Page 4 of 20
OR3.1 | Bone and Joint Infection Assessment — SDL Guide (Part 4)
Distinguishing Pyogenic from Tuberculous Musculoskeletal Infection
One of the most important clinical distinctions in musculoskeletal infection is between pyogenic (bacterial) infection and tuberculous bone and joint disease. In India, TB continues to be endemic, and skeletal TB — though accounting for only about 1-3% of all TB cases — represents a significant diagnostic challenge because its presentation overlaps with degenerative and neoplastic conditions. The key discriminating feature is tempo: pyogenic infection is acute (days), with fever, raised WBC, and elevated CRP; TB is indolent (months to years), with constitutional features (low-grade fever, night sweats, weight loss) and mildly elevated or normal acute-phase reactants. Recognition of this temporal contrast is clinically vital because the two conditions require entirely different treatment regimens: anti-staphylococcal antibiotics and surgical drainage for pyogenic disease versus anti-tubercular therapy (ATT) for 9-12 months for skeletal TB. Initiating inappropriate empirical antibiotics in TB osteomyelitis delays diagnosis and fosters drug resistance, while missing pyogenic septic arthritis and treating it as TB destroys the joint while the focus awaits culture results.
Further distinguishing features are summarised below:
| Feature | Pyogenic Osteomyelitis | Tuberculous Osteomyelitis |
|---|---|---|
| Onset | Acute (days-weeks) | Subacute/chronic (months) |
| Fever | High (>38.5°C) | Low-grade |
| WBC | Markedly elevated | Normal or mildly elevated |
| CRP/ESR | Markedly elevated | ESR elevated; CRP may be normal |
| Organism | S. aureus (most common) | M. tuberculosis |
| Radiograph | Lytic + periosteal reaction | Lytic, osteoporosis, little periosteal reaction |
| Cold abscess | Absent | Present (pathognomonic) |
| Sinus tract | Present in chronic disease | Present; typically discharges "rice bodies" |
| Site | Metaphysis of long bones | Spine (Pott's), hip, knee |
| Histology | Neutrophilic abscess | Caseating granuloma with Langhans' giant cells |
The cold abscess deserves special mention: in TB, the body forms an abscess filled with necrotic, cheesy (caseous) material but the vigorous acute inflammatory response (heat, redness) is ABSENT — hence "cold" abscess. In Pott's disease (TB spine), the cold abscess may track along fascial planes far from the vertebral lesion — a psoas abscess originating at the lower thoracic spine may present as a lump in the groin.
Diagnosis of skeletal TB requires bacteriological confirmation: Ziehl-Neelsen staining and culture of aspirated material, or biopsy with histopathology showing caseating granulomas. Nucleic acid amplification tests (GeneXpert MTB/RIF) have high sensitivity and specificity and can also detect rifampicin resistance. Anti-tubercular therapy (ATT: HRZE for 2 months then HR for 4 months, minimum 6-9 months for skeletal TB) is the cornerstone of treatment.
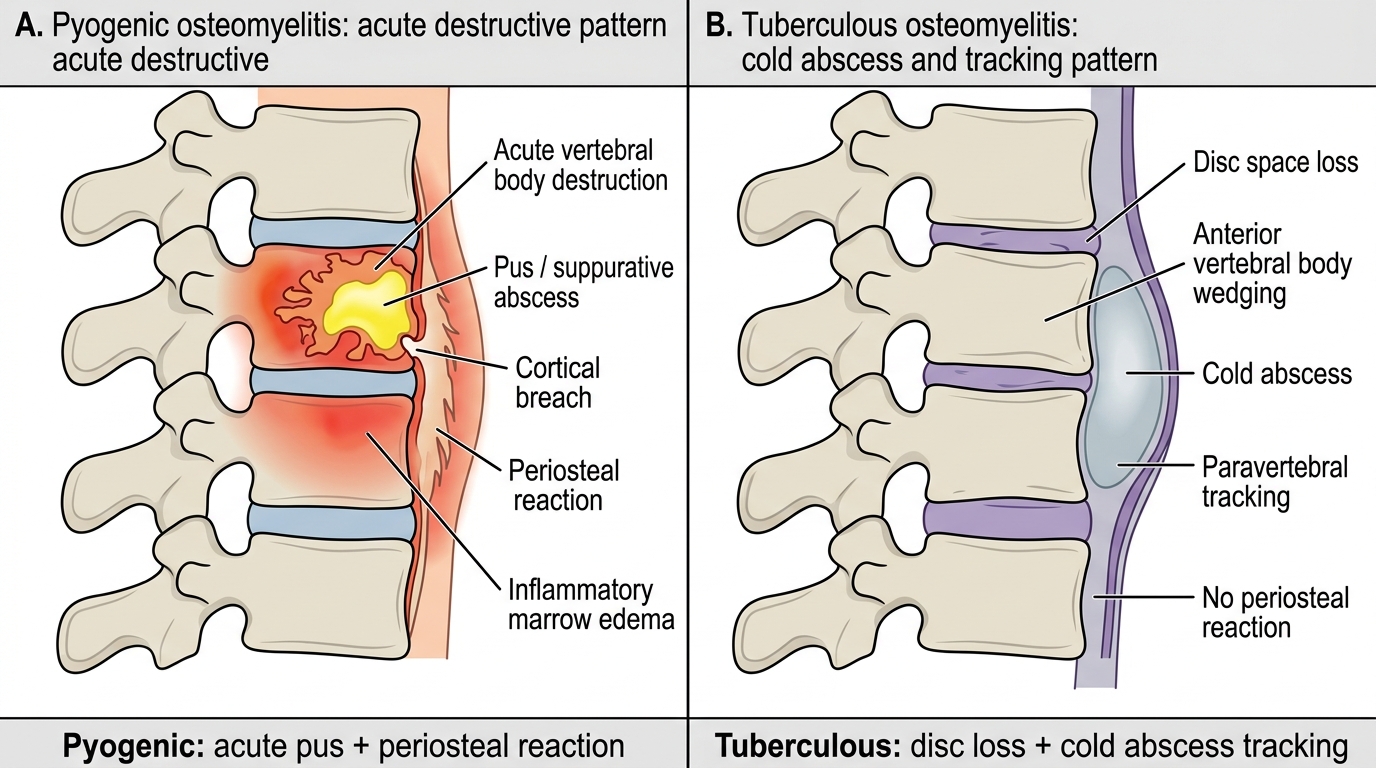
Pyogenic vs Tuberculous Vertebral Osteomyelitis
Self-Assessment: Applying the Diagnostic Framework
To consolidate your learning, work through the following self-assessment scenarios, applying the clinical, laboratory, and radiological framework developed in this module. Each scenario maps to a key discriminating principle.
