Page 10 of 18
OR2.16 | Paediatric Orthopaedic Injury Patterns — SDL Guide (Part 3)
Salter-Harris Classification of Physeal (Growth Plate) Injuries
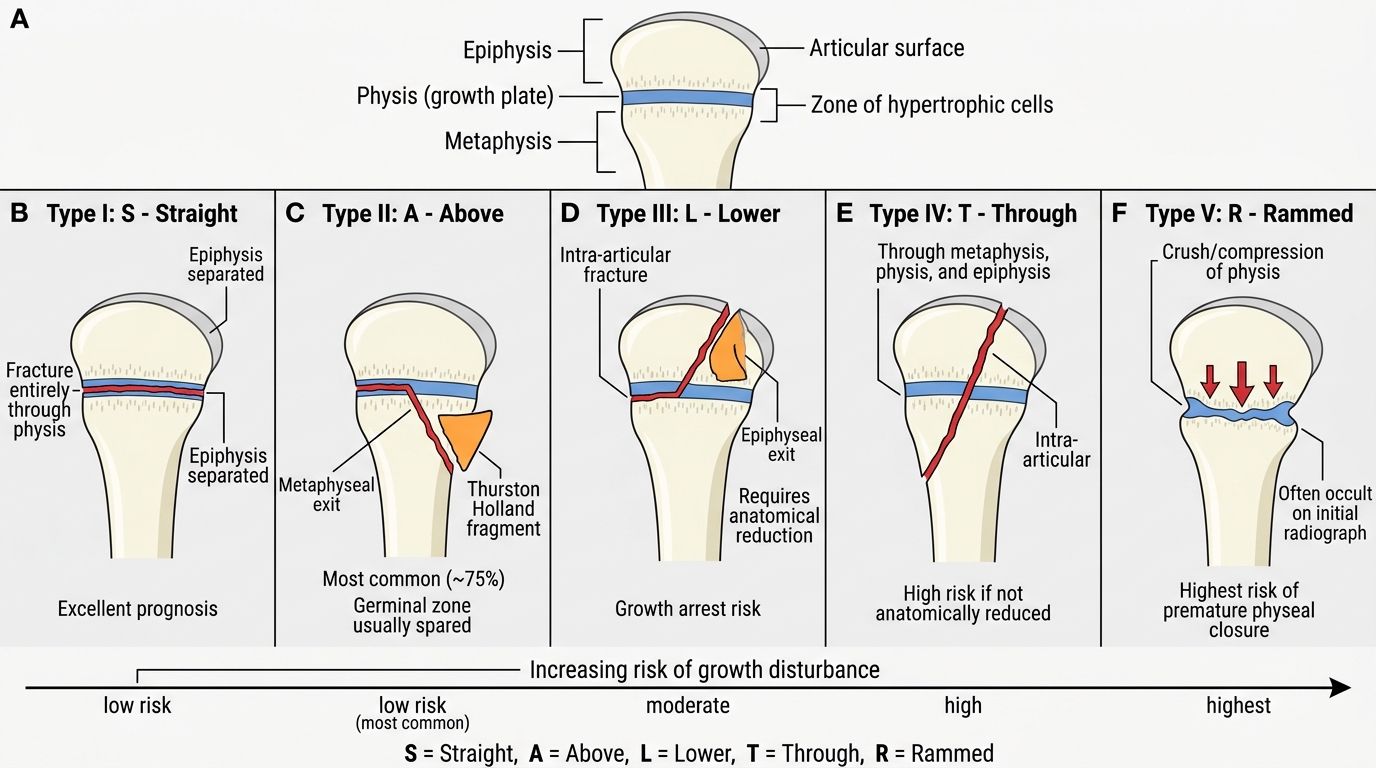
The physis (growth plate, epiphyseal plate) is the cartilaginous zone of proliferating cells between the epiphysis and the metaphysis responsible for longitudinal bone growth. Because it is cartilaginous and has not yet been mineralised, the physis is mechanically the weakest structural region in the paediatric skeleton -- under stress, it fails before the ligaments or adjacent bone cortex. This is why children sustain epiphyseal injuries where adults would sustain ligament sprains. The clinical consequence of physeal injury is the risk of premature growth plate closure, which can cause limb-length discrepancy, angular deformity, or a combination of both, depending on whether the entire or part of the physis is injured. The Salter-Harris classification (1963, Harris and Salter) describes five types of physeal injury based on the relationship of the fracture line to the physis, epiphysis, and metaphysis. A widely used mnemonic is SALTR: S = Straight across (Type I); A = Above (Type II -- metaphyseal fragment; most common, best prognosis); L = Lower/below (Type III -- epiphyseal fragment, enters joint, moderate prognosis); T = Through (Type IV -- crosses physis, metaphyseal AND epiphyseal fragments, requires anatomical reduction); R = Rammed/crushing (Type V -- axial compression injury with no radiological fracture line, worst prognosis).
