Page 8 of 18
OR2.16 | Paediatric Orthopaedic Injury Patterns — SDL Guide
Learning Objectives
- Describe the unique anatomical and biomechanical features of the paediatric skeleton that make children's fractures differ from adult fractures
- Diagnose supracondylar humerus fracture and identify the associated neurovascular complications, specifically median nerve/AIN injury and brachial artery injury with compartment syndrome risk
- Classify Salter-Harris epiphyseal injuries (Types I-V) using the SALTR mnemonic and explain the implications of each type for growth disturbance
- Recognise forearm and distal radius fracture patterns specific to children, including pulled elbow (radial head subluxation) and its reduction technique
- Outline the management principles for each injury type, including indications for urgent operative intervention
INSTRUCTIONS
Children's bones are biologically different from adults' and break differently. The growth plate is the weakest link in the paediatric skeleton, making epiphyseal injuries the defining trauma pattern of childhood. Missing a supracondylar humerus fracture complication -- particularly a brachial artery injury combined with median nerve deficit and compartment syndrome -- can result in Volkmann's ischaemic contracture, a devastating and largely preventable outcome. This module teaches you to identify, classify, and initiate management for the three most important paediatric orthopaedic injury groups: supracondylar fractures, forearm injuries including pulled elbow, and Salter-Harris physeal injuries.
References
- Maheshwari's Essential Orthopaedics, 5th ed., Ch. 28 — Fractures in Children (textbook)
- Apley & Solomon's System of Orthopaedics and Trauma, 10th ed., Ch. 24 — Children's Fractures (textbook)
- Ebnezar's Textbook of Orthopaedics, Ch. 31 — Paediatric Fractures (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 6-year-old boy falls from a climbing frame onto his outstretched right hand. He is crying and holding his arm in mild flexion. In the emergency department, his forearm is mildly swollen, he has pain on passive finger extension, and his radial pulse is weak but palpable. His fingers on the right hand are slightly pale and he winces when you gently extend them. What fracture do you suspect, what specific nerve do you test first, and does the presence of a weak radial pulse reassure you about the vascular status?
WHY THIS MATTERS
Paediatric orthopaedic injuries are not simply 'smaller versions' of adult fractures. The growing skeleton has unique structural vulnerabilities -- particularly the physis (growth plate) -- that create injury patterns absent in adults, and complications that are uniquely severe. Supracondylar humerus fractures are the most common elbow fractures in children and carry a disproportionately high risk of neurovascular injury. Volkmann's ischaemic contracture, resulting from missed anterior interosseous nerve deficit and brachial artery compromise in the context of compartment syndrome, is one of the most devastating preventable complications in paediatric orthopaedics. Every final-year student must be able to assess the neurovascular status of the hand after elbow injury in a child and act on what they find.
RECALL
Recall from your anatomy studies: the anterior interosseous nerve (AIN) is the motor branch of the median nerve arising in the forearm, supplying flexor pollicis longus, pronator quadratus, and the index finger flexor digitorum profundus -- tested by asking the patient to make an 'OK sign' (tip-to-tip pinch). The brachial artery lies anterior to the elbow, closely related to the medial epicondyle and vulnerable in supracondylar fractures. From your physiology: the anterior compartment of the forearm is a closed fascial space -- if perfusion is compromised, intracompartmental pressure rises, further impairing perfusion and causing ischaemic muscle necrosis. A present (but weak or dampened) radial pulse does not exclude ischaemia.
Supracondylar Humerus Fracture -- Clinical Presentation
Supracondylar humerus fracture is the most common fracture around the elbow in children, accounting for approximately 60% of all paediatric elbow fractures, with peak incidence between 5 and 8 years of age. It occurs almost always from a fall on the outstretched hand (FOOSH mechanism), in which the hyperextension force transmitted through the elbow causes the distal humerus to fracture through the thin supra-condylar region -- the weakest bony region just above the condyles. In approximately 95-97% of cases the distal fragment displaces posteriorly (extension type, Gartland classification); the remaining minority are flexion-type (anterior displacement) with a higher risk of ulnar nerve injury. The typical clinical presentation is a child holding the arm in slight flexion, with a diffuse posterior elbow swelling ('S-sign' or 'swelling in the cubital fossa'), point tenderness just above the lateral and medial condyles, and pain that is dramatically worsened by any attempt at passive extension. The child is usually distressed and protective of the arm. The key clinical lesson at presentation is that the neurovascular examination must be performed before any immobilisation, sedation, or attempted reduction, because the initial findings serve as both a diagnostic guide and a medicolegal baseline.
