Page 2 of 20
OR3.1 | Bone and Joint Infection Assessment — SDL Guide (Part 2)
Chronic Osteomyelitis: Sequestrum, Involucrum, and Sinus Tracts
Chronic osteomyelitis develops when acute osteomyelitis is inadequately treated or when there is devascularised cortical bone that cannot be sterilised by antibiotics. The pathological hallmarks are uniquely orthopaedic and must be understood precisely because they determine the surgical strategy.
A sequestrum is a piece of dead, avascular cortical bone that has been separated from its blood supply by the infection-driven inflammatory process. The mechanism: pus accumulates beneath the periosteum and within the medullary canal, stripping the periosteum from the cortex (depriving it of periosteal blood supply) and simultaneously increasing endosteal pressure (reducing medullary blood supply). The cortex between these two devascularised zones undergoes ischaemic necrosis, forming the sequestrum. The sequestrum is characteristically radiodense (denser than the adjacent living bone) because the dead bone cannot undergo the resorption that living bone undergoes in the inflammatory environment. The sequestrum is effectively a nidus of infection — bacteria living within the dead bone are inaccessible to antibiotics (which require a blood supply to reach their target) and to immune cells. This is the fundamental reason why chronic osteomyelitis cannot be cured with antibiotics alone.
Surrounding the sequestrum, the elevated periosteum lays down a new shell of reactive bone — this is the involucrum. The involucrum is a hallmark of the body's reparative attempt, and its presence radiographically indicates a chronic or healing infection. The involucrum has small perforations called cloacae, through which pus and small fragments of sequestrum may discharge via sinus tracts to the skin surface. A discharging sinus is the classic clinical marker of chronic osteomyelitis.
Clinically, chronic osteomyelitis presents with recurrent episodes of pain, erythema, and purulent discharge from a sinus tract, often over months to years. There may be a history of previous acute infection, trauma, or surgery. Long-standing chronic osteomyelitis can occasionally undergo malignant transformation to squamous cell carcinoma of the sinus tract (Marjolin's ulcer), a late but important complication.