Salter-Harris Physeal Fracture Classification
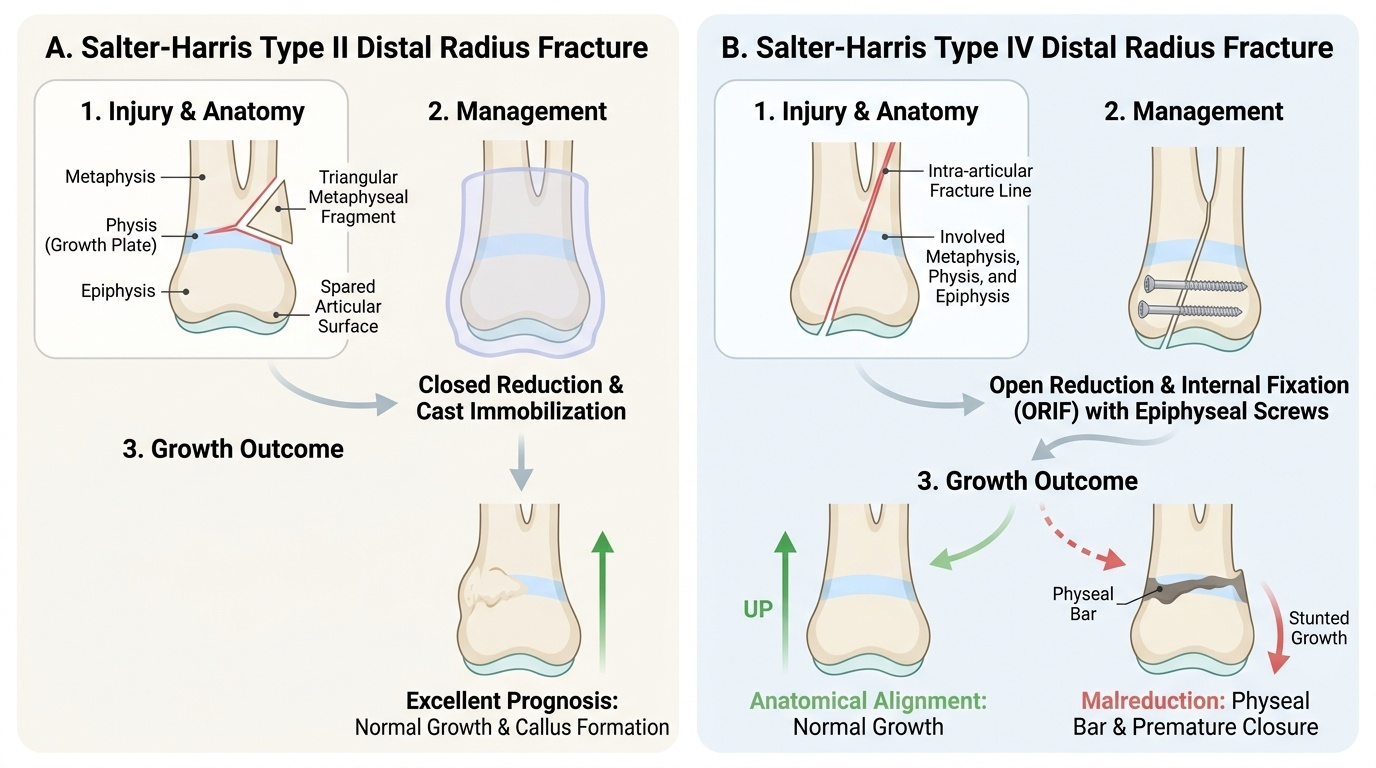
Type I (S -- Straight): fracture line runs entirely through the physis (through the zone of hypertrophic cells). The epiphysis is separated from the metaphysis. Radiographs may appear normal or show only widening of the physis -- this is a clinical diagnosis made by point tenderness directly over the physis. Prognosis is excellent (physis intact, blood supply preserved). Type II (A -- Above): the fracture line runs partly through the physis and then exits through the metaphysis, creating a triangular metaphyseal fragment (Thurston Holland fragment). This is the most common Salter-Harris type (approximately 75% of physeal fractures). Prognosis is excellent because the germinal zone of the physis is not disrupted. Type III (L -- Lower): fracture runs through the physis and then exits through the epiphysis -- an intra-articular fracture. Because the fracture line passes through the physis to reach the epiphysis, the germinal cells may be disrupted locally. Anatomical reduction (often operative) is required to restore the joint surface and prevent growth arrest. Type IV (T -- Through/Across): fracture line crosses the full thickness of the epiphysis, physis, AND metaphysis. This is invariably intra-articular and requires open reduction and internal fixation (ORIF) to achieve anatomical alignment of all three layers -- any residual displacement risks a bony bar forming across the physis, causing angular deformity as the child grows. Type V (R -- Rammed): axial compression of the physis with crushing of the germinal cells. There may be NO radiological fracture line initially (making diagnosis very difficult); the injury is recognised retrospectively when premature physeal closure occurs. Retrospective diagnosis is associated with poor outcome. A high index of suspicion is needed for axial-loading injuries to the physis in a child.
