Page 10 of 22
OR2.13 | Ankle Fracture Management — SDL Guide (Part 2)
Syndesmotic Injuries — Diagnosis and Management
The distal tibiofibular syndesmosis is the fibrous joint between the distal tibia and fibula, held together by four ligaments: anterior inferior tibiofibular ligament (AITFL), posterior inferior tibiofibular ligament (PITFL), inferior transverse ligament, and the distal interosseous membrane. Together, they maintain the mortise width at 4–5 mm (tibiofibular clear space on AP radiograph) and allow 1–2 mm of physiological fibular motion during ankle flexion. Syndesmotic disruption allows the mortise to widen, displacing the talus laterally — even 1 mm of lateral talar shift reduces ankle contact area by approximately 40%, dramatically accelerating post-traumatic arthritis.
Clinical diagnosis: the 'squeeze test' (compress the tibia and fibula together at the mid-leg level — pain distally at the syndesmosis is positive) and the external rotation stress test (dorsiflexion of the ankle combined with external rotation of the foot — pain at the anterior syndesmosis is positive) are the clinical screening tests. Both have moderate sensitivity; combined, they are useful. The 'cotton test' (intraoperative — grasp the heel and apply lateral stress while viewing fluoroscopically for mortise widening) is the definitive intraoperative assessment.
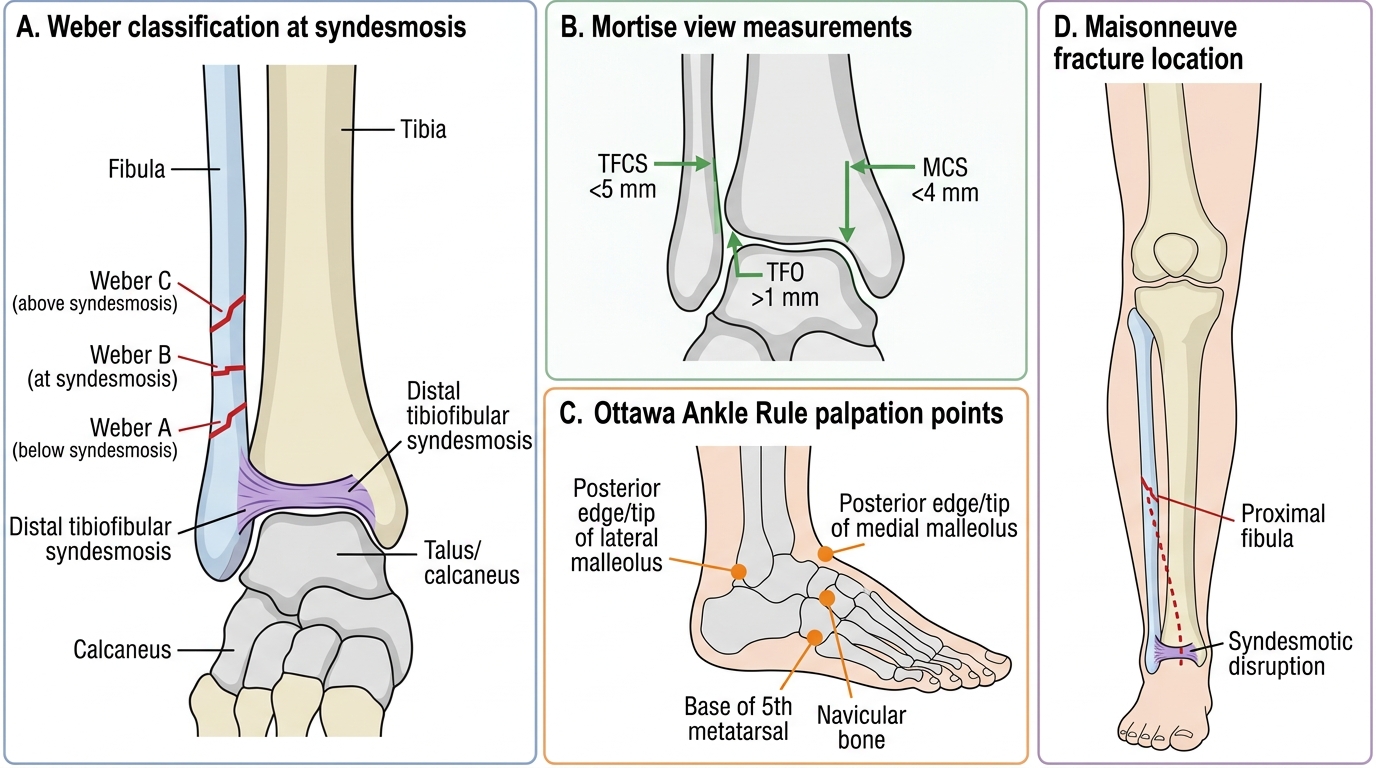
Radiographic diagnosis: standard mortise view (15° internal rotation AP) and lateral ankle X-ray. The tibiofibular clear space (TFCS) — the distance between the medial border of the fibula and the lateral border of the posterior tibial line on the mortise view — should be <5 mm. Tibiofibular overlap (TFO) on the mortise view should be >1 mm and on the AP view >5 mm. Medial clear space (MCS) — the distance between the medial talus and the medial malleolus — should be <4 mm and should equal the superior joint space; a MCS ≥5 mm indicates deltoid disruption. CT and MRI can confirm subtle syndesmotic and deltoid injuries.
