Page 5 of 22
OR2.2 | Proximal Humerus Fracture Management — SDL Guide (Part 2)
Management
Management decisions for proximal humerus fractures require integration of fracture pattern (Neer classification), patient age and bone quality, functional demands, and associated injuries. The majority (~80%) are one-part fractures that are managed non-operatively: immobilisation in a collar-and-cuff or polysling for 3-4 weeks, followed by pendulum exercises starting at 1-2 weeks, and progressive active-assisted physiotherapy. Radiographic and clinical union expected by 6-8 weeks; shoulder stiffness is the main complication of prolonged immobilisation, so physiotherapy is commenced early.
For two-part fractures, operative treatment is considered for significantly displaced greater tuberosity fractures (>5 mm displacement -- the supraspinatus footprint is affected) and significantly displaced surgical neck fractures in active patients; valgus-impacted surgical neck fractures in the elderly are often managed non-operatively as the periosteum and blood supply are preserved. Operative options include closed reduction and percutaneous K-wire fixation, open reduction and proximal humeral locking plate fixation, or intramedullary nailing. The locking plate (PHILOS or equivalent) is currently the most common operative implant for displaced fractures in younger patients with adequate bone stock.
For three-part and four-part fractures: in young patients (<60 years, good bone quality), open reduction and internal fixation (ORIF) with a locking plate is preferred, accepting the AVN risk (13-34%) because preserving the native joint is the priority. In elderly patients (>65-70 years, osteoporotic bone, low functional demand), primary hemiarthroplasty (humeral head replacement) is preferred for four-part fractures and head-splitting fractures, as ORIF in this group has high rates of hardware failure, malunion, and AVN. For very active elderly patients, total shoulder arthroplasty or reverse total shoulder arthroplasty (RTSA) may be indicated. RTSA is specifically preferred when rotator cuff integrity is compromised, as its design does not depend on the rotator cuff for stability.
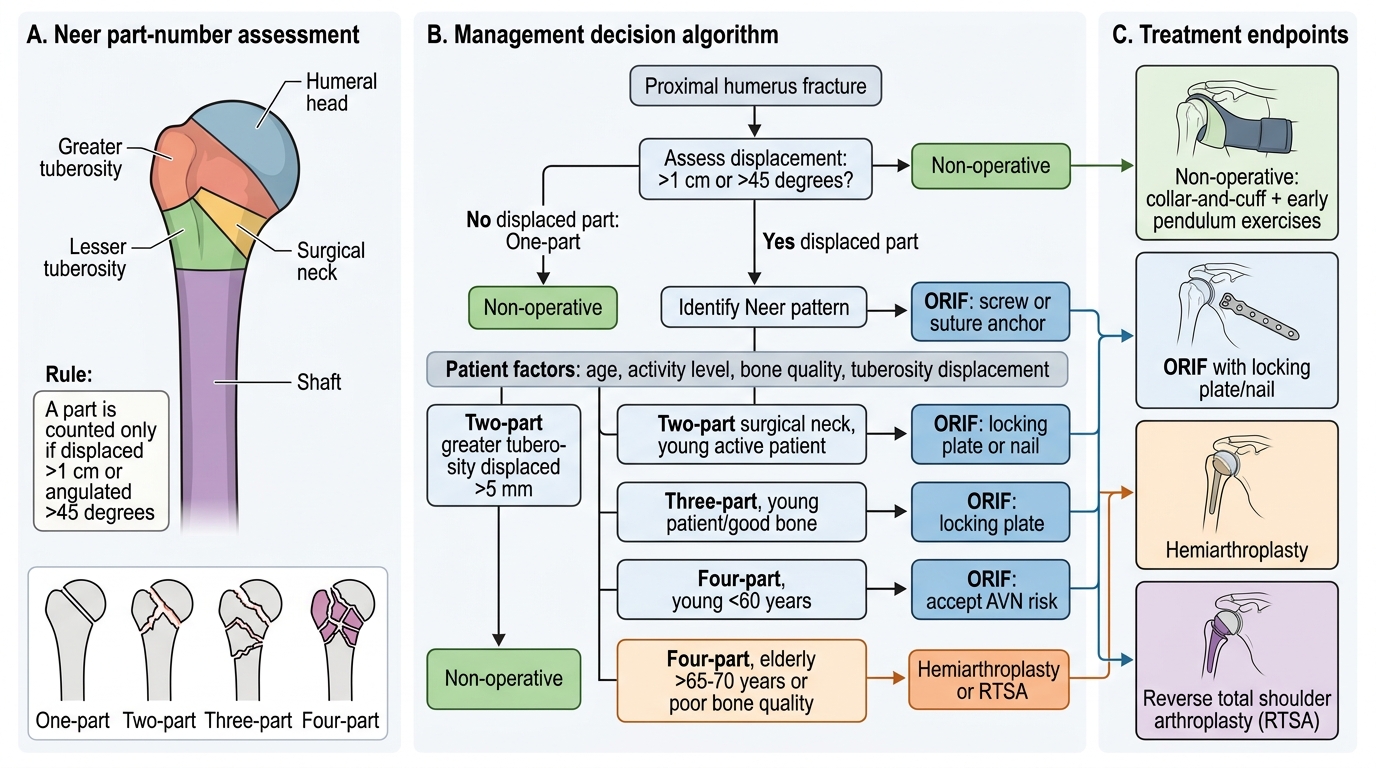
Proximal Humerus Fracture Management Algorithm
| Neer type | Management of choice |
|---|---|
| One-part (all types) | Non-operative: collar-and-cuff, early pendulum exercises |
| Two-part GT displaced >5 mm | ORIF (screw or suture anchor) |
| Two-part surgical neck, young active | ORIF (locking plate or nail) |
| Three-part, young | ORIF (locking plate) |
| Four-part, young (<60) | ORIF accepting AVN risk |
| Four-part, elderly (>65-70) | Hemiarthroplasty / RTSA |
Self-Assessment: Clinical Scenarios
Test your understanding with the following structured scenarios. In each case, determine the Neer classification, identify the nerve at risk, and outline the management.
