Page 1 of 22
OR2.10 | Patella and Peri-knee Fracture Management — SDL Guide
Learning Objectives
- Describe the mechanism of injury and classification of patellar, distal femur, and proximal tibia fractures
- Identify clinical signs of neurovascular compromise and compartment syndrome complicating peri-knee fractures
- Interpret plain radiographic findings and recognise when CT is indicated for peri-knee injuries
- Outline operative and non-operative management principles for fractures of the patella, distal femur, and tibial plateau
- Apply the 6 Ps of compartment syndrome monitoring and understand the threshold for emergency fasciotomy
INSTRUCTIONS
Fractures around the knee — the patella, distal femur, and proximal tibia — are high-energy injuries that frequently occur at the intersection of orthopaedic and vascular surgery. The popliteal artery runs in intimate proximity to the distal femur and proximal tibia, making neurovascular injury an ever-present risk. Compartment syndrome of the leg is one of the most limb-threatening complications in orthopaedics; recognising it early is a core skill for every MBBS graduate. This module grounds you in the anatomy, fracture patterns, and management principles you will need in any casualty or ward setting.
References
- Maheshwari's Essential Orthopaedics, Ch 29-30 (textbook)
- Apley & Solomon's System of Orthopaedics and Trauma, 10th ed, Ch 29 (textbook)
- Ebnezar's Textbook of Orthopaedics, 5th ed (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 32-year-old motorcyclist is brought to casualty after a head-on collision. His right knee is swollen, held in 20° flexion, and he cannot extend the leg against gravity. The skin over the anterior knee is intact but tense. Distal pulses are present, but he describes numbness down the outer aspect of his leg and cries out when you passively dorsiflex his ankle. Radiographs show a comminuted patellar fracture with a gap between fragments, and a subtle depression in the lateral tibial plateau. What immediate threat must you rule out before even discussing fracture fixation?
WHY THIS MATTERS
Peri-knee fractures are among the most consequential injuries you will encounter, not because the bone lesion itself is difficult to diagnose, but because the overlying and adjacent soft tissue structures — the extensor mechanism, popliteal vessels, peroneal nerve, and four closed muscle compartments of the leg — can be silently destroyed in the hours after injury. Missing compartment syndrome costs a limb. Missing a popliteal artery injury costs a life or a leg. Every student who rotates through any emergency department, orthopaedic ward, or rural hospital must be able to perform a focused neurovascular check, interpret the clinical signs of evolving compartment syndrome, and communicate with confidence to a senior surgeon.
RECALL
Before proceeding, recall the bony anatomy of the knee joint: the distal femur widens into medial and lateral condyles separated by the intercondylar notch; the proximal tibia presents medial and lateral plateaus separated by the tibial spines; the patella is a sesamoid bone within the quadriceps-patellar tendon-tibial tubercle extensor mechanism. The popliteal fossa contains the popliteal artery (a direct continuation of the femoral artery), the popliteal vein, and the bifurcation into anterior and posterior tibial arteries at the level of the tibial neck. The common peroneal nerve winds around the fibular neck, where it is vulnerable to traction and direct injury. The four compartments of the leg (anterior, lateral, deep posterior, superficial posterior) are enclosed by unyielding fascial sheaths, making the leg especially prone to compartment syndrome.
Fracture Patella — Mechanism, Pathology, and Extensor Disruption
The patella, the largest sesamoid bone in the body, is embedded within the quadriceps tendon superiorly and the patellar tendon inferiorly, forming the central pillar of the knee's extensor mechanism. Understanding the mechanism of injury is inseparable from understanding the resulting fracture pattern and — crucially — whether the extensor mechanism remains intact. There are two distinct injury vectors: a direct blow (dashboard injury, fall on the flexed knee), which tends to produce a comminuted or stellate fracture with partial preservation of the retinaculum; and an indirect tensile pull from a suddenly resisted quadriceps contraction (stumble, tripping on a step), which typically causes a transverse fracture with complete disruption of both the medial and lateral retinacula. The distinction matters profoundly for management: a comminuted direct-blow fracture with intact retinacula may still allow active knee extension, whereas a transverse tensile fracture almost always renders the extensor mechanism discontinuous.
