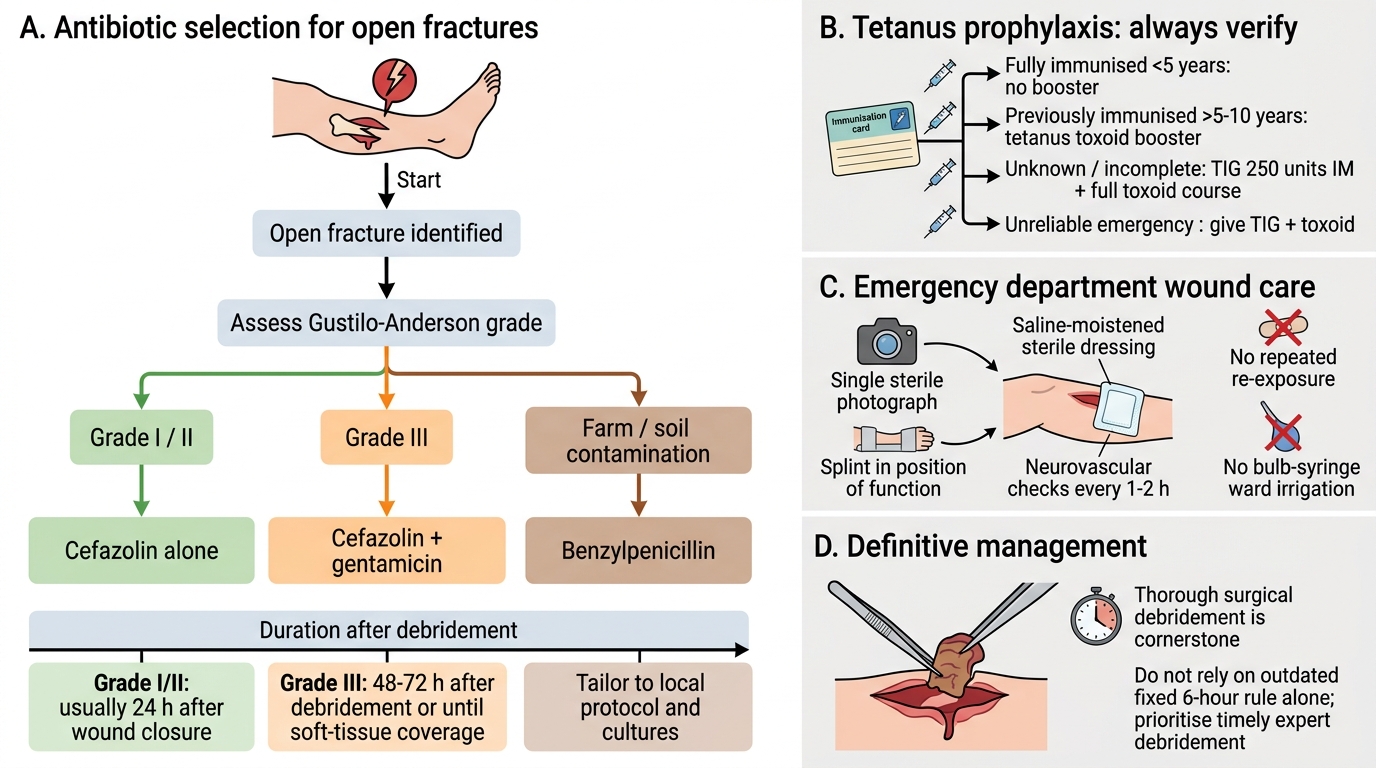
Open Fracture Antibiotic and Initial Care Flowchart
Tetanus prophylaxis must be verified and provided regardless of the wound grade. The protocol depends on immunisation history: if fully immunised (<5 years), no additional action is needed; if previously immunised but more than 5-10 years ago, give a tetanus toxoid booster; if immunisation status is unknown or incomplete, give tetanus immunoglobulin (TIG) 250 units IM plus a full course of toxoid. In emergency presentations where history is unreliable, err toward giving both TIG and toxoid.