Salter-Harris Injuries -- Investigation and Management Principles
Provided image
The investigation of suspected physeal injury begins with plain radiographs in at least two planes. A crucial point in interpretation is to compare the injured side with the contralateral limb -- normal physeal anatomy varies considerably by age and skeletal maturity, and what appears to be widening of the physis may be normal for that age unless comparison films confirm it is abnormal. In Type I injuries, plain films may be entirely normal and the diagnosis is clinical; in these cases, if clinical suspicion is strong, the limb should be immobilised and reassessed at 10-14 days when periosteal new bone formation may confirm the injury site. MRI is the gold standard for imaging when plain films are normal but clinical suspicion of physeal injury persists, as it directly visualises the cartilaginous physis. CT is used in complex fractures (Types III and IV) to plan reduction and implant placement, particularly around the distal tibia and distal humerus. Bone scintigraphy has a role in the diagnosis of stress fractures of the physis in young athletes, but is rarely used in acute trauma.
Management principles are determined by the Salter-Harris type:
- Type I: closed reduction and immobilisation for 4-6 weeks (plaster cast); excellent union rate and growth prognosis.
- Type II: closed reduction and cast immobilisation in most cases; K-wire fixation if the reduction is unstable or cannot be maintained.
- Type III: open reduction and internal fixation (ORIF) required in most cases to restore the articular surface; screws placed within the epiphysis must not cross the physis.
- Type IV: always ORIF to restore all three anatomical layers; screws crossing the physis are acceptable if they are small-diameter cannulated screws that can be removed early.