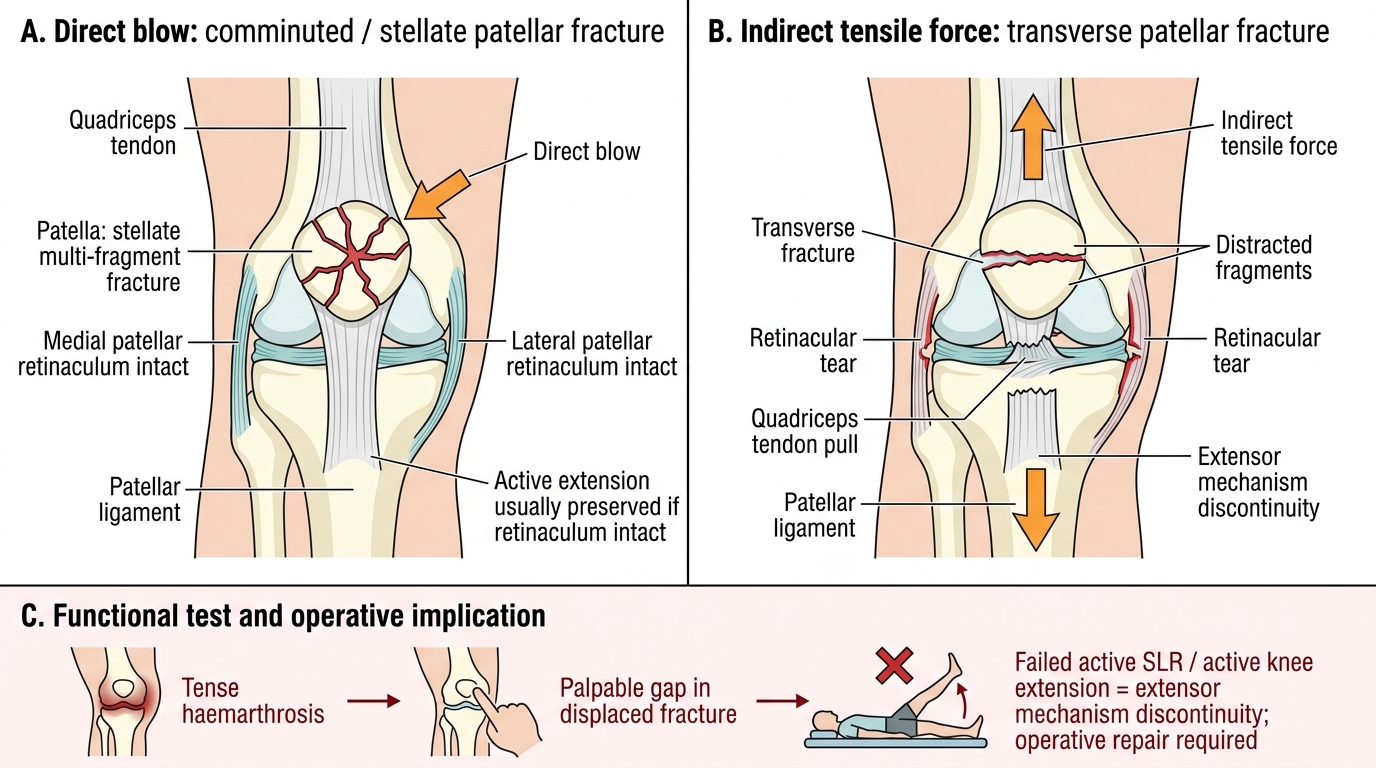
Patellar Fracture Patterns and Extensor Mechanism Continuity
Comminuted fractures (direct mechanism) are stellate or multi-fragmentary; if the retinaculum is intact, active extension is preserved. Transverse fractures (indirect mechanism) cross the mid-patella or upper third; displacement reflects retinacular tear. Vertical fractures are rare; the extensor mechanism is usually preserved. Avulsion fractures at the upper or lower pole indicate partial tendon avulsion.
