Page 7 of 22
OR2.12 | Leg and Foot Fracture Management — SDL Guide (Part 3)
Lisfranc Management and Outcomes
Provided image
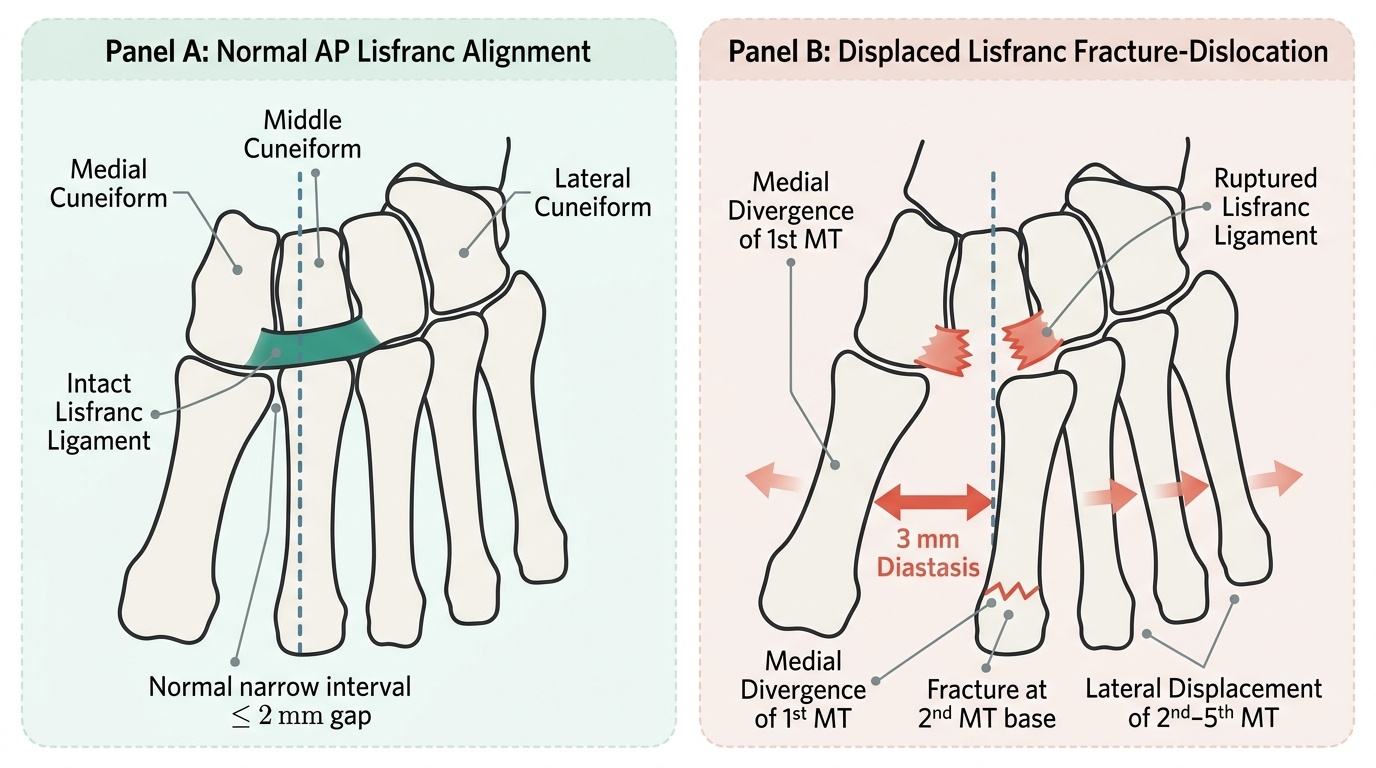
The management of Lisfranc injuries is determined by the degree of displacement. Non-operative management (short-leg cast, strict non-weight-bearing for 6–8 weeks) is appropriate only for truly non-displaced, stable injuries confirmed on weight-bearing radiographs or CT — a minority of cases. Any displacement (>2 mm diastasis) or instability constitutes an operative indication.
Operative management: open reduction and internal fixation (ORIF) with lag screws across the tarsometatarsal joints is the standard approach for acute injuries. The principle is anatomic reduction of all displaced metatarsals under direct vision, confirmed with intraoperative fluoroscopy, and fixation with transarticular screws. The Lisfranc screw (from the medial cuneiform to the base of the second metatarsal) is the most important fixation point — it must restore and maintain the recessed position of the second metatarsal base. In low-energy ligamentous Lisfranc injuries (no associated fractures), a trend toward primary arthrodesis of the medial three TMT joints has shown superior long-term results in some studies, avoiding the post-traumatic arthritis that frequently follows ORIF of purely ligamentous injuries. The lateral two TMT joints are typically not fused, as they have greater mobile function.
Long-term outcomes: the most significant complication of missed or inadequately treated Lisfranc injuries is post-traumatic midfoot arthritis — painful collapse of the medial longitudinal arch, difficulty walking on uneven ground, and inability to return to sporting activities. This underscores why the diagnosis must not be missed in the emergency department. Late salvage with TMT arthrodesis is less satisfactory than primary anatomic reduction.