For each case below, identify the most likely diagnosis, justify your answer by naming the discriminating features, and outline the immediate management steps. Compare your reasoning with the explanations provided.
Scenario A: A 12-year-old presents with 5 days of high fever (39.5°C), severe right distal femoral metaphyseal tenderness, WBC 19,000, CRP 160 mg/L. Plain X-ray is normal. What is the diagnosis, which investigation do you request next, and what do you start immediately?
Answer rationale: Acute haematogenous osteomyelitis. The normal X-ray at 5 days is expected (changes need 7-10 days). Order MRI to detect medullary oedema and subperiosteal abscess. Start blood cultures FIRST, then empirical IV cloxacillin/flucloxacillin. Arrange surgical drainage if MRI shows abscess or no clinical improvement at 36-48 h.
Scenario B: A 28-year-old presents with 8 months of intermittent right knee pain, a discharging sinus, weight loss of 6 kg, mild fever, ESR 80 mm/h, WBC 9,500, Mantoux +++, X-ray shows periarticular osteoporosis and joint space loss. What distinguishes this from pyogenic septic arthritis, and what is the critical diagnostic step?
Answer rationale: TB arthritis (indolent tempo, constitutional features, osteoporosis without periosteal reaction, positive Mantoux). Critical step: joint aspiration/synovial biopsy for ZN stain, culture (LJ medium for MTB), and histopathology (caseating granuloma with Langhans' giant cells). GeneXpert MTB/RIF if available. Do NOT start ATT without bacteriological confirmation where possible.
Scenario C: A 50-year-old with poorly controlled diabetes presents with recurrent discharge from a thigh sinus for 3 years. X-ray shows a dense bone fragment surrounded by a thick bony shell. CRP is 60 mg/L, WBC 13,000. What are the pathological structures named on X-ray, and why has medical treatment alone failed?
Answer rationale: Sequestrum (dense dead bone fragment) within an involucrum (reactive periosteal new bone shell). Medical treatment fails because the sequestrum is avascular — antibiotics cannot reach it. Sequestrectomy + saucerisation is mandatory. Diabetes (Cierny-Mader Host Grade B) increases the complexity of reconstruction.
SELF-CHECK
In chronic osteomyelitis with a visible sequestrum, why does prolonged antibiotic therapy alone fail to cure the infection?
A. The bacteria develop antibiotic resistance within days of starting treatment
B. The sequestrum is avascular dead bone — antibiotics require a blood supply to reach their target and cannot penetrate avascular tissue
C. The patient's immune response destroys the antibiotics before they reach the bone
D. Oral antibiotics are not absorbed adequately in orthopaedic infections
Reveal Answer
Answer: B. The sequestrum is avascular dead bone — antibiotics require a blood supply to reach their target and cannot penetrate avascular tissue
The sequestrum is a piece of dead, avascular cortical bone. Since antibiotics depend on the bloodstream to reach infected tissue, they cannot penetrate avascular dead bone. Surgical sequestrectomy is mandatory to physically remove the nidus of infection. This is the fundamental reason chronic osteomyelitis requires surgery, not just antibiotics.
CLINICAL PEARL
Three distinctions that trip up examinees and house officers alike: (1) Pulse is often present in early compartment syndrome — never reassure on a palpable pulse. Pain out of proportion and pain on passive stretch are the earliest and most reliable signs. A pulseless limb in compartment syndrome is already at the edge of irreversible ischaemia. (2) A normal X-ray does NOT exclude osteomyelitis in the first 7-10 days — get an MRI or bone scan when clinical suspicion is high. (3) 'Cold' in cold abscess means the absence of local heat and redness — not that the abscess is literally cold. The cold abscess is the hallmark of tuberculosis because TB provokes a granulomatous (not acute neutrophilic) inflammatory response; it may be fluctuant and large, but the overlying skin is NOT warm and erythematous.