Clinical presentation: the knee is swollen with a haemarthrosis, often visible as a tense effusion. In displaced fractures, a gap is palpable between fragments on the anterior patella. The cardinal test is active straight-leg raise (SLR) and attempted active knee extension against gravity — failure to extend or extend against gravity confirms extensor mechanism discontinuity and mandates operative repair.
Distal Femur Fractures — Classification and Neurovascular Risk
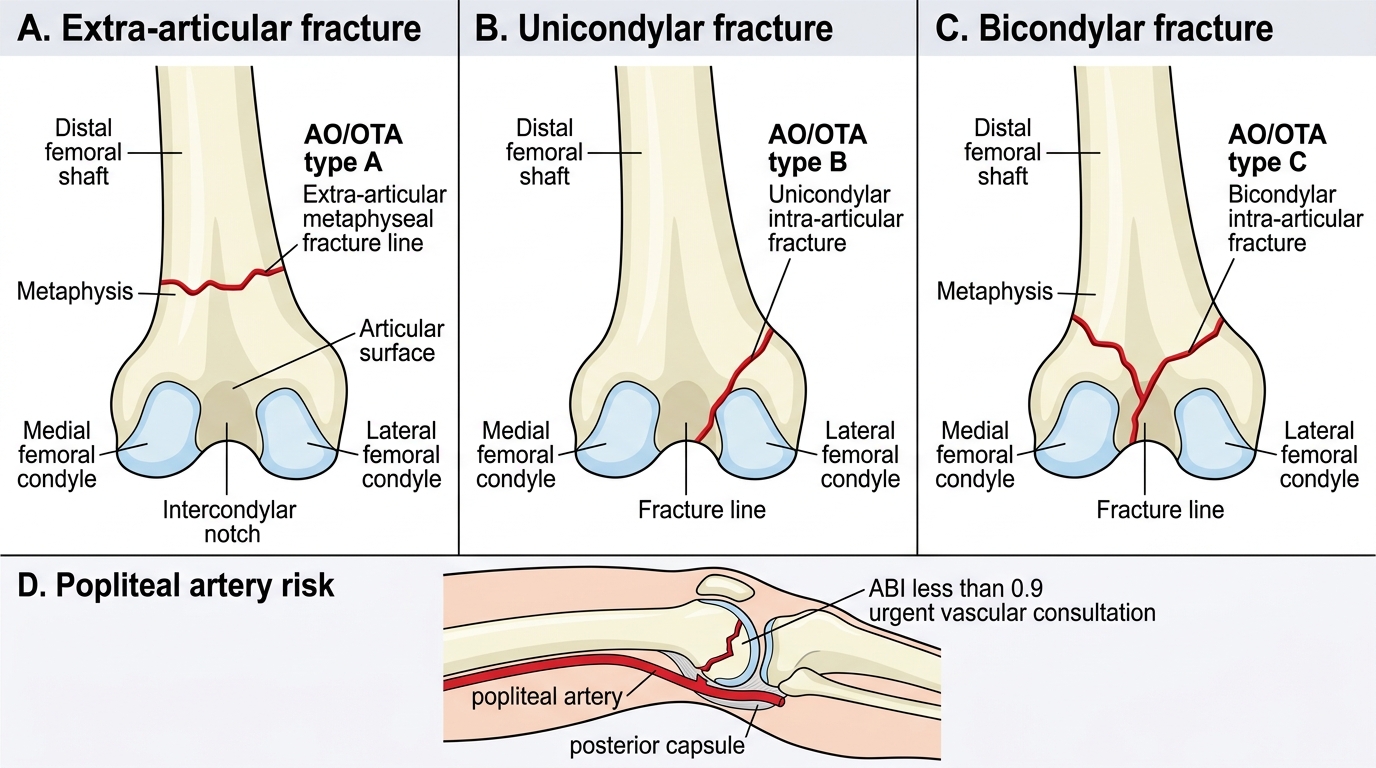
Distal femur fractures account for approximately 4–7% of all femoral fractures and are clinically significant injuries that arise from two distinct populations: high-energy mechanisms in young adults (road traffic accidents, falls from height) producing comminuted intra-articular fractures, and low-energy mechanisms in elderly osteoporotic individuals (simple falls) producing metaphyseal fractures. The distal femur comprises the metaphysis and the medial and lateral condyles; fractures may be entirely extra-articular (supracondylar), partially articular (unicondylar), or completely intra-articular (bicondylar T- or Y-type). The AO/OTA classification provides the standard framework: type A = extra-articular, type B = partial articular (unicondylar), type C = complete articular (bicondylar) — further subdivided 1/2/3 by degree of comminution. Type C fractures require restoration of both articular surfaces before any axial stability can be achieved.