Scenario A: A 68-year-old woman with osteoporosis falls at home. X-ray shows a proximal humerus fracture with no segment displaced more than 1 cm or 45 degrees. She has full sensation over the regimental badge area and can contract the deltoid. The Neer classification is one-part (no segment displaced). Management: non-operative -- collar-and-cuff for 3 weeks, pendulum exercises from week 1, progressive physiotherapy. Axillary nerve intact.
Scenario B: A 40-year-old manual worker is thrown from a motorbike. X-ray and CT show all four Neer segments displaced with a comminuted articular head. Regimental badge area is anaesthetic. Neer classification: four-part. Nerve: axillary nerve (neuropraxia probable, document and monitor). Management: young patient with high functional demand -- ORIF with locking plate accepting 13-34% AVN risk; neurology review for axillary nerve; physiotherapy post-fixation.
Scenario C: A 78-year-old retired school teacher has a four-part proximal humerus fracture with marked osteoporosis. She wishes to return to independent living. Management: given age, osteoporotic bone, and functional aspirations -- reverse total shoulder arthroplasty is preferred over ORIF (hardware failure and AVN risk are high in this group) and over hemiarthroplasty (RTSA gives better functional outcomes when rotator cuff quality is uncertain in elderly patients).
Key self-check points:
1. Name the nerve that must always be tested in proximal humerus fractures and its cutaneous territory.
2. What is the AVN risk in Neer four-part fractures?
3. In an 80-year-old with a four-part fracture, which operative option is now preferred over hemiarthroplasty and why?
CLINICAL PEARL
The regimental badge area test is non-negotiable before and after every proximal humerus fracture reduction or fixation. A missed pre-operative axillary nerve palsy that is documented post-operatively creates significant medico-legal risk. Most post-traumatic axillary nerve palsies are neuropraxias -- test monthly for recovery (deltoid contraction and sensation return by 3 months in most cases). If no recovery by 6 months, refer for electromyography and nerve conduction studies.
SELF-CHECK
When testing for axillary nerve injury in a patient with a proximal humerus fracture, which clinical test is most reliable?
A. Sensation over the entire outer arm down to the elbow
B. Sensation over the regimental badge area (lateral deltoid, 2 finger-breadths below acromion) and palpation of deltoid contraction
C. Power of wrist extension
D. Biceps reflex
Reveal Answer
Answer: B. Sensation over the regimental badge area (lateral deltoid, 2 finger-breadths below acromion) and palpation of deltoid contraction
The axillary nerve innervates the deltoid (motor) and the skin over the lateral deltoid -- the regimental badge area, approximately 4 cm in diameter, two finger-breadths below the acromion. This combined motor-sensory test is the bedside standard. Wrist extension tests the radial nerve (radial groove of humerus, not at risk here); the biceps reflex tests C5-C6 via the musculocutaneous nerve.