Radiographic Signs and Neurovascular Risk in Supracondylar Humerus Fracture
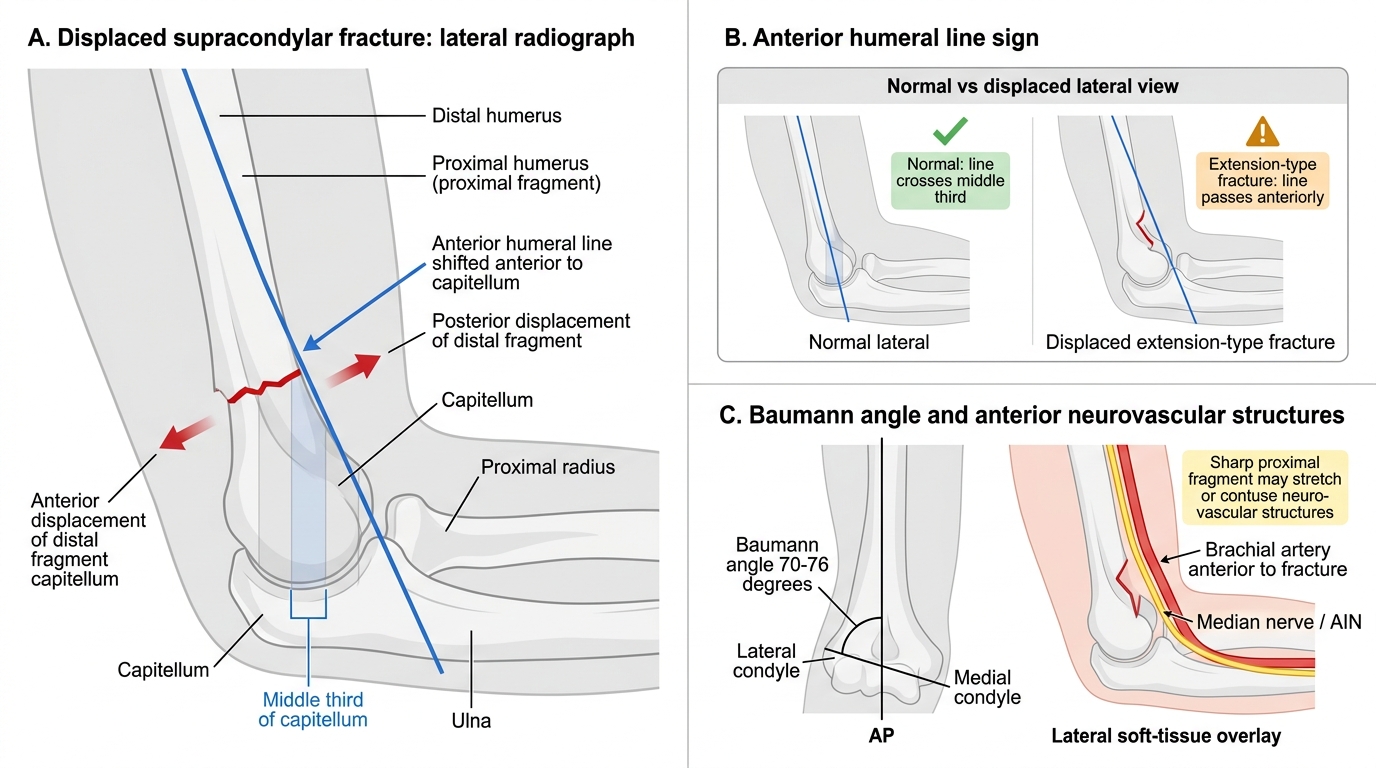
The anterior humeral line (drawn along the anterior cortex of the humerus on a lateral radiograph) normally passes through the middle third of the capitellum. In a displaced extension-type supracondylar fracture, this line passes anterior to the capitellum or through its anterior third -- a reliable radiological sign of posterior displacement. Baumann's angle (the angle between the physeal line of the lateral condyle and the long axis of the humerus on the AP view, normally 70-76 degrees) assesses varus/valgus alignment and guides reduction.
Supracondylar Fracture -- Neurovascular Complications
The neurovascular complications of supracondylar humerus fractures are the most clinically significant aspect of this injury and must be systematically assessed in every case. The anterior interosseous nerve (AIN), the motor branch of the median nerve arising in the proximal forearm, is the most commonly injured nerve -- it is stretched or contused by the anteriorly displaced proximal fragment. AIN palsy presents as inability to perform the 'OK sign' (tip-to-tip pinch between thumb and index finger) because the flexor pollicis longus and the index flexor digitorum profundus are paralysed. The thumb assumes a flat (extended) position rather than the normal flexed-tip posture. Sensation is spared because the AIN carries only motor fibres -- this is a pure motor deficit and should not be confused with complete median nerve palsy. Complete median nerve injury (less common but more serious) additionally impairs sensation over the radial three-and-a-half fingers and causes weakness of the thenar muscles and wrist flexors.