Wound care in the emergency department means: (1) a single sterile photograph of the wound for documentation; (2) covering with a saline-moistened sterile dressing to prevent desiccation of viable tissue; (3) NO repeated re-exposure for clinical curiosity; (4) NO ward-level wound irrigation with bulb syringes (historically practised, now shown to be ineffective and potentially harmful by dislodging clots); (5) splinting of the limb in a position of function with neurovascular checks every 1-2 hours until surgery.
Surgical Management -- Debridement Timing and Principles
The cornerstone of open-fracture management is thorough surgical debridement. The old teaching that 'debridement must be performed within 6 hours' has been revised by evidence showing that the actual infection risk is determined more by the grade of contamination, adequacy of debridement, and early antibiotic administration than by a strict 6-hour ceiling. Current guidelines state that debridement should be performed as early as feasible, ideally within 6-12 hours for heavily contaminated wounds, but that a slightly longer delay (e.g. waiting for daylight hours with a full surgical team) is preferable to performing inadequate debridement by a junior team in the middle of the night. For low-energy Grade I and II fractures with minimal contamination and early antibiotic cover, a delay to the next available operating list is now considered acceptable by most guidelines. The principles of debridement are:
- Wound extension: the skin edges are extended (not excised) to allow adequate visualisation of all soft-tissue planes.
- Systematic zone-by-zone debridement: skin -- subcutaneous fat -- fascia -- muscle (assessed by the 4 Cs: colour, consistency, contractility, capacity to bleed) -- periosteum -- bone. Devitalised tissue in each zone is excised. Bone fragments without soft-tissue attachment are removed (avascular sequestra); large fragments with soft-tissue pedicles are retained.
- Irrigation: high-volume saline irrigation (3-9 litres depending on grade) using a pulsatile lavage or gravity-flow system. High-pressure pulsatile lavage is now controversial and not universally recommended; gravity-flow bulb irrigation is acceptable and safer for tissue viability.
