Page 5 of 22
OR2.12 | Leg and Foot Fracture Management — SDL Guide
Learning Objectives
- Describe the mechanism of injury, fracture patterns, and management of fractures of both bones of the leg (tibia and fibula)
- Explain the unique biomechanical and clinical features of calcaneus fractures, including the role of Bohler's angle in assessment
- Outline the management principles for fractures of small bones of the foot — metatarsals and phalanges
- Describe the anatomy, mechanism of injury, diagnosis, and management of Lisfranc fracture-dislocation
- Identify when compartment syndrome of the leg or foot is a risk and outline the principles of fasciotomy
INSTRUCTIONS
Fractures of the leg and foot together represent some of the most common injuries seen in emergency departments worldwide. From the high-energy tibia fracture after a road traffic accident that threatens limb viability, to the missed Lisfranc fracture-dislocation in a footballer that leads to lifelong midfoot arthritis, these injuries span the full spectrum of orthopaedic complexity. Understanding the anatomy, biomechanics, and management principles of this region is essential for every MBBS graduate who will work in any casualty or primary care setting.
References
- Maheshwari's Essential Orthopaedics, Ch 30-31 (textbook)
- Apley & Solomon's System of Orthopaedics and Trauma, 10th ed, Ch 30-31 (textbook)
- Ebnezar's Textbook of Orthopaedics, 5th ed (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 19-year-old cricketer lands awkwardly after jumping and sustains a twisting injury to the forefoot while wearing cleats. He presents to the emergency department with severe midfoot pain, swelling, and an inability to weight-bear. Examination reveals tenderness along the medial aspect of the midfoot at the tarsometatarsal joint and an ecchymosis in the plantar arch — the so-called 'plantar ecchymosis sign'. Plain radiographs are ordered. What fracture-dislocation complex must always be ruled out in midfoot injuries, and what specific radiographic finding would clinch the diagnosis?
WHY THIS MATTERS
Injuries to the leg and foot are ubiquitous in both high-energy trauma (road traffic accidents, falls from height) and sports. The tibia, as the primary weight-bearing bone of the leg, is the most commonly fractured long bone in adults. Calcaneus fractures from falls onto the heel constitute 60% of all tarsal fractures and are notorious for long-term disability if managed suboptimally. The Lisfranc fracture-dislocation is the most commonly missed major foot injury in emergency settings, with missed or delayed diagnosis leading to post-traumatic midfoot arthritis and long-term functional limitation. Competence in recognising, initially managing, and referring these injuries appropriately is a core skill for every MBBS graduate.
RECALL
The leg consists of the tibia (medial, weight-bearing bone) and fibula (lateral strut bone), connected by the interosseous membrane. The tibia transmits approximately 80% of body weight while the fibula bears approximately 15–20%. The blood supply to the tibia enters via the nutrient artery (from the posterior tibial artery) at the posterior tibia between the middle and distal thirds; the proximal third and distal portion are relatively avascular, making them prone to delayed union and non-union. The foot has three functional regions: the hindfoot (calcaneus and talus), the midfoot (navicular, cuboid, and three cuneiforms), and the forefoot (metatarsals and phalanges). The Lisfranc joint (tarsometatarsal joint complex) is the keystone of the medial longitudinal arch, stabilised by the Lisfranc ligament running between the medial cuneiform and the base of the second metatarsal.
Fractures of Both Bones of the Leg — Mechanism, Pattern, and Severity
Both-bone leg fractures (tibia and fibula) are the most common long bone fractures in adults. The tibia, being subcutaneous along its anteromedial surface with minimal soft tissue cover, is particularly vulnerable to open fracture; up to 25% of tibial shaft fractures present as open injuries. The mechanism determines the fracture pattern: direct trauma (road traffic accident, direct blow) produces transverse or short oblique fractures with variable degrees of comminution; indirect twisting forces produce long spiral or oblique fractures; high-energy mechanisms produce comminuted or segmental fractures with extensive soft tissue injury.