AO/OTA Classification of Distal Femur Fractures
The most important neurovascular structure at risk is the popliteal artery, which is tethered at the adductor hiatus proximally and at the popliteal fossa distally; it is pulled anteriorly against the posterior capsule of the knee in hyperextension injuries. Posterior displacement of the distal fragment can directly lacerate or kink the artery. Doppler assessment of the dorsalis pedis and posterior tibial pulses, as well as the ankle-brachial index (ABI), is mandatory; an ABI <0.9 mandates urgent vascular surgery consultation. The common peroneal nerve may be stretched by valgus or rotational forces. Examination should document plantar and dorsiflexion strength, sensation in the first web space (deep peroneal territory), and lateral leg sensation (superficial peroneal).
SELF-CHECK
A 28-year-old man sustains a distal femur fracture after a road traffic accident. On examination, dorsalis pedis pulse is absent but the foot is warm and capillary refill is 3 seconds. The ankle-brachial index (ABI) is 0.75. What is the most appropriate immediate next step?
A. Immediate operative fixation of the femur fracture
B. Urgent vascular surgery consultation for suspected popliteal artery injury
C. Apply a above-knee plaster splint and reassess in 4 hours
D. MRI of the knee to assess ligamentous injury
Reveal Answer
Answer: B. Urgent vascular surgery consultation for suspected popliteal artery injury
An ABI <0.9 after knee-region trauma indicates likely arterial injury — in this case, probable popliteal artery injury. Vascular surgery must be involved immediately; the ischaemia window for limb salvage is typically 4–6 hours. Fracture fixation proceeds in coordination with vascular repair. Plastering and waiting would result in irreversible limb ischaemia.
Tibial Plateau Fractures — Schatzker Classification and Compartment Syndrome
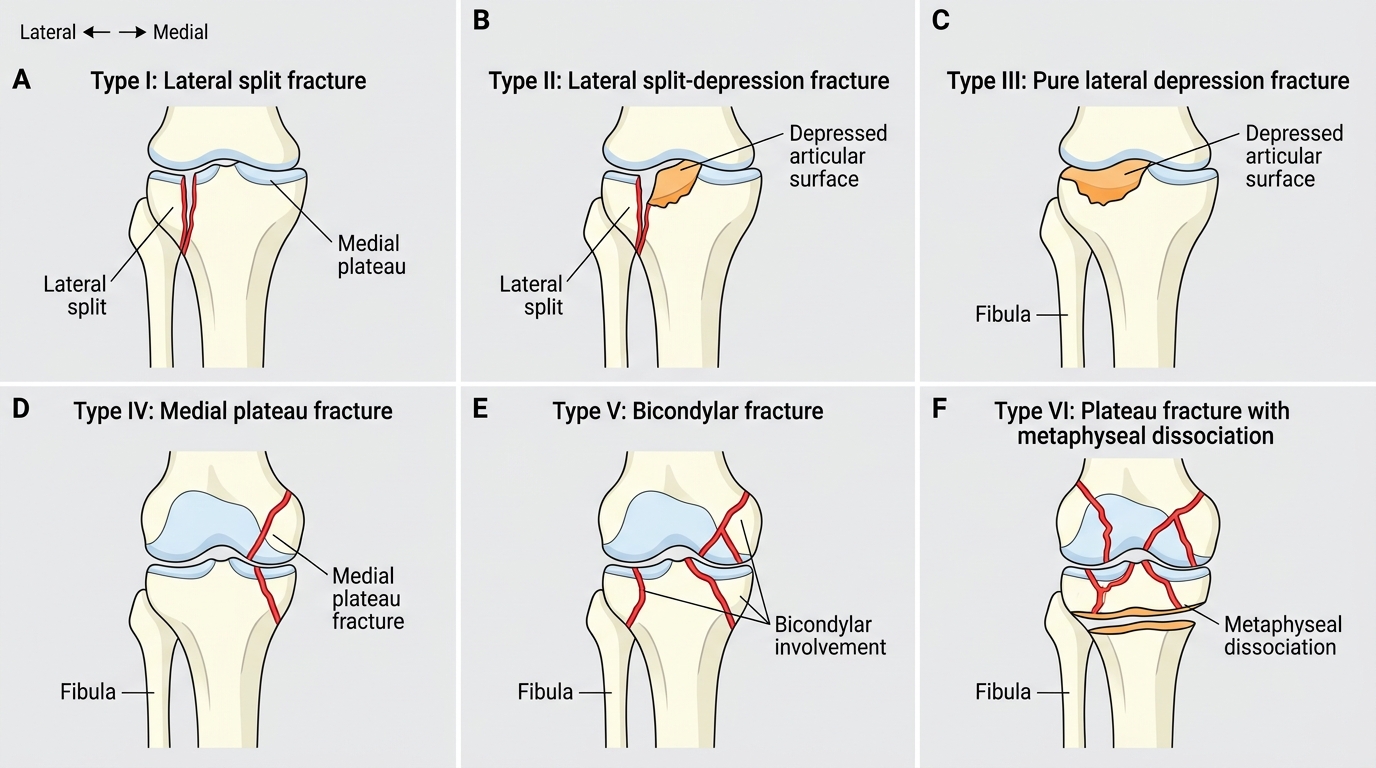