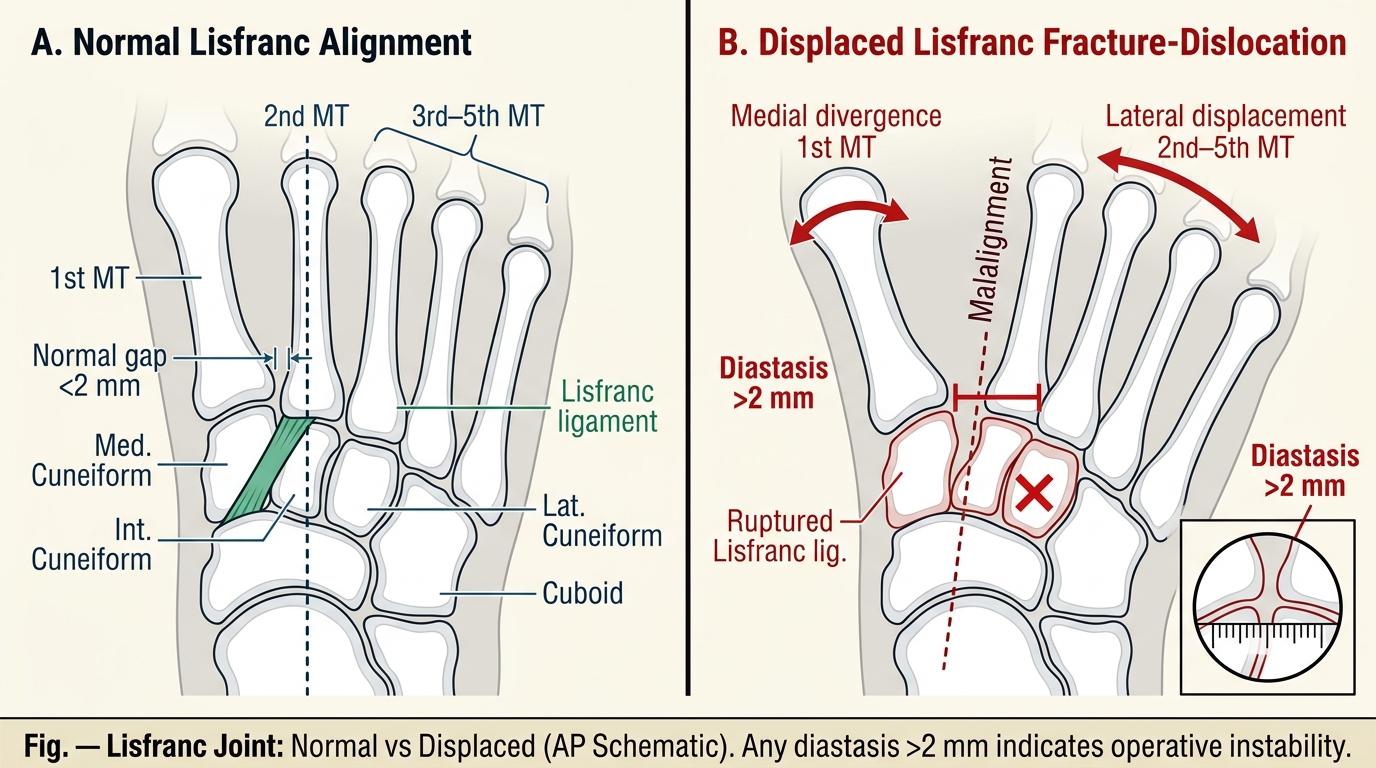
Lisfranc Joint: Normal Alignment vs Fracture-Dislocation (AP Schematic)
SELF-CHECK
A 22-year-old footballer twists his foot on a cleat and presents with midfoot pain, bruising on the sole of the foot, and inability to weight-bear. An AP radiograph shows a 3 mm gap between the bases of the first and second metatarsals. What is the most likely diagnosis and appropriate management?
A. Jones fracture of the fifth metatarsal; intramedullary screw fixation
B. Lisfranc fracture-dislocation; operative reduction and internal fixation
C. Mid-tarsal (Chopart) dislocation; closed reduction and plaster cast
D. Metatarsal stress fractures; activity restriction and protective shoe
Reveal Answer
Answer: B. Lisfranc fracture-dislocation; operative reduction and internal fixation
A 3 mm diastasis between the first and second metatarsal bases, combined with plantar ecchymosis and inability to weight-bear, is diagnostic of Lisfranc fracture-dislocation. Displacement >2 mm is an operative indication. ORIF with Lisfranc screw fixation restores TMT joint anatomy; failure to treat operatively results in post-traumatic midfoot arthritis and chronic disability.