The Gustilo-Anderson classification of open fractures is applied to all open tibial fractures: Grade I (wound <1 cm, minimal contamination), Grade II (wound 1–10 cm, moderate contamination), Grade IIIA (wound >10 cm, adequate soft tissue cover feasible), Grade IIIB (wound >10 cm, periosteal stripping, inadequate cover requiring flap), Grade IIIC (vascular injury requiring repair). Grade IIIB and IIIC tibial fractures are among the most challenging injuries in orthopaedics, often requiring the combined input of the orthopaedic surgeon, plastic surgeon, and vascular surgeon.
Isolated fibula shaft fractures are much less common and often result from direct blows; the fibula is non-weight-bearing alone, and if the tibia is intact, the patient can bear weight — although pain and swelling localised to the fibular shaft should prompt X-ray to confirm isolated fibula fracture and rule out a complex proximal injury pattern.
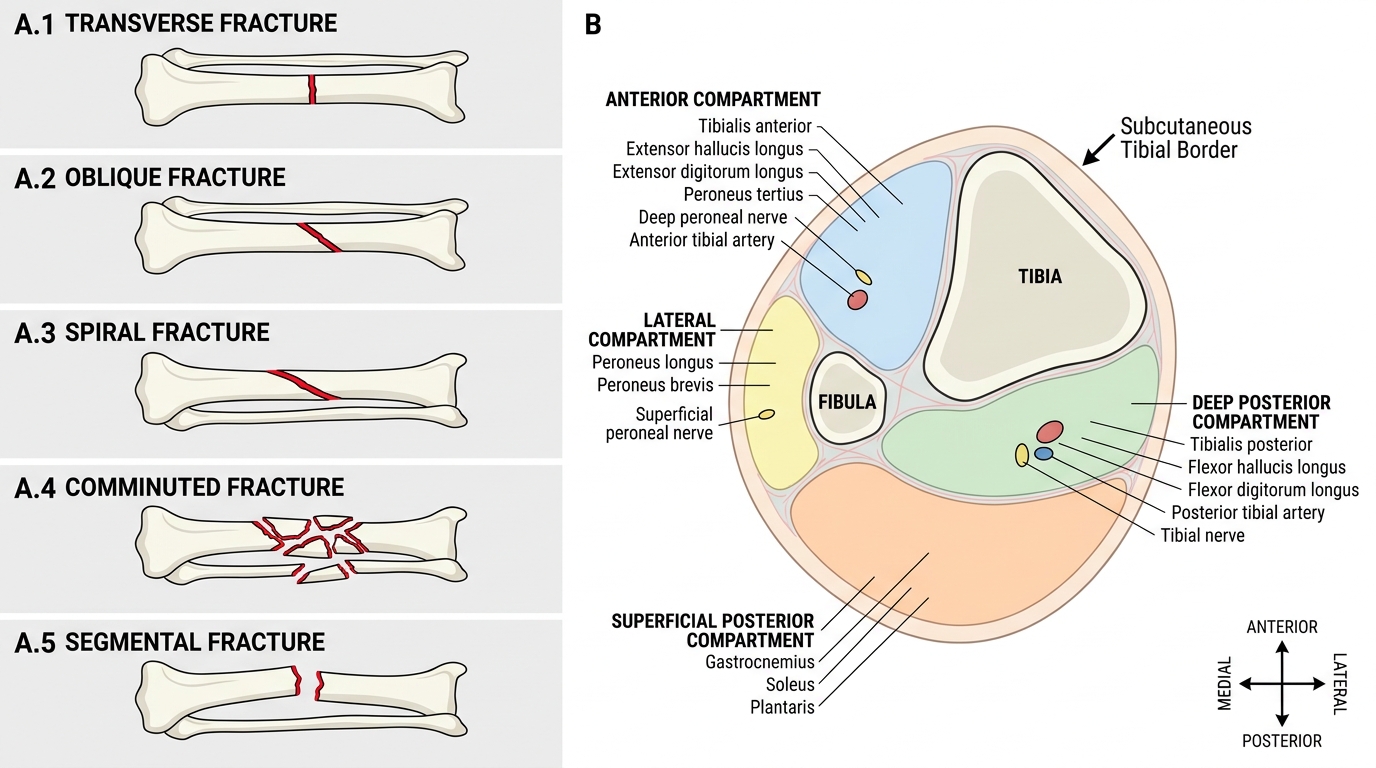
Tibial Shaft Fracture Patterns and Leg Compartments
Both-Bone Leg Fractures — Investigation and Management
Provided image
Plain radiographs of the leg (full tibia and fibula, AP and lateral, including the knee and ankle joints) are the initial investigation. The proximal and distal joint views are essential because associated knee or ankle injuries (proximal fibular fracture in Maisonneuve pattern; plafond fracture) may radically change the management plan. CT is indicated for complex fractures involving the tibial plafond.
