Page 3 of 22
OR2.10 | Patella and Peri-knee Fracture Management — SDL Guide (Part 3)
Compartment Syndrome — Emergency Fasciotomy
Compartment syndrome of the leg is a surgical emergency; once the diagnosis is established clinically (or by pressure measurement ΔP <30 mmHg), fasciotomy must not be delayed by any other consideration, including fracture fixation. The operative approach for four-compartment fasciotomy of the leg uses two longitudinal incisions: an anterolateral incision (between the fibula and the tibial crest) that decompresses the anterior and lateral compartments through fascial releases; and a posteromedial incision (2 cm posterior to the tibial border) that decompresses both the deep and superficial posterior compartments. Both incisions are left open; the skin is loosely approximated or covered with a wound VAC. Delayed primary closure or split-thickness skin grafting is performed at 48–72 hours once swelling subsides.
The clinical rule that must be emphasised to every student: a palpable peripheral pulse does not exclude compartment syndrome. Pulses are lost only when compartment pressure exceeds systolic blood pressure — by which time irreversible myoneural ischaemia has occurred. The earliest and most sensitive clinical sign is pain out of proportion to the injury, particularly pain provoked by passive stretching of the muscles in the affected compartment. In an obtunded or intubated patient where clinical signs cannot be elicited, pressure monitoring is mandatory. Delayed fasciotomy (>6–8 hours) results in myonecrosis, contracture, renal failure from rhabdomyolysis, and permanent disability.
Self-Assessment — Peri-Knee Fractures
This section consolidates the key concepts from peri-knee fracture management into a structured self-assessment framework. Use the following questions to test your understanding before reviewing the micro-quizzes that appear earlier in this module. First, consider the extensor mechanism: can you name the three tests that confirm its integrity and state the threshold measurement that distinguishes operative from non-operative patellar fracture management? Second, for the distal femur, run through the AO/OTA A/B/C classification and identify which type mandates articular surface reconstruction before shaft fixation. Third, for the tibial plateau, list the Schatzker types in order and state the criteria (articular depression threshold, ligamentous instability) that shift management from non-operative to operative. Fourth, rehearse the 6 Ps of compartment syndrome in order of their temporal appearance during evolving ischaemia, and confirm your understanding of why a palpable pulse does not exclude the diagnosis. Fifth, state the fasciotomy threshold in terms of absolute compartment pressure and the differential pressure formula, and describe the two-incision approach for four-compartment decompression of the leg.
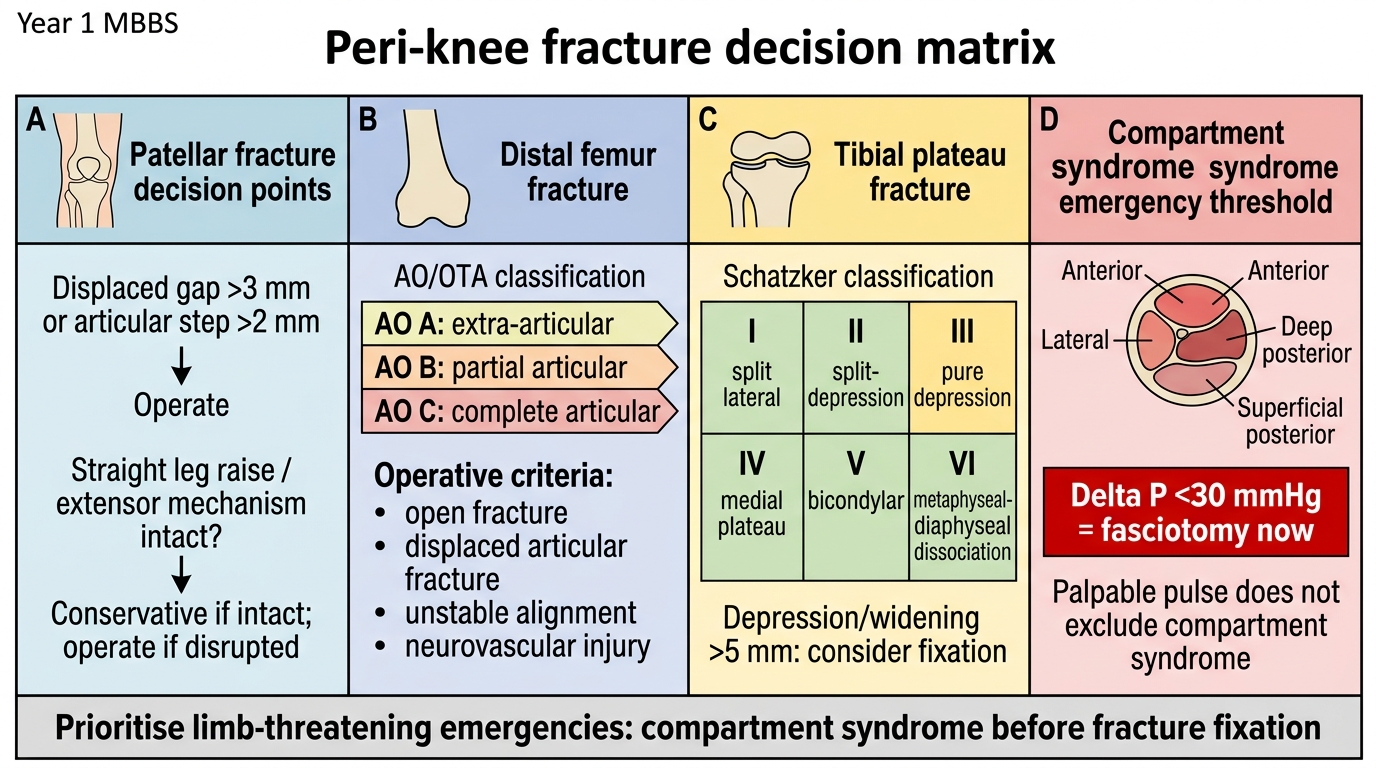
Peri-knee Fracture Decision Matrix
CLINICAL PEARL
Three rules to engrave for peri-knee fractures: (1) An absent dorsal pedis pulse after a distal femur or proximal tibia fracture is a vascular emergency — never wait for a pulse to return spontaneously. (2) Pain on passive stretch of muscles is the most reliable early sign of compartment syndrome — never be reassured by a present pulse in this context. (3) The Schatzker classification number directly predicts operative complexity: Types I–III may be managed with limited surgery, but Type VI distal femur is high-energy and often requires staged damage-control orthopaedics before definitive ORIF.