- Wound closure decision: Grade I can be closed primarily if debridement is thorough. Grade II wounds should generally be left open for 48 hours and reassessed at a second-look procedure. Grade III wounds are never closed primarily -- soft-tissue reconstruction is planned as a staged procedure.
Skeletal stabilisation is performed at the same sitting, typically by external fixation for Grade II-III injuries (maintains alignment, allows wound access, avoids implant in contaminated field) or intramedullary nailing for low-energy Grade I fractures in experienced centres.
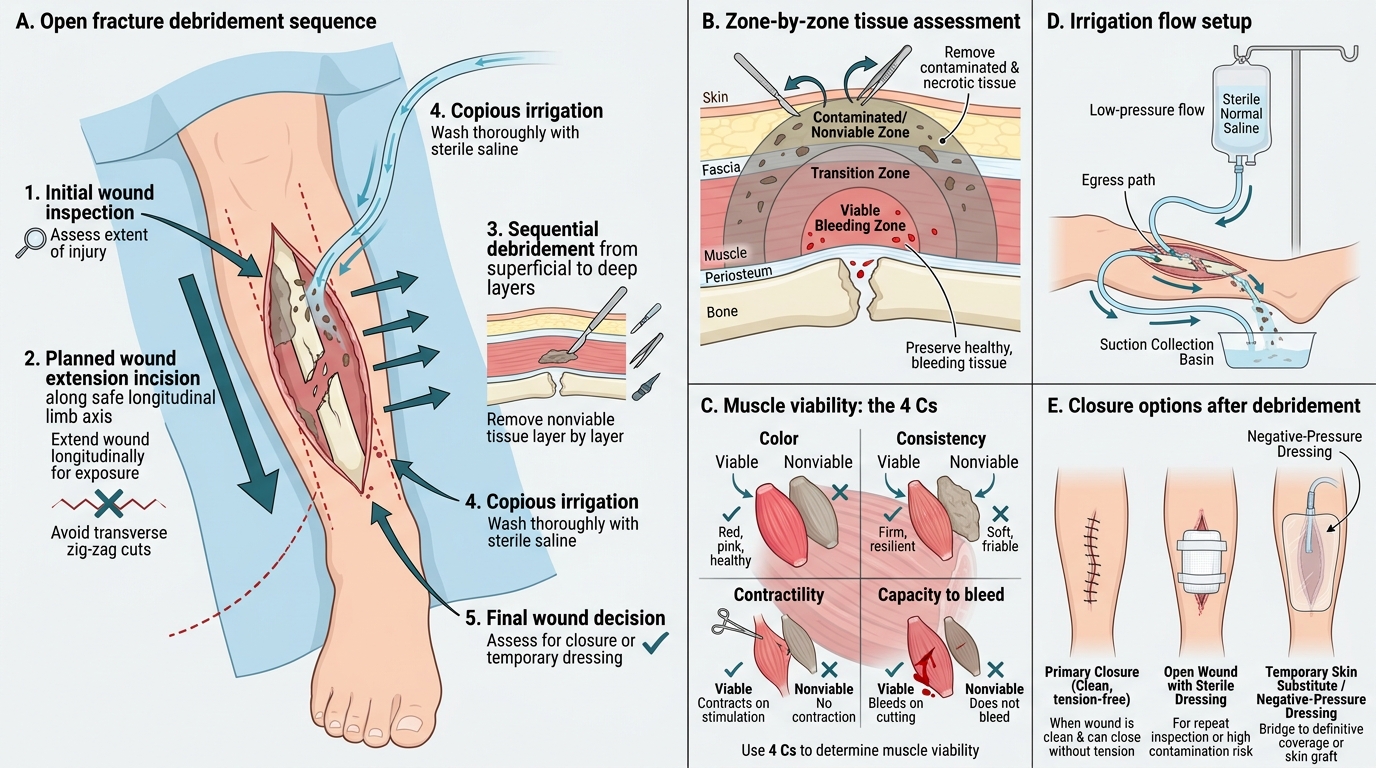
Open Fracture Debridement: Step-by-Step Overview
Self-Assessment: Open Fracture Recognition and First-Hour Priorities
This section tests your consolidation of the core open-fracture management framework developed across this module. When you encounter an open fracture in clinical practice, the management is time-critical and protocol-driven -- the actions you take in the first sixty minutes have a greater impact on the likelihood of deep infection than the choice of implant or the elegance of the surgical technique. A systematic first-hour approach covers the following steps in order of priority: classify the wound using the Gustilo-Anderson system (remembering to defer final grading to the operating theatre); assess and document the neurovascular status of the distal limb, particularly recognising that Grade IIIC is defined by arterial injury requiring repair; administer grade-directed antibiotics within 1 hour of presentation (Grade I/II = cefazolin alone; Grade III = cefazolin plus gentamicin; farm or soil contamination = add benzylpenicillin for clostridial cover); verify and document tetanus immunisation status and provide prophylaxis as required; apply a single sterile saline-moistened dressing without repeated re-exposure; splint the limb in a position of function; and arrange emergency debridement as early as feasible with an adequate surgical team. The obsolete fixed 6-hour rule should never be cited as current practice -- the evidence base for antibiotic timing within 1 hour is far stronger than any fixed debridement-timing rule.