Tibial plateau fractures involve the proximal articular surface of the tibia and are produced by axial loading combined with a valgus or varus force — classically the 'bumper fracture' where the vehicle bumper strikes the lateral knee, driving the lateral femoral condyle into the lateral tibial plateau. The Schatzker classification (I–VI) is universally used and directly guides management: Type I = lateral split (young bone, no depression); Type II = lateral split-depression (most common, seen in middle-aged patients); Type III = pure lateral depression; Type IV = medial plateau fracture (associated with higher-energy, more comminution); Type V = bicondylar fracture; Type VI = bicondylar fracture with separation of diaphysis from metaphysis (highest energy, worst soft tissue injury). Types IV–VI carry significant risk of neurovascular compromise.
Schatzker Classification of Tibial Plateau Fractures
Compartment syndrome is the defining complication of proximal tibia fractures and tibial shaft injuries. The leg has four muscle compartments — anterior (tibialis anterior, extensor hallucis/digitorum, deep peroneal nerve, anterior tibial vessels), lateral (peroneus longus/brevis, superficial peroneal nerve), deep posterior (tibialis posterior, flexors, posterior tibial vessels, tibial nerve), and superficial posterior (gastrocnemius, soleus) — each enclosed in non-expansible fascia. When intra-compartmental pressure rises (from haemorrhage, oedema, or external compression), microvascular perfusion fails despite patent major vessels. The classic 6 Ps: Pain out of proportion to injury (earliest, most sensitive), Pain on passive stretch (highly specific — passively dorsiflex the toes: if anterior compartment pain is severe, compartment syndrome is likely), Paraesthesia (nerve ischaemia), Paralysis (late, motor ischaemia), Pallor, Pulselessness (very late — do not wait for absent pulses to diagnose compartment syndrome; pulses are often PRESENT until arterial occlusion pressure is reached).
Compartment pressure measurement: normal <10 mmHg; fasciotomy is indicated when measured compartment pressure exceeds 30 mmHg, or when the differential pressure (ΔP = diastolic BP − compartment pressure) is less than 30 mmHg. A four-compartment fasciotomy through two incisions (antero-lateral and postero-medial) is the definitive treatment.