Self-Assessment — Leg and Foot Fracture Management
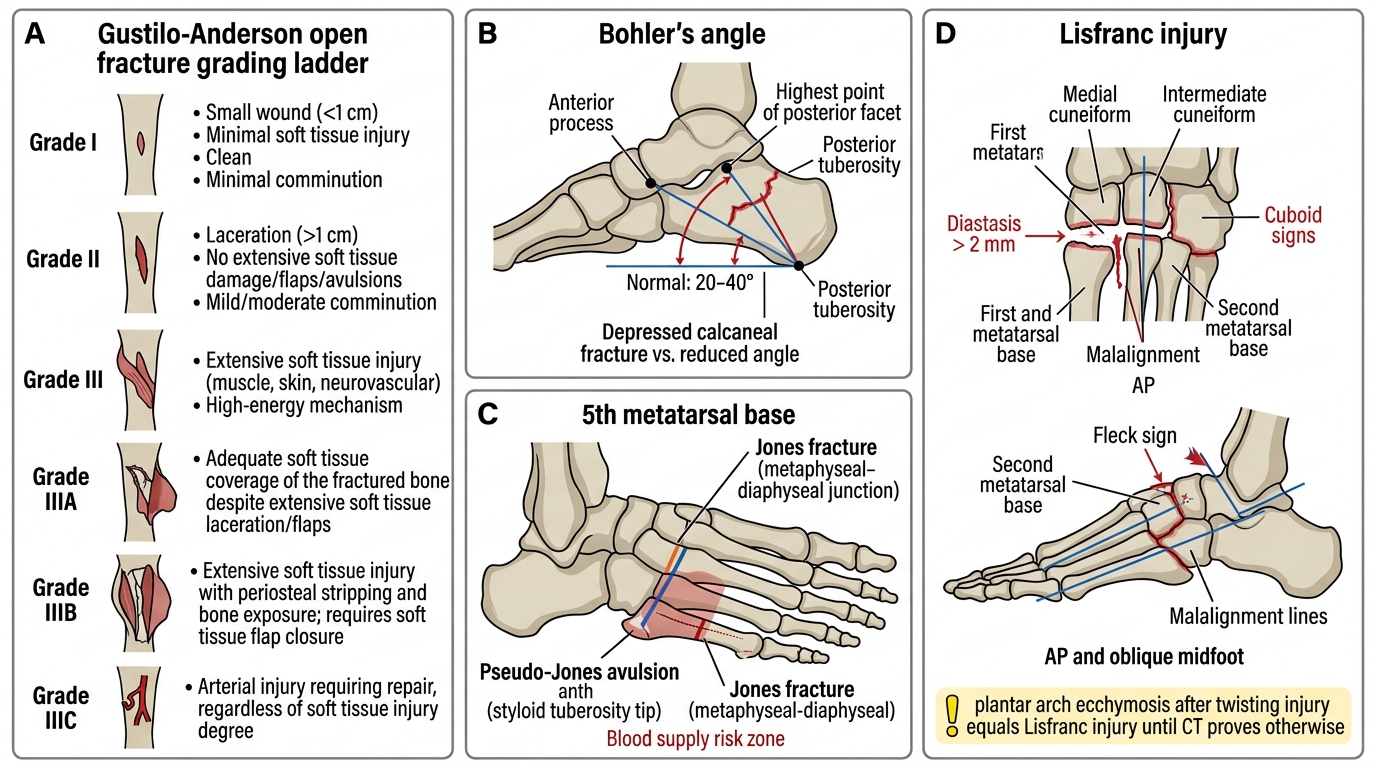
This self-assessment section is designed to verify your command of the key clinical concepts in leg and foot fracture management before you proceed to the clinical pearl and summary. Work through each prompt systematically. First, for both-bone leg fractures: apply the Gustilo-Anderson classification — what specific criteria distinguish Grade IIIA from Grade IIIB, and what is the single most important time-sensitive intervention for all open fractures regardless of grade? Second, for calcaneus fractures: draw Bohler's angle on a mental image of a lateral calcaneus X-ray — name the three bony landmarks, state the normal range, and explain what a value of 5° signifies for management. Third, for the fifth metatarsal: describe the radiographic feature that distinguishes a Jones fracture from a pseudo-Jones avulsion, explain the vascular basis for the Jones fracture's high non-union risk, and state the management difference. Fourth, for Lisfranc injury: name the three radiographic signs on a weight-bearing AP foot view that confirm the diagnosis, and state the management when diastasis exceeds 2 mm. Fifth, in a patient who falls from height onto both heels, name the two additional anatomical sites that must be radiographically evaluated before the patient leaves the emergency department.
Lower Limb Fracture Self-assessment Reference
CLINICAL PEARL
Two rules for foot fractures that prevent the most common missed diagnoses: (1) In any fall from height, always X-ray both heels (bilateral calcaneus fractures occur in 10–15%) AND the lumbar spine (L1/L2 compression fracture occurs in approximately 10%); (2) Plantar ecchymosis (bruising in the plantar arch) after a midfoot twisting injury is pathognomonic of Lisfranc ligament rupture — treat as a Lisfranc injury until CT proves otherwise. A Jones fracture (transverse fracture at the 5th metatarsal metaphyseal-diaphyseal junction) requires operative fixation due to poor blood supply and high non-union risk; do not confuse it with the benign pseudo-Jones avulsion at the styloid tip.