Non-operative management is appropriate for closed, undisplaced or minimally displaced tibial shaft fractures with acceptable alignment — less than 5° angulation in any plane, <1 cm shortening, and <10° rotation. Management consists of a long-leg cast (above-knee) for 4–6 weeks until early callus formation, followed by a patellar tendon-bearing (PTB) cast. Weight-bearing as tolerated in the PTB cast promotes fracture healing through the principle of functional bracing (Sarmiento).
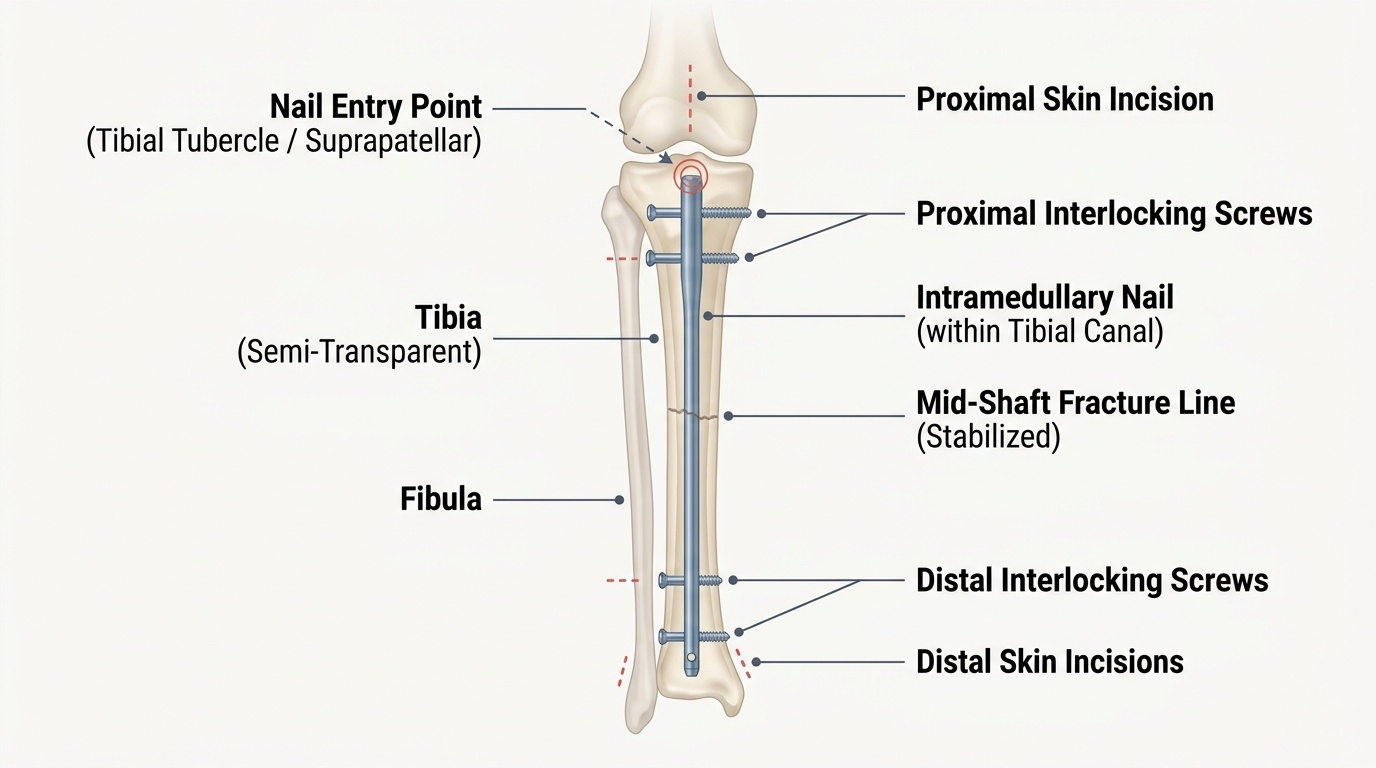
Operative management is indicated for: displaced fractures, open fractures, polytrauma, bilateral leg fractures, compartment syndrome, and failure of closed reduction. The intramedullary nail (IMN) is the standard definitive treatment for displaced tibial shaft fractures — it provides rotational and length stability, allows early weight-bearing, and has a low infection rate for closed fractures. External fixation is the initial treatment of choice for Grade IIIB/IIIC open fractures when soft tissue contamination or vascular repair dictates temporising fixation before wound closure. Plating is used for fractures involving the proximal or distal metaphysis-diaphysis junction where the nail cannot achieve adequate fixation.