- Type V: no acute treatment reliably prevents premature physeal closure; treatment is surveillance for growth disturbance and corrective osteotomy or epiphysiodesis of the opposite limb when deformity is established.
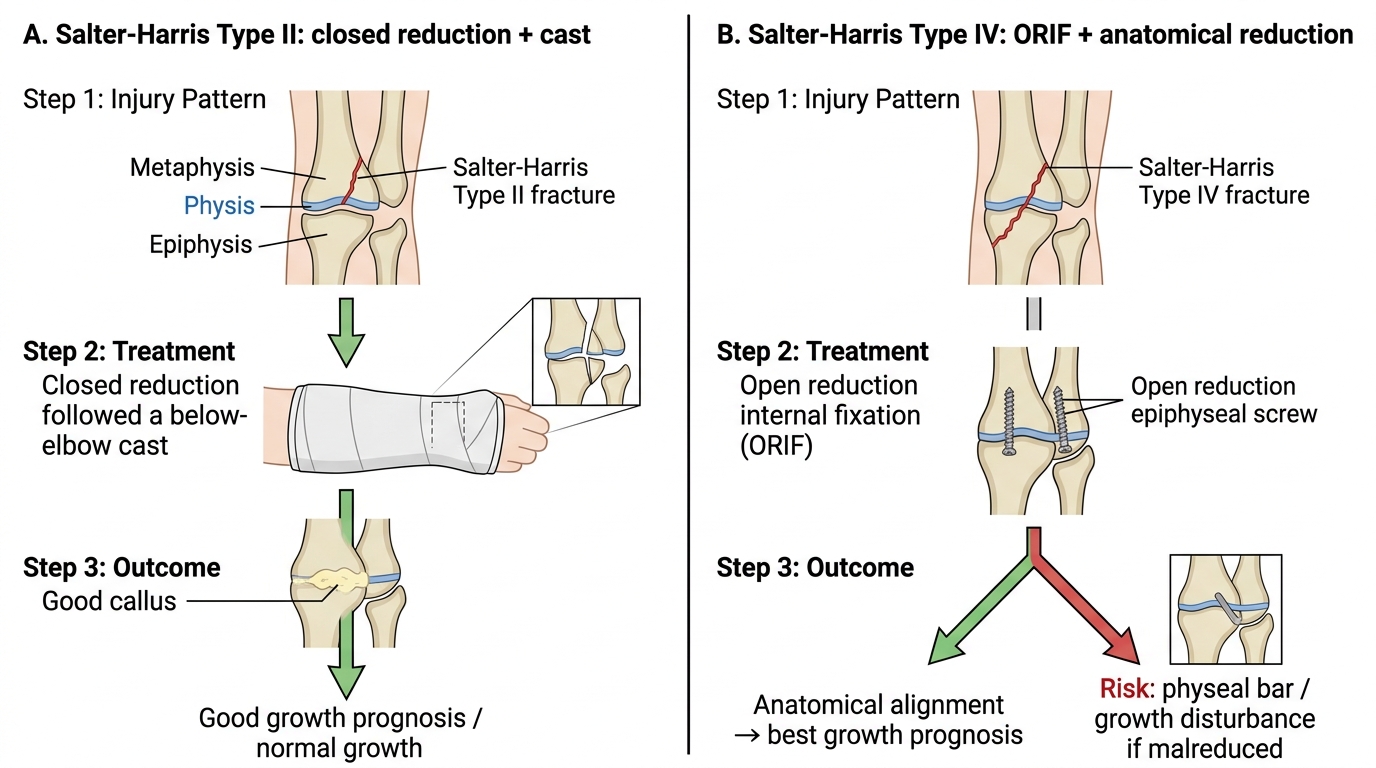
Management and Prognosis of Salter-Harris II vs IV Distal Radius Fractures
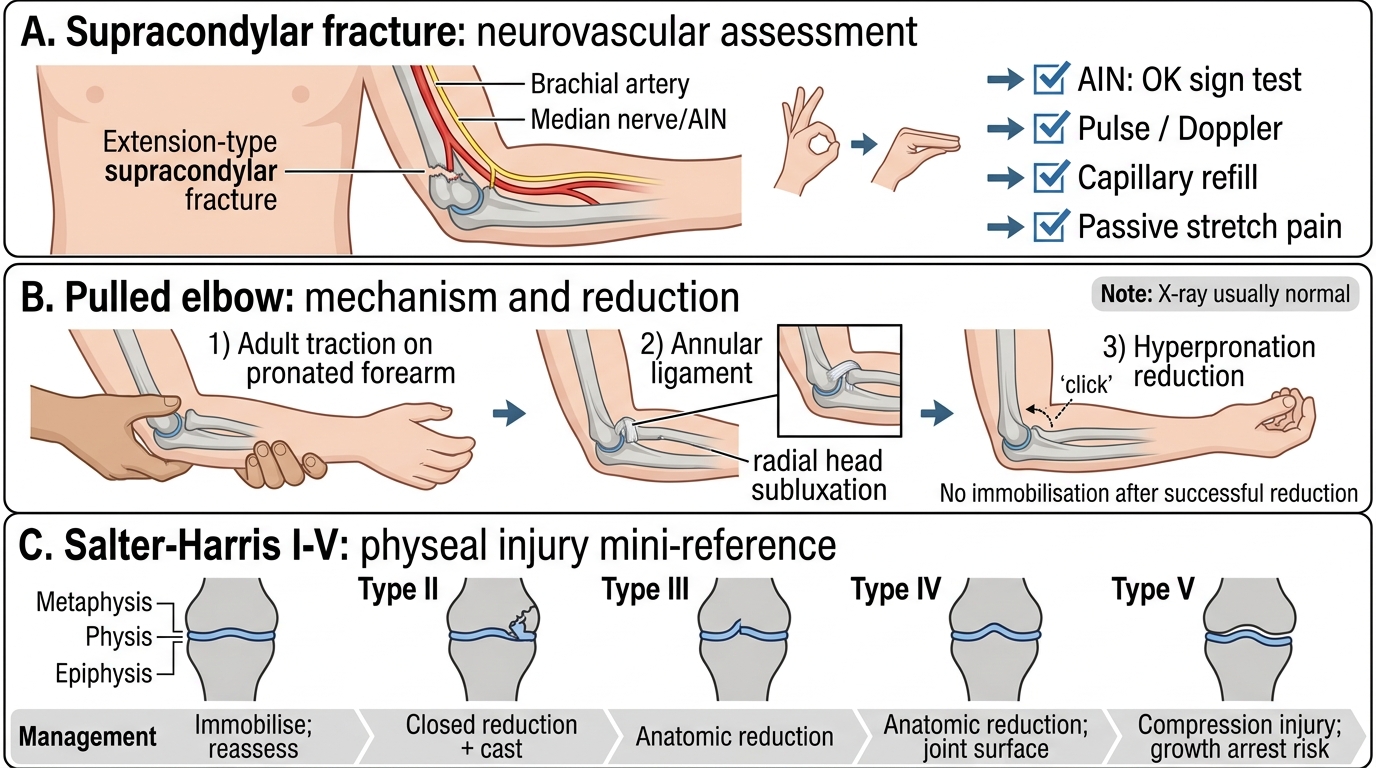
Self-Assessment: Paediatric Fracture Recognition and Neurovascular Assessment
This self-assessment section integrates the three injury groups covered in this module. The most high-stakes clinical skill is the neurovascular assessment after supracondylar humerus fracture: specifically, the AIN test (OK sign -- inability indicates AIN/median nerve injury), brachial artery assessment (pulse quality plus capillary refill plus Doppler), and early compartment syndrome signs (pain on passive finger extension = earliest warning). A present but weak pulse does NOT exclude arterial injury or ischaemia -- the concept of the 'pink pulseless hand' is the key clinical trap. For pulled elbow, the characteristic history (traction on a young child's arm) combined with the position held (pronation and mild flexion) is diagnostic -- no radiograph is needed in classic cases and the only intervention required is reduction using hyperpronation or supination-flexion. For Salter-Harris injuries, the SALTR mnemonic organises both the classification and the management (Types I-II: closed treatment; Types III-IV: operative; Type V: surveillance and late reconstruction).
Paediatric Orthopaedic Injury Assessment Summary
Test yourself: (1) A 6-year-old with a Grade III supracondylar fracture cannot flex the tip of the right index finger independently. Which nerve is affected, what is the specific branch, and what clinical test confirmed the deficit? (Answer: Median nerve -- specifically the anterior interosseous nerve (AIN), which supplies flexor pollicis longus and the index flexor digitorum profundus. The 'OK sign' test -- asking the child to form a circle with thumb and index fingertip -- revealed