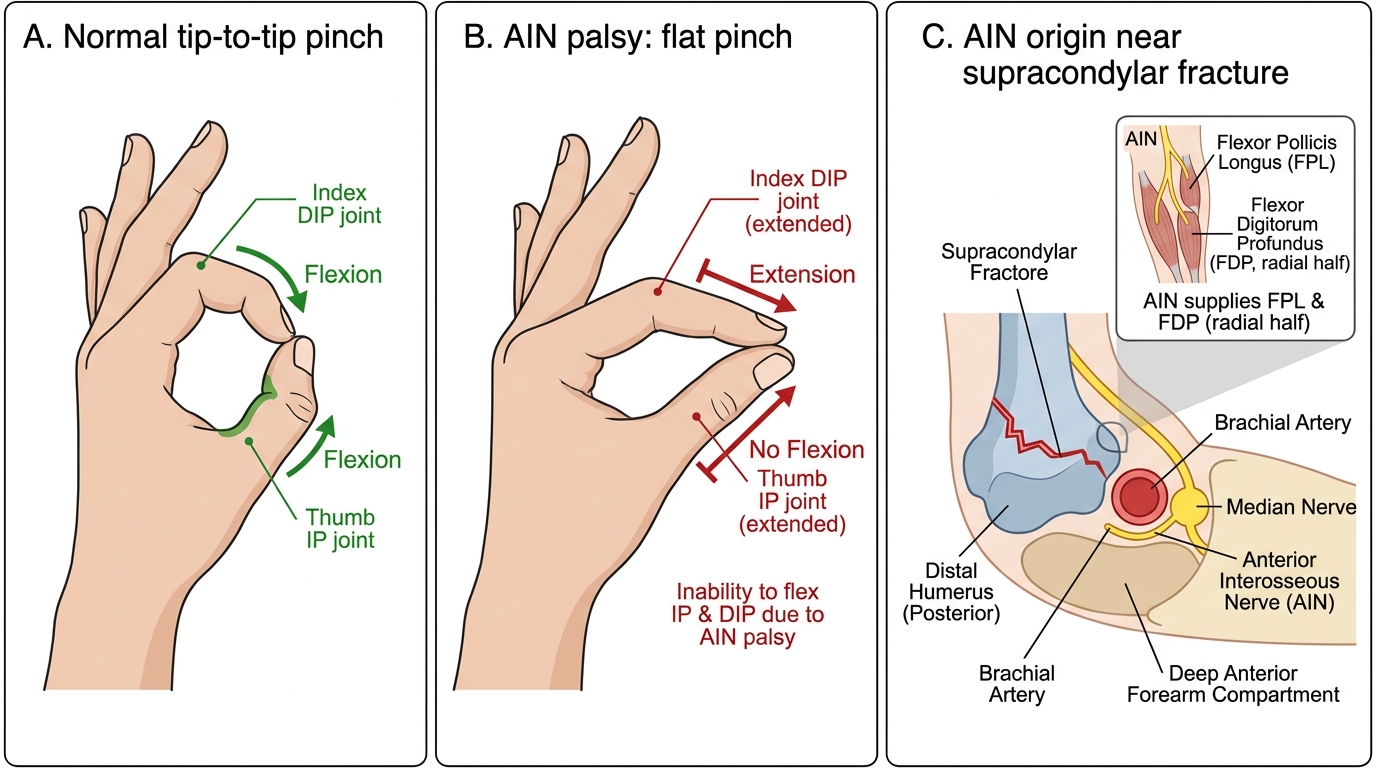
AIN Palsy: Normal OK Sign Versus Flat Pinch
The brachial artery is the most critical vascular structure at risk. It passes anterior to the elbow joint directly in front of the fracture site and can be stretched, contused, kinked, or lacerated by the displaced proximal fragment. Assessment of the brachial artery status combines pulse palpation, Doppler examination, and capillary refill. A critical distinction is the concept of the 'pink, pulseless hand': when the brachial artery is spastic or kinked but not completely transected, the hand may be pink and warm with adequate collateral flow through the recurrent radial and ulnar arteries, yet the radial pulse is absent. This scenario does NOT exclude arterial injury and requires urgent operative exploration after reduction -- a pink pulseless hand that does not reperfuse after reduction must be explored. The 6 Ps of compartment syndrome -- pain (disproportionate, and on passive stretch of finger flexors = earliest sign), pallor, paraesthesia, pulselessness, paralysis, and pressure -- must be serially assessed. Missing an evolving compartment syndrome in the setting of a supracondylar fracture leads to Volkmann's ischaemic contracture, a fibrotic replacement of the flexor compartment muscles with permanent claw-hand deformity. The compartment pressure threshold for fasciotomy (>30 mmHg, or delta P <30 mmHg) applies equally in children.