Management: isolated AITFL sprains (low-grade syndesmotic sprains, Grade I) are managed with rest and functional rehabilitation. Frank syndesmotic disruption (mortise widening on radiograph, positive cotton test intraoperatively) requires surgical fixation — traditionally trans-syndesmotic cortical screws (spanning 3 or 4 cortices), with removal at 8–12 weeks before weight-bearing; newer suture-button (TightRope) devices are increasingly used as they allow physiological micromotion and do not require removal.
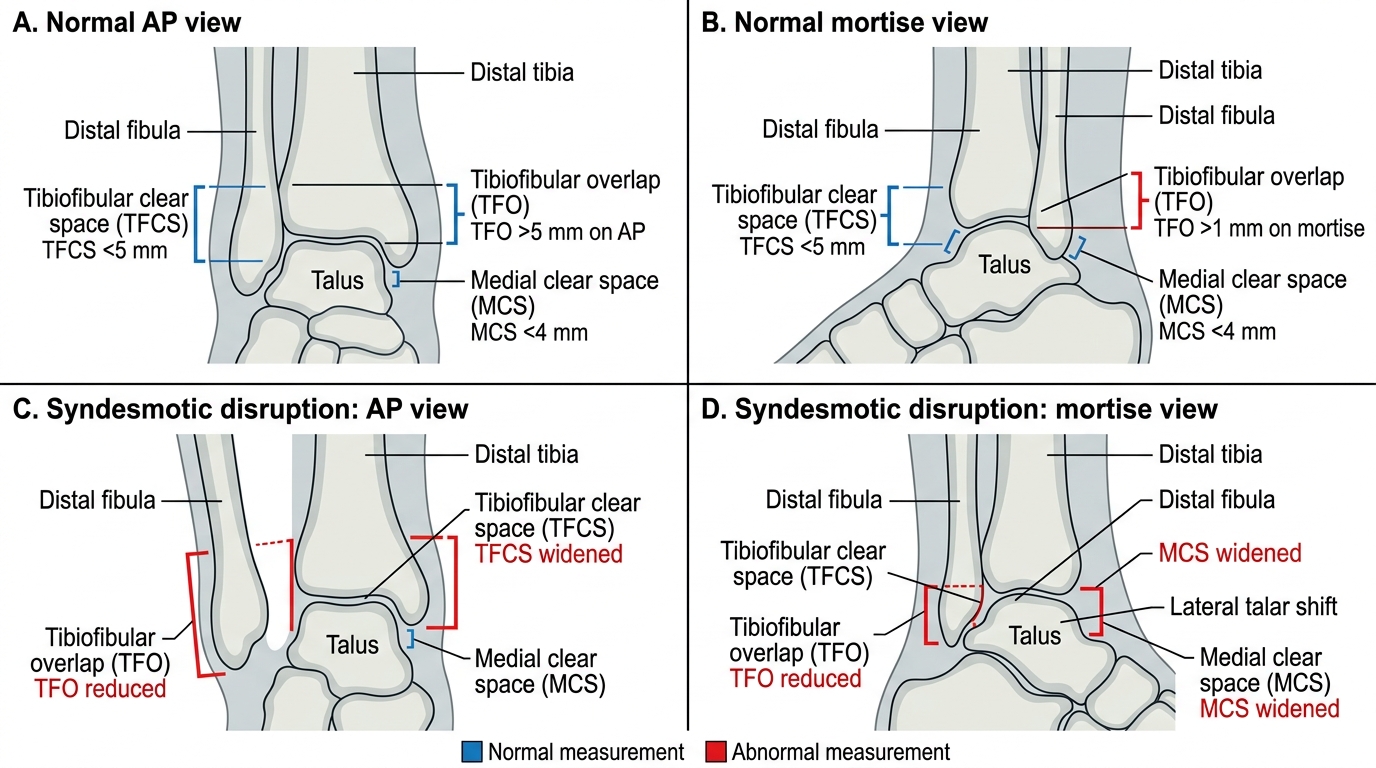
Ankle Syndesmosis Measurements on AP and Mortise Views
Management of Ankle Fractures — Stable versus Unstable
The fundamental question in ankle fracture management is whether the injury is stable or unstable. An unstable ankle fracture is one where the tibiotalar articulation will not remain reduced under physiological loading, predicting malunion and post-traumatic arthritis unless anatomically reduced and held. The following are classified as unstable: bimalleolar fractures (both the medial and lateral malleoli fractured), trimalleolar fractures (medial, lateral, and posterior malleoli), fractures with >1 mm lateral talar shift on mortise view, Weber B fractures with confirmed medial-side disruption, Weber C fractures (nearly all unstable), and Maisonneuve fractures.
Non-operative management is appropriate for: isolated undisplaced lateral malleolus fractures (Weber A or undisplaced Weber B with intact medial side and normal mortise view), confirmed with stress radiographs if necessary. Treatment is a below-knee walking cast or removable aircast boot for 4–6 weeks, followed by physiotherapy. The fracture should be reviewed radiographically at 1 week to confirm no secondary displacement.
Operative management is required for unstable fractures. The standard approach: open reduction and internal fixation (ORIF) under general or spinal anaesthesia. The fibula is fixed first (restores length and rotation of the lateral pillar) with a one-third tubular plate or lag screw, after which the medial malleolus is fixed with two cancellous screws (or a tension band construct). The posterior malleolus is fixed if it is >25% of the articular surface on lateral view and if it is displaced >2 mm (smaller undisplaced posterior fragments do not require separate fixation as they are stabilised by the PITFL attached to the fragment). Syndesmotic fixation is added if the intraoperative cotton test reveals residual mortise instability after fibular fixation.
Post-operatively, the patient is kept non-weight-bearing in a cast or splint for 4–6 weeks, followed by graduated weight-bearing and physiotherapy. Elevation, ice, and strict skin-crease monitoring are essential in the post-operative period because ankle fracture surgery through oedematous tissue is associated with wound-healing complications.
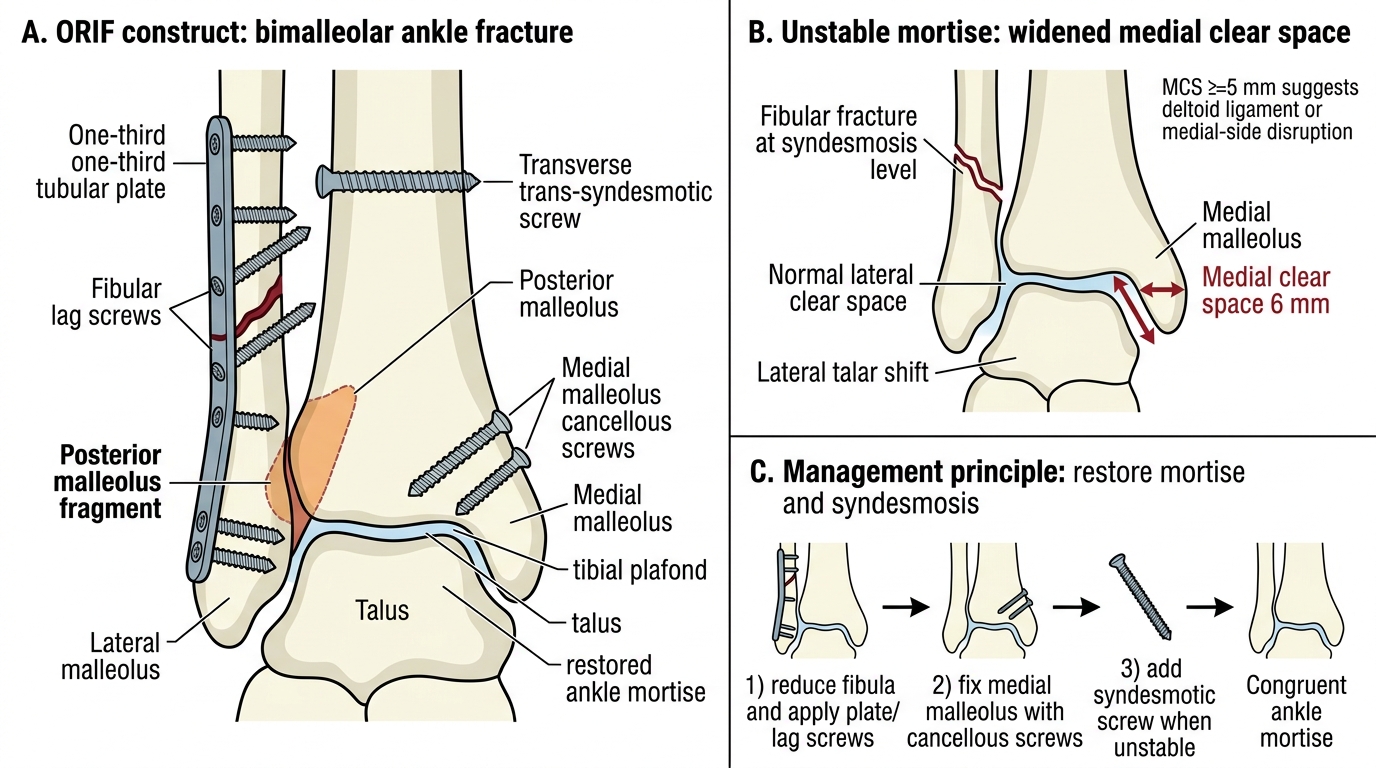
ORIF of Unstable Bimalleolar Ankle Fracture
SELF-CHECK
On the standard mortise view of the ankle, a medial clear space of 6 mm is noted, with a fibular fracture at the level of the syndesmosis. The lateral clear space is normal. What does the widened medial clear space indicate, and how does it affect management?
A. Isolated lateral malleolus fracture — can be managed in a boot
B. Disruption of the deltoid ligament or medial malleolus, indicating an unstable mortise requiring operative fixation
C. Normal anatomical variant, no management change required
D. Posterior malleolus fragment that requires CT for characterisation
Reveal Answer
Answer: B. Disruption of the deltoid ligament or medial malleolus, indicating an unstable mortise requiring operative fixation
The medial clear space (MCS) on the mortise view should be <4 mm (approximately equal to the superior joint space). A MCS ≥5 mm indicates deltoid ligament disruption or a displaced medial malleolus fracture — both signify medial-side injury and ankle mortise instability. A Weber B fibular fracture with medial-side disruption is an unstable SER Stage IV injury requiring ORIF to restore mortise congruence.
Self-Assessment — Ankle Fracture Classification and Management
This self-assessment section consolidates the principal frameworks used in ankle fracture assessment and management that you have studied in this module. Work through the following structured questions to confirm your command of the clinical decision-making process. First, regarding the Ottawa Ankle Rules: state the two specific anatomical palpation sites on the fibula and tibia, the midfoot sites, and the weight-bearing criterion that triggers a radiograph request; identify two patient populations in whom the OAR are not applicable. Second, for the Weber classification: state the fibular fracture level for each of the three categories (A, B, C) relative to the syndesmosis, and explain why a Weber B fracture may be either stable or unstable. Third, for the Lauge-Hansen system: identify which of the four patterns is most common, describe its four stages, and explain what a Stage IV pattern means for management. Fourth, for the syndesmosis: state the three key radiographic measurements on the mortise view (TFCS, MCS, TFO) with their normal thresholds, and explain the clinical significance of a medial clear space of 6 mm. Fifth, describe the operative sequence for ORIF of a trimalleolar fracture and state the criterion for posterior malleolus fixation.
Ankle Fracture Reference: Weber, Mortise, Ottawa Rule, and Maisonneuve
CLINICAL PEARL
Three rules for ankle fractures: (1) Apply the Ottawa Ankle Rules before ordering X-rays — point tenderness at the posterior malleolar edges or inability to weight-bear are the triggers, not just 'ankle pain'; applying the rules saves a third of ankle X-rays. (2) A normal ankle X-ray does not rule out a Maisonneuve fracture — if you see a widened mortise or medial clear space but no visible fibular fracture on standard ankle views, the fibula may be fractured at the proximal end; X-ray the full fibula including the knee. (3) The medial clear space must equal the superior joint space (both <4 mm normally); any asymmetry or value ≥5 mm indicates deltoid disruption and an unstable mortise — do not dismiss this as a 'simple' lateral fracture.