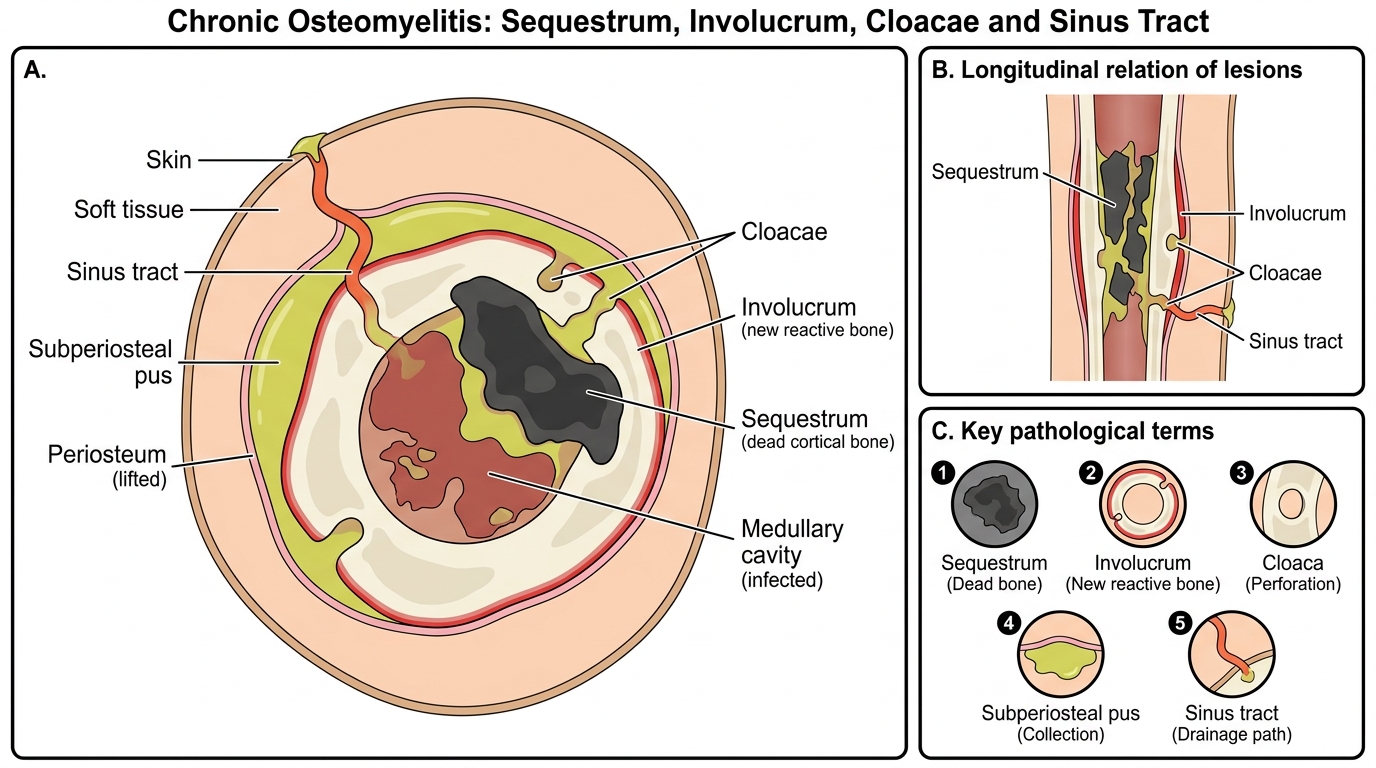
Chronic Osteomyelitis of a Long Bone
Investigations: Laboratory and Imaging
A systematic investigation approach is essential to confirm the diagnosis, identify the causative organism, and assess the extent of infection. The erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) are the most sensitive inflammatory markers — CRP rises within 6 hours of infection onset and is a better acute-phase marker than ESR, which takes 24-48 hours to peak. A white cell count >15,000/μL with neutrophilia supports bacterial infection but is non-specific. Blood cultures must be obtained before antibiotics are started and are positive in approximately 50-60% of cases — this yield is highest in the first 48 hours and drops rapidly once antibiotics are administered. When blood cultures are negative, bone aspiration or biopsy provides the most definitive microbiological diagnosis.
Plain radiographs are the first imaging investigation. In the first 7-10 days of acute osteomyelitis, the plain radiograph is typically normal or shows only soft-tissue swelling — bone destruction requires loss of approximately 30-50% of bone mineral and therefore takes at least one to two weeks to become radiographically visible. After 10-14 days, periosteal reaction (a thin shell of new bone laid down by the elevated periosteum) and lytic areas in the metaphysis may appear. The key teaching point is that a normal radiograph does NOT exclude early osteomyelitis.
Bone scintigraphy (technetium-99m MDP scan) can detect osteomyelitis within 24-48 hours of onset, before radiographic changes appear. It has high sensitivity (approximately 90%) but limited specificity — fractures, tumours, and bone infarcts also show increased uptake. It remains useful when MRI is not available.
MRI is now the gold standard investigation for acute osteomyelitis when the diagnosis is in doubt. It shows medullary oedema (decreased T1, increased T2 signal), subperiosteal collections, soft-tissue extension, and abscess formation with remarkable sensitivity (>97%) — and it does so within days of infection onset. MRI is particularly valuable for delineating the extent of disease to guide surgical drainage.
Ultrasound is a bedside tool for detecting subperiosteal abscess — a hypoechoic collection lifting the periosteum from the cortex — and can guide aspiration or drainage.