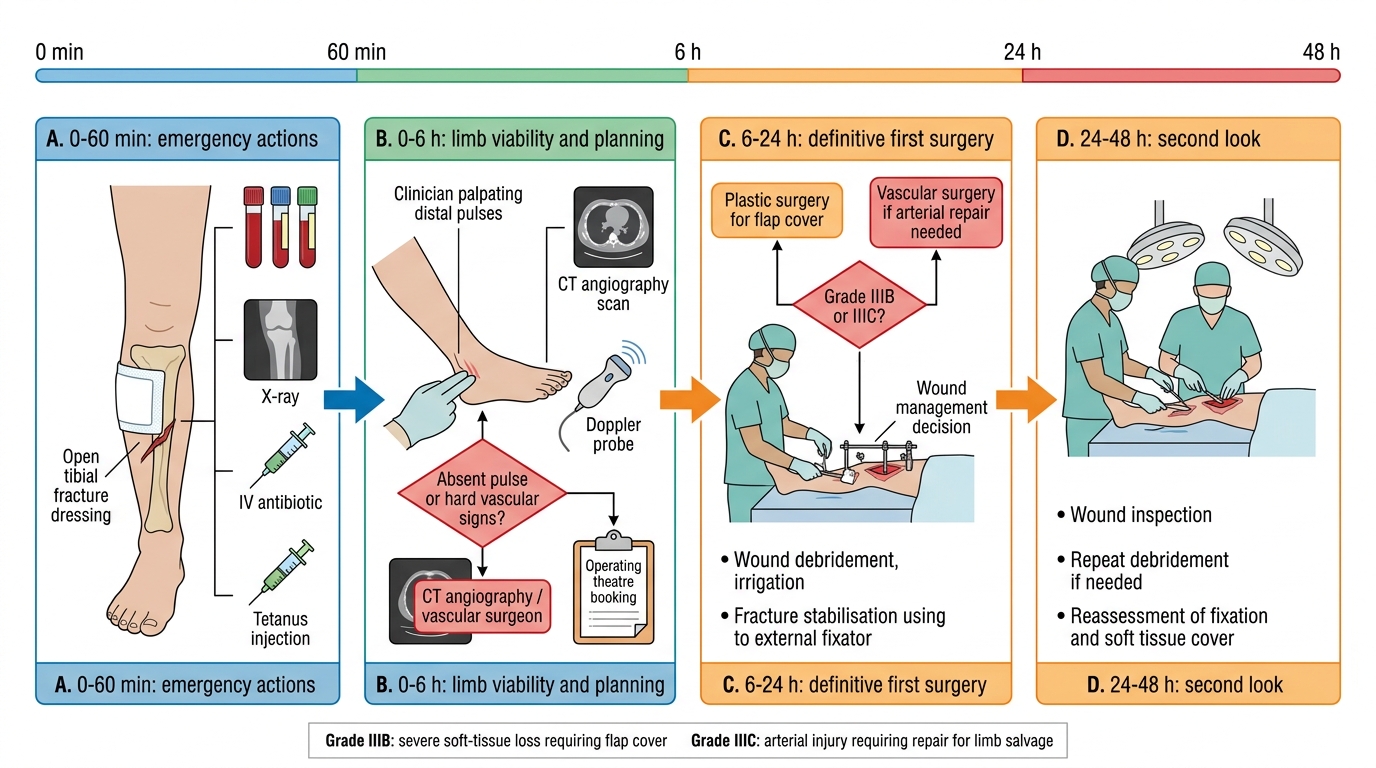
First 24-48 Hours of Open Fracture Management
Test yourself: (1) What is the defining feature that distinguishes Grade IIIC from Grade IIIB open fractures? (Answer: Grade IIIC has an arterial injury requiring repair for limb salvage -- the wound size and soft-tissue damage criteria may be identical; it is the vascular injury that defines the grade.) (2) A farmer falls off a tractor and sustains an open tibial fracture with a 3 cm wound contaminated with soil and manure. What additional antibiotic should be added beyond the standard Grade II regimen, and why? (Answer: Add high-dose benzylpenicillin for clostridial coverage against gas gangrene -- farm and soil contamination carries a high risk of Clostridium spore inoculation.) (3) Why should wound cultures taken at the emergency department NOT be used to direct antibiotic therapy for open fracture infection? (Answer: The organisms colonising the wound surface at the time of injury are not the same organisms that eventually infect the bone -- delayed infection is typically with hospital-acquired pathogens such as MRSA and Gram-negative rods acquired during the surgical admission, not the original environmental contaminants.)
CLINICAL PEARL
The two most dangerous errors in open fracture management are: (1) reassurance based on a present distal pulse, and (2) delaying antibiotics until the operating theatre. A present pulse does not exclude arterial injury -- intimal tears can thrombose over hours. Assess the ABI; if <0.9, pursue CT angiography urgently. And antibiotics within 1 hour are the single most powerful modifiable factor in reducing deep infection after open fracture. The old fixed 6-hour debridement rule is obsolete -- adequate early antibiotic cover has decoupled debridement timing from infection risk more than any surgical technique.