For open fractures: emergency antibiotics within 1 hour of injury (current evidence supports early antibiotic administration as the single most effective measure against infection; the 'old 6-hour rule' for debridement is obsolete — debridement should occur as soon as safely feasible), tetanus prophylaxis, thorough wound debridement, and fracture stabilisation.
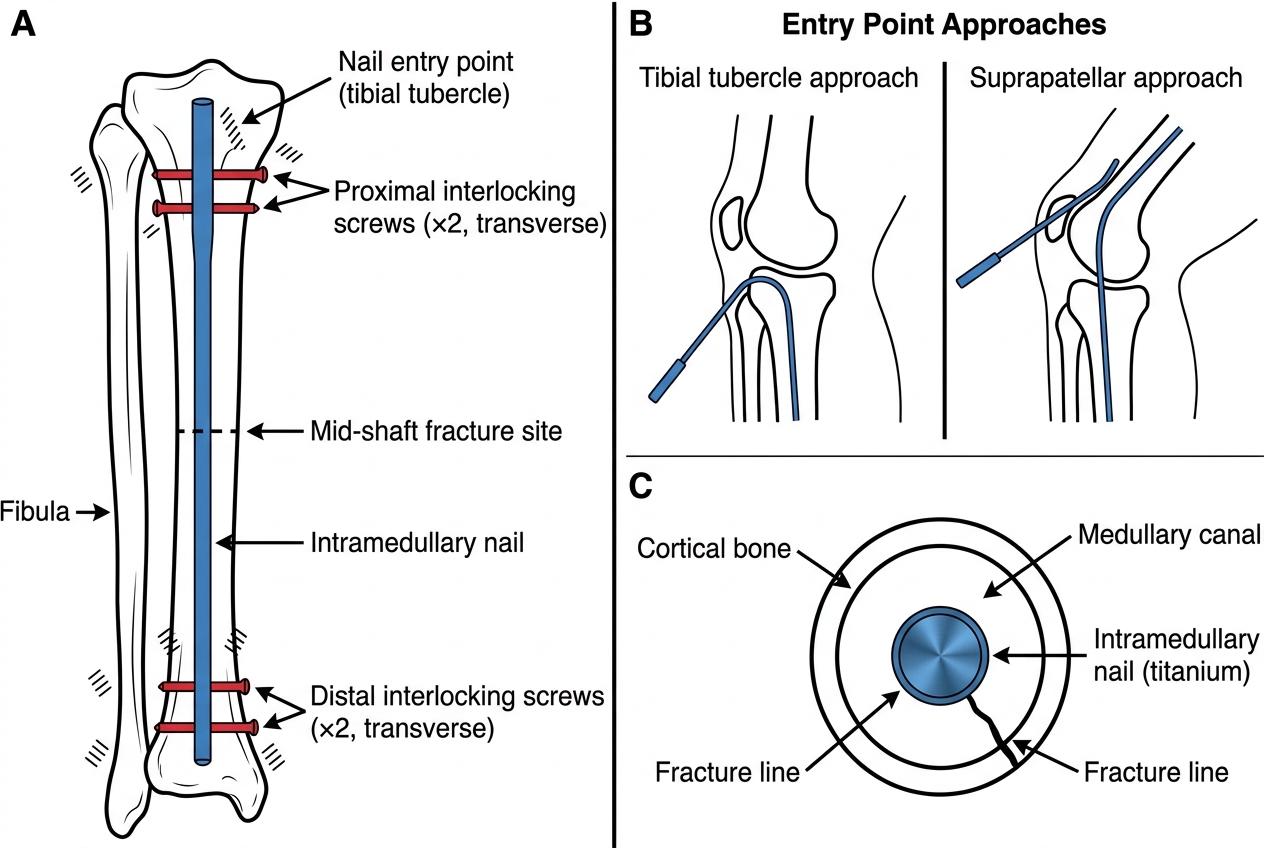
Intramedullary Nail Fixation of Tibial Shaft Fracture
SELF-CHECK
A 30-year-old construction worker sustains an open tibial shaft fracture with a 12 cm wound, periosteal stripping over 8 cm, and necrotic muscle edges visible in the wound, but radial pulses (anterior tibial and posterior tibial) are palpable. According to the Gustilo-Anderson classification, what grade is this fracture?
A. Grade I
B. Grade II
C. Grade IIIA
D. Grade IIIB
Reveal Answer
Answer: D. Grade IIIB
Grade IIIB is characterised by a wound >10 cm (this is 12 cm), periosteal stripping, inadequate soft tissue cover requiring local or free flap reconstruction, but no vascular injury requiring repair. Grade IIIC adds arterial injury requiring repair. Grade IIIA has adequate soft tissue cover despite extensive contamination. This patient's wound with periosteal stripping and necrotic muscle, but no vascular injury, is Grade IIIB.
Calcaneus Fractures — Mechanism, Bohler's Angle, and Management
The calcaneus is the largest bone of the foot and the most commonly fractured tarsal bone, accounting for approximately 60% of all tarsal fractures. The classic mechanism is a fall from height landing on the heel — a high-energy axial compression that drives the lateral process of the talus into the posterior facet of the calcaneus like a wedge, producing an intra-articular fracture with depression of the posterior facet. The body of the calcaneus flattens, widens laterally, and loses height — a pattern captured by the reduction in Bohler's angle.
Bohler's angle is a critical radiographic measurement on the lateral calcaneus view: it is the angle formed between two lines — one from the highest point of the anterior process to the highest point of the posterior facet, and another from the highest point of the posterior facet to the superior border of the posterior tuberosity. Normal range: 20–40°. In a comminuted intra-articular calcaneus fracture, this angle is reduced (often to 0° or even negative values), reflecting posterior facet depression. A Bohler's angle <20° reliably indicates significant articular involvement.
The Sanders classification (based on CT coronal images of the posterior facet) is the standard for operative planning: Type I = non-displaced; Type II = two-part fracture of the posterior facet; Type III = three-part; Type IV = four-part, highly comminuted. Types II and III are typically managed operatively in young, active patients; Type IV may require primary subtalar arthrodesis given the severity of articular destruction.