inability to flex the index tip, producing a flat pinch rather than a rounded O.) (2) A 3-year-old is brought in crying after her father 'yanked her arm' while she was trying to run away. She holds her arm pronated at the side and screams when you try to supinate it. X-ray is normal. What is the diagnosis, and what do you do? (Answer: Pulled elbow -- radial head subluxation with annular ligament entrapment. Perform reduction by hyperpronation with the elbow held at 90 degrees -- a click indicates successful reduction. No immobilisation needed.) (3) A 12-year-old falls on an outstretched hand and has physeal tenderness at the distal radius. X-ray shows a triangular metaphyseal fragment on the ulnar side of the distal radial physis with the epiphysis displaced. What Salter-Harris type is this, what is the prognosis, and what treatment is appropriate? (Answer: Salter-Harris Type II -- the fracture exits through the metaphysis creating the Thurston Holland fragment. Prognosis is excellent as the germinal physis is not disrupted. Closed reduction and cast immobilisation is appropriate in most cases.)
CLINICAL PEARL
Three high-yield clinical pearls for paediatric orthopaedic injuries: (1) In supracondylar fractures, test the AIN (OK sign) BEFORE the radial pulse -- the AIN is the most commonly injured nerve and a subtle motor deficit is easier to miss than an absent pulse. (2) The 'pink pulseless hand' is NOT reassuring -- it means collateral flow is keeping the hand alive while the main artery is compromised; it requires urgent operative attention, not observation. (3) For Salter-Harris injuries, Types I and II have excellent prognosis with closed treatment; Types III and IV require anatomical operative reduction because any residual step at the physis creates a bony bar that causes progressive deformity. Type V (axial compression) often has a normal X-ray acutely -- diagnose it retrospectively when growth arrest becomes apparent.