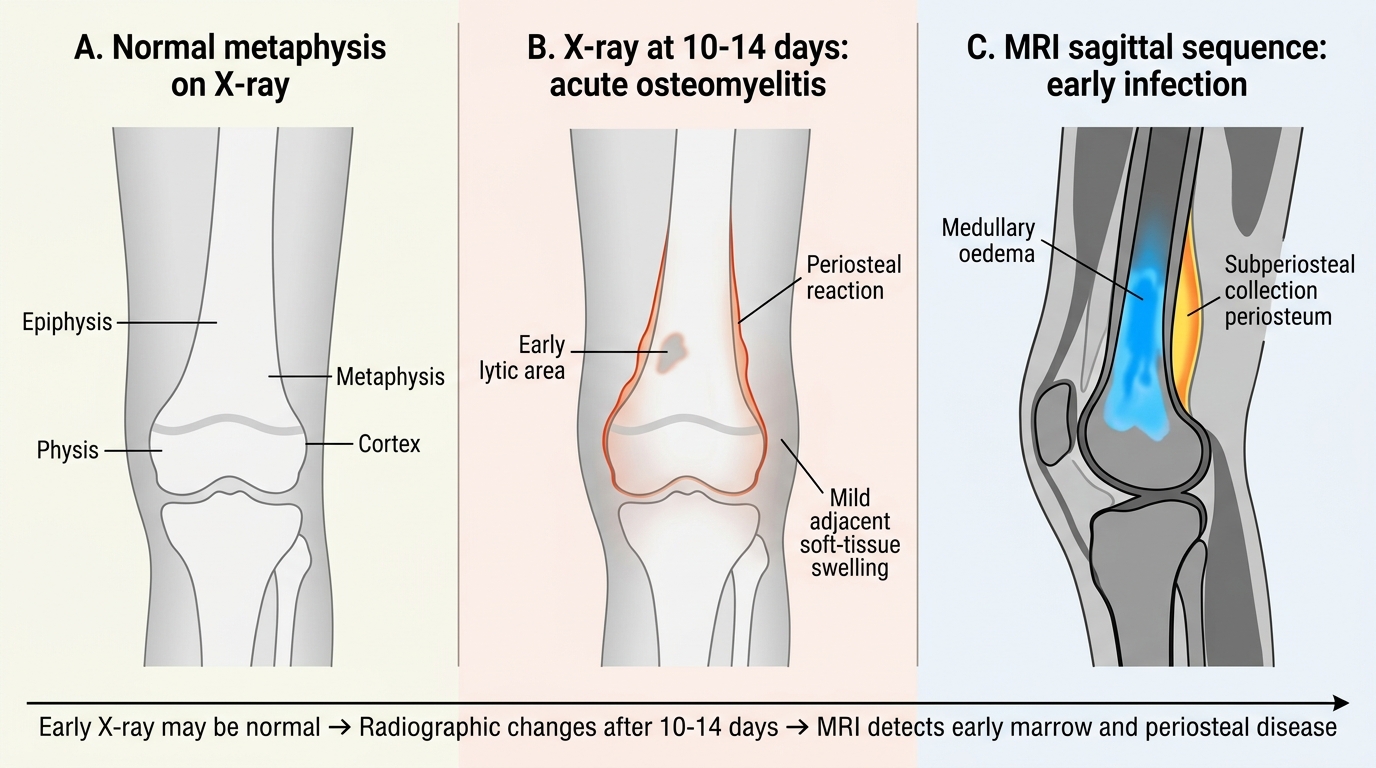
Imaging Evolution in Acute Osteomyelitis
SELF-CHECK
A 7-year-old with 3 days of fever and right knee pain has a plain X-ray reported as normal. What is the correct interpretation?
A. Osteomyelitis is excluded because the X-ray is normal
B. Plain X-ray is insensitive in the first 7-10 days; MRI or bone scan should be obtained if clinical suspicion is high
C. The child has septic arthritis, not osteomyelitis, because only soft-tissue swelling is seen
D. A normal X-ray at 3 days rules out bacterial infection — the fever must be viral
Reveal Answer
Answer: B. Plain X-ray is insensitive in the first 7-10 days; MRI or bone scan should be obtained if clinical suspicion is high
Plain radiographic changes of osteomyelitis (periosteal reaction, lytic areas) require 10-14 days to appear because 30-50% of bone mineral must be lost before radiographic visibility. A normal X-ray in the first week does NOT exclude osteomyelitis. MRI is the gold standard early imaging investigation.
Principles of Management: Acute Osteomyelitis
The management of acute osteomyelitis pivots on a single principle: the earlier treatment is started, the better the outcome. The goals are to eradicate infection, prevent progression to chronic osteomyelitis, and preserve bone and joint function. Management is either non-operative (antibiotics alone) or operative (antibiotics plus surgical drainage), depending on the stage and presence of abscess formation.
Antibiotic therapy should be started immediately after blood cultures are taken. The empirical antibiotic choice targets the most likely organism — in children and adults, this is S. aureus, so empirical treatment begins with an anti-staphylococcal penicillin (cloxacillin/flucloxacillin) or a first-generation cephalosporin (cefazolin). In suspected methicillin-resistant S. aureus (MRSA) infections, vancomycin is the empirical choice. When the blood culture or aspirate identifies the organism, antibiotics are de-escalated to the narrowest effective agent. The duration of antibiotic therapy has evolved: intravenous antibiotics for 2-5 days once clinical improvement occurs (fever resolving, CRP falling), followed by oral antibiotics for 3-6 weeks total is now supported by high-quality evidence. The old dogma of prolonged IV antibiotics for weeks is no longer recommended.
Surgical drainage is indicated when: (1) there is evidence of a subperiosteal or soft-tissue abscess, (2) there is no clinical response to antibiotics within 36-48 hours, (3) the joint is involved (septic arthritis), or (4) neonatal osteomyelitis (because of the high risk of epiphyseal damage). The surgical approach involves incision and drainage, removal of pus, and thorough lavage. In established disease with intraosseous abscess, drilling of the metaphysis to release intraosseous pressure is performed.
The critical goal is to prevent transition to chronic osteomyelitis — once cortical necrosis and sequestrum formation occur, the disease enters a chronic phase that is far more difficult and costly to treat.
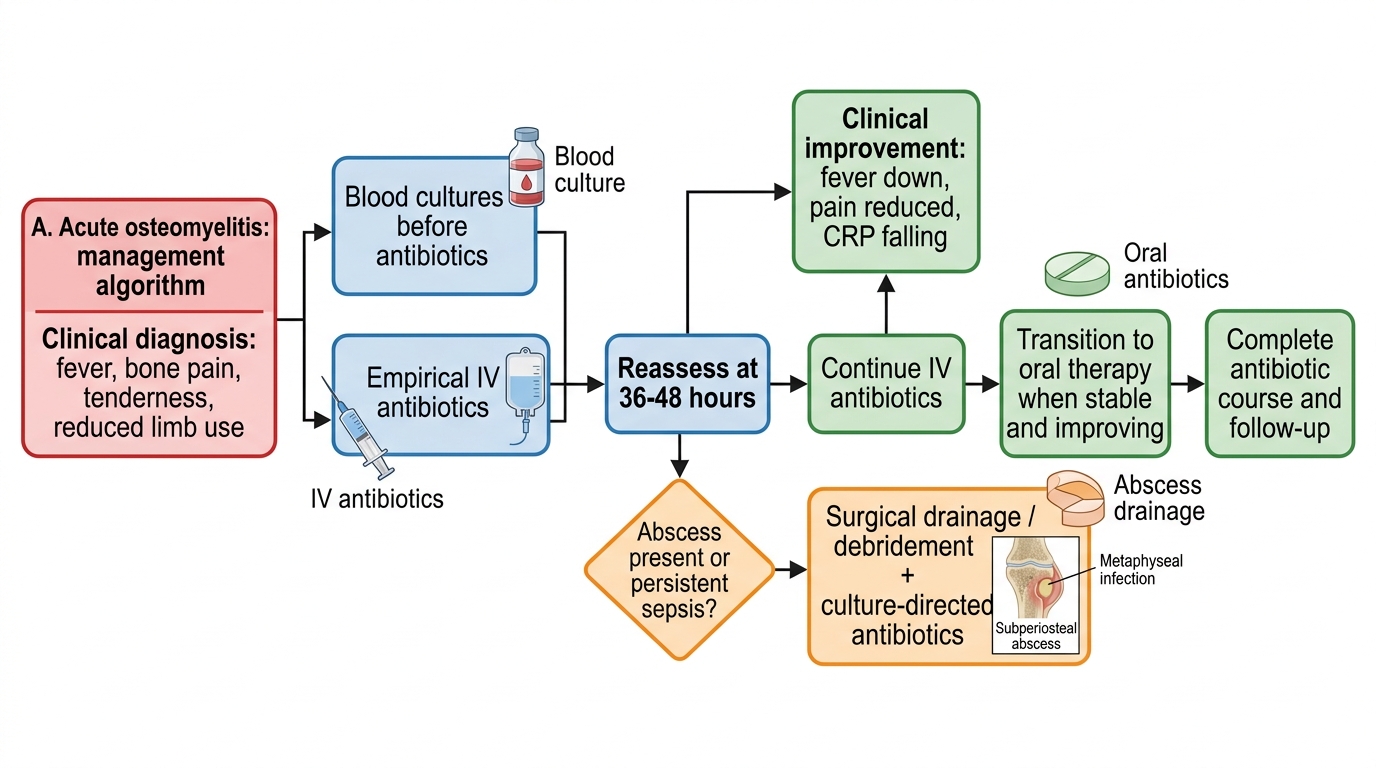
Acute Osteomyelitis Management Algorithm