Supracondylar Fracture -- Investigation
Investigation begins with plain radiographs of the elbow in AP and lateral projections -- crucially, the lateral view must be a true lateral with the elbow in approximately 90 degrees flexion to accurately assess the anterior humeral line. The Gartland classification (used for extension-type fractures) guides management: Gartland I = non-displaced (anterior humeral line intact); Gartland II = displaced but with posterior cortex intact (the distal fragment hinges on the posterior cortex); Gartland III = completely displaced with no cortical contact. For vascular assessment, bedside Doppler examination and pulse oximetry on all five fingers are performed; if the pulse is absent after reduction, CT angiography or operative exploration is undertaken urgently. MRI has no role in the acute setting. Nerve conduction studies are reserved for cases where neurological recovery is not occurring at 8-12 weeks post-injury.
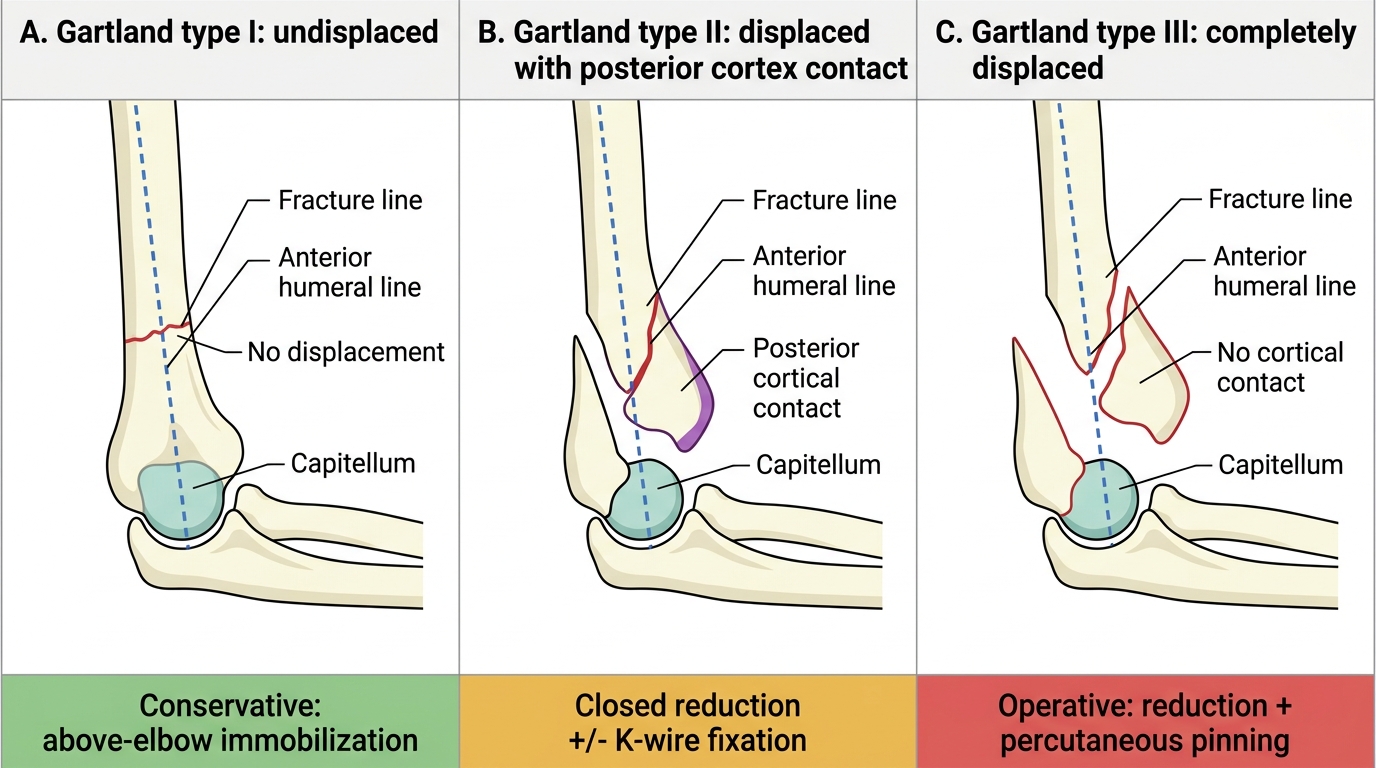
Gartland Classification of Supracondylar Humerus Fractures