Extra-articular calcaneus fractures (avulsion of the posterior tuberosity by the Achilles tendon, fractures of the anterior process) have better prognosis and are more often managed non-operatively.
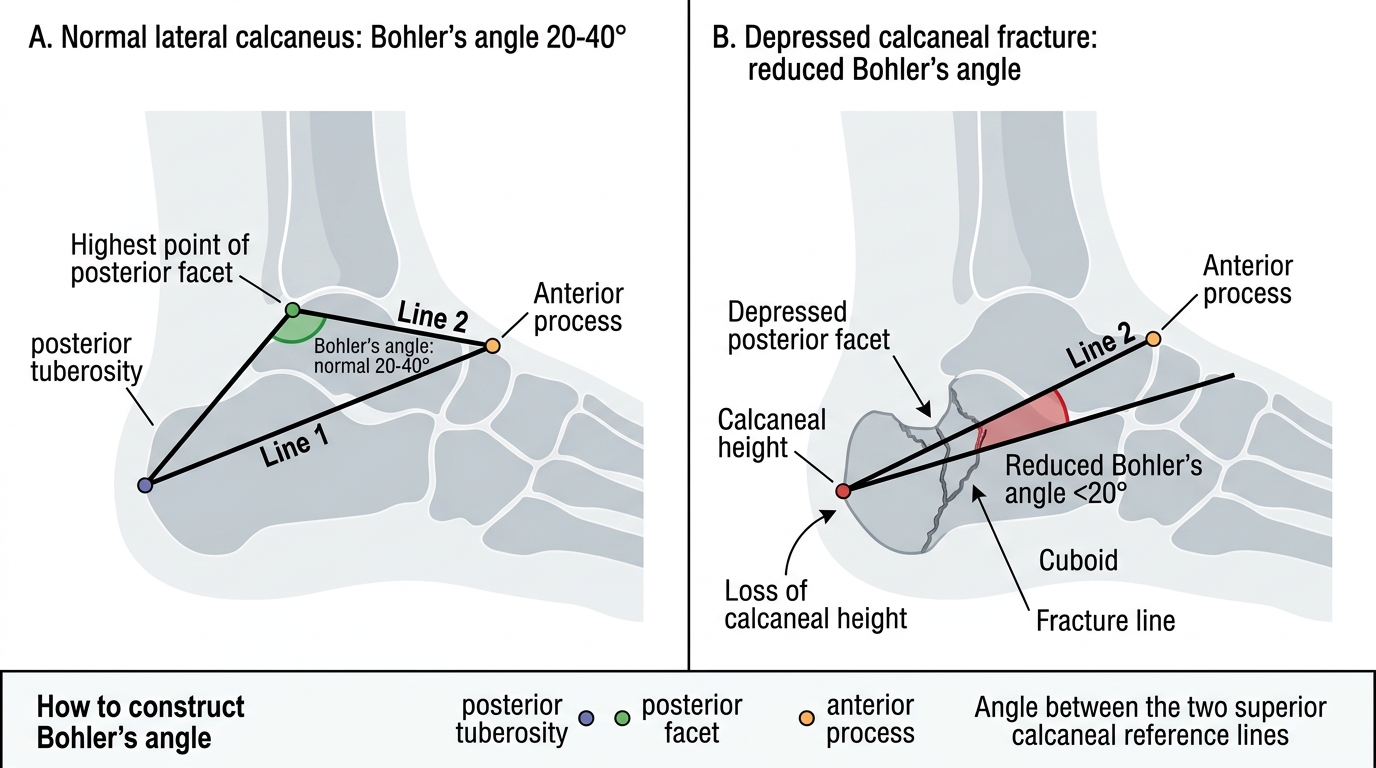
Bohler's Angle in Normal